


Review Article - (2019) Volume 4, Issue 4
Anorexia of The Female Adolescent: Biological Condition Different Blood Types (0,A,B,AB) Mother/Daughter Traumatic Blood Contact between the Two During Pregnancy and/or Birth. Psychological and Nutritional Causes and Treatment
Received Date: Jul 06, 2019 / Accepted Date: Jul 24, 2019 / Published Date: Sep 09, 2019
Copyright: ©Lorenzo Bracco. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Anorexia of the Female Adolescent begins within a limited period of time after menarche and it is characterized by weight loss and loss of menstrual cycle for more than three months. This anorexia is due by psychological and relational causes of the girl and her family. My new theory is that upstream of these causes the Anorexia of the Female Adolescent also requires a biological condition:
“Different Blood Types Mother/Daughter (0, A, B, AB)”. In my medical practice I found that all girls suffering from Anorexia of the Female Adolescent have different blood type from their mother. There are no exceptions in my data. With my new theory all physicians can make an early diagnosis because the group at risk of anorexia to be monitored is reduced to a small percentage of adolescent girls: only those with a blood type different from that of the mother. This will reduce mortality rate and also the consequences (osteoporosis and osteopenia) because late diagnosis is the main cause of therapy failure and of the high mortality rate. However, not all girls with different blood type than the mother develop the Anorexia of the Female Adolescent, but only a few. Why? My hypothesis is that in addition to the difference in the mother/daughter blood type there has been also a blood contact between the two, not necessarily detected, during pregnancy and/or at birth. Psychological and nutritional causes and treatment.
Keywords
Anorexia, Anorexia of the Female Adolescent, Blood Type, Adolescent, Trauma, Placental Trauma, Trauma Therapy, Blood Mismatch, Predictive Diagnosis, Early Diagnosis
Anorexia
Anorexia is an eating disorder in which the most serious cases can continue over a prolonged period of time and might involve the total rejection of all kinds of food.
In order to prevent and treat Anorexia Nervosa, we should distinguish between:
Anorexia Independent of Age and Sex (the form of anorexia that can arise at any age in both males and females) and
Anorexia of the Female Adolescent (anorexia that arises in the female during adolescence and can re-appear throughout the course of life). The Anorexia of the Female Adolescent is the prevalent and the most dangerous of the two.
Anorexia Independent of Age and Sex
This Anorexia may be a symptom or consequence of:
• Chemotherapy
• Some types of cancer
• Some diseases
• Some hormonal disorders
• Some obsessive behaviors
• Burnout
• Depression
To take care of this type of anorexia we must treat the causes or situations of which it is a symptom or a consequence.
There must also be a food re-education program because, after a long time of fasting and poor feeding times, the person has lost orientation in eating. The food re-education program must actively involve the person so that he/she not only acquires knowledge, but also adjusts his/her eating habits to a proper diet. To this purpose, it is necessary to involve the nutrition scientist in therapy.
Treatment of this type of anorexia requires the intervention of medical doctor and, very often, in parallel the intervention of psychotherapist. This is particularly true in the case with anorexia resulting from burnout and depression that frequently manifests itself after a period of extreme stress also during childhood, adolescence,adulthood in response to a failed attempt to seek acceptance within the family or the society. Depression can also manifest itself as a result of an experience of exclusion a person has suffered, like a separation from one’s family, divorce, work termination, retirement, etc…This depression can assume particularly serious aspects and can be cause of Eating Disorders. Most times these Eating Disorders take the form of an excessive consumption of food because a person seeks comfort and compensation for lack of affection. Other times, however, these Eating Disorders can involve an insufficient food intake, which can potentially develop into anorexia, expecially when an individual is so embittered that he or she no longer has the will to live. Usually this anorexia responds relatively well to pharmacological therapy, while Anorexia of the Female Adolescent doesn’t react to pharmacological therapy.
Anorexia of the Female Adolescent
Anorexia of the Female Adolescent (the prevalent and the most dangerous kind of anorexia) manifests precisely during the phase of a young woman’s blossoming femininity. There can also be relapses of this form of anorexia over the course of life. This kind of anorexia strikes societies and social classes where the variety and quantity of food can be abundant.
Anorexia of the Female Adolescent is characterized by:
• Extreme weight loss
• Interruption of the menstrual cycle for more than three months (this occurs in a period close to the first menstrual cycle, within a maximum of three years)
These first two facts are sufficient for the diagnosis of Anorexia of the Female Adolescent. Also usually there is:
• Loss of the female form (including shrinkage of breasts)
• Distorted perception of one’s own weight (which always seems excessive)
• The desire to undergo physical exertion beyond one’s capacity
• Refusal to recognize the gravity of the situation
There is a general agreement that the causes of Anorexia of the Female Adolescent are psychological and relational, connected with dysfunctional:
- Relationship with herself
- Mutual mother/daughter relationship
- Mutual father/daughter relationship
- Mutual relationship between the girl and the environment surrounding her
- Eating habits of the family
- Affective and emotional communication between family members.
My New Theory
In addition to all this, I have also identified a biological condition for Anorexia of the Female Adolescent: the blood type (0, A, B, AB) of the mother and the bloood type (0, A, B, AB) of the daughter are always different.
I am a medical doctor and a psychotherapist, and I have been interested in eating disorders since I started my career. I began to focus my attention especially on Anorexia of the Female Adolescent in response to an event that might seem curious, but that had the same effect on me as the apple did on Newton.
Twenty five years ago, I was visiting one of my patients, a 30-year-old woman at that time. She suffered from anorexia, which she had been experiencing off and on since her adolescence. Her fetal life and her birth had been constantly problematic: placenta abruption happened several times, bleeding occurred, and her birth witnessed a great loss of blood. As a medical doctor normally does, I was filling out the clinical record and asked the young lady numerous questions. The patient’s mother was present during the medical visit.
When I asked the daughter a simple question, “Do you know your blood type? Is it 0, A, B or AB?”, something unexpected happened. The mother became extremely alarmed and went on repeating obsessively: “My daughter doesn’t have my blood type!”.
I was astonished by the vehemence and the emotional charge of the mother. “Curious”, I thought, instead of becoming irritated as a result of the mother’s intense interruption.
From that day on, I consistently asked all the anorexic girls suffering from Anorexia of the Female Adolescent and their mothers about their blood types. To my great surprise, the result was: young women suffering from Anorexia of the Female Adolescent do not possess the same blood type (0, A, B, AB) of their mothers.
I had a very significant case as an example in this regard: a family composed of a mother with blood type A, a father with blood type B and the two daughters, the first with blood type A and the second with B, slightly younger. The environment, the school, the educational principles of the family, the habits and friendships were very similar for both. In the history of both there were no significant traumatic facts and their lives until adolescence took place in a very similar way. However, the story of the two daughters differed from adolescence. The daughter with B, like her father, at adolescence had a very serious form of Anorexia of the Female Adolescent which, with ups and downs, continued until she was 32 years old, when she came to me. She was visibly suffering from anorexia and was single. I had observed that the mother, talking about this daughter, whatever her daughter said or did, commented: “This my daughter is very strange”. Just to give you an example, her daughter wanted to take a trip to Africa, which is quite usual today. But the mother commented that going to Africa was a strange idea. The paradoxical thing was that her husband, the girl’s father, had long dabbled in being an explorer and had spent a long time talking to me about his travels, including those in Africa. The other daughter, slightly older, with blood type A, like her mother, had never suffered from anorexia. The mother, speaking of her, said: “This daughter is really all right, married, with two children”. In summary: the daughter with a blood type different from that of her mother was suffering from Anorexia of the Female Adolescent, the other daughter, with the same blood type as her mother, is not suffering from anorexia.
In my personal collection of data (over 100 cases collected in 25 years):
a) Only the women who have a different blood type (0, A, B, AB) from the mother are suffering from Anorexia of the Female Adolescent (there are no exceptions in my data)
b) many women have a different blood type from the mother and are not anorexic
The hypothesis of why different blood type mother/daughter only in some of these girls is biological condition for Anorexia of the Female Adolescent is that there has been a blood contact, not necessarily detected, between the two during pregnancy and/or at birth.
Let me explain it better. The placenta manages the exchange of oxygen, carbon dioxide, nutrients and waste between the blood of the fetus and the blood of the mother. The placenta does not permit red blood cells of the mother and those of the fetus to come into contact. For this reason, there is usually no problem between mother and daughter with different blood types (0, A, B, AB).
But what happens if the different blood types of the mother and of her daughter come into contact? This could happen, for example, during a high-risk pregnancy and/or birth (if it is particularly traumatic) or during any other event that may have led to contact between the blood of both mother and daughter. These events, which cause the passage of a few red blood cells beyond the placental barrier, can be caused by placental suffering due to natural causes or sometimes also following invasive surgical or diagnostic intrauterine interventions.
Let’s go back to our question: what happens if the different blood types of the mother and of her daughter come into contact?
Something very similar to the alarm when a transfusion, between a donor and a patient of incompatible blood types, occurs in medicine by mistake.
In the case of wrong blood transfusion, the patient is at risk of dying. But here we are not talking about a transfusion, they are just only a few drops that cross the placenta. If only a few drops of incompatible blood come into contact with each other, the fetus is not at risk of dying, however an alarm is triggered, an alarm that is one of the strongest in the human body.
This alarm caused by contact between incompatible mother/daughter blood types is equal to what would happen with a wrong transfusion and it is a real trauma. The strong effects of this alarm are:
![]() Immunological
Immunological
![]() Neurovegetative
Neurovegetative
![]() Physiological
Physiological
![]() Emotional
Emotional
This alarm perturbs the relationship between mother and daughter especially in such a sensitive period as the daughter’s adolescence.
In conclusion we can say that:
The blood types of the mother and of the daughter are different + Contact of mother’s blood and the blood of her daughter = Biological condition for Anorexia of the Female Adolescent. This biological condition is a conditio sine qua non, that means a condition that is necessary but not sufficient.
This upstream biological condition allows the causes to be efficient and lead to anorexia. Anorexia cannot be induced solely by the causes we have listed (disfunctional: relationship with herself, mutual mother/daughter relationship, mutual father/daughter relationship, mutual relationship between the girl and the environment surrounding her, affective and emotional communication between the family members, eating habits of the family). These causes are also present in several girls not suffering from anorexia. On the other hand, the biological condition alone without causes cannot induce anorexia.
Nowadays Anorexia of the Female Adolescent is very dangerous, revealing a high mortality rate. This mortality is usually due to the fact that the diagnosis is made too late, indeed many girls suffering from Anorexia of the Female Adolescent seek help from medical services for the first time when they are already skin and bones (long after three months of absence of the menstrual cycle: six months, one year, sometimes longer). With my new theory all physicians can make an early diagnosis because the group at risk of anorexia to be monitored is reduced to a small percentage of adolescent girls: only those with a blood type different from that of the mother. Knowing that a girl has a different blood type from her mother, she may be subject to discreet monitoring by the family doctor or school psychologist. As soon as the family doctor or school psychologist sees that the girl is slimming, must check if the girl has had the menstrual cycle in the last three months. If the control gives a negative result, the girl could have early diagnosis of Anorexia of the Female Adolescent, certainly not long after the third month of absence of the menstrual cycle.
So the treatment of the anorexia can start immediately. Nowadays, in the western-style societies, most adolescent girls were born in hospital. Usually the hospital detects the blood type of the mother and the newborn. Public health using the databases of obstetric hospitals could easily communicate to the family doctor and the school psychologist what are the girls with blood type different from that of the mother.
I hope that this article encourages many to carry out control studies on my theory which, once recognized as valid and shared, could save many lives allowing early diagnosis.
I have been asked several times how many are girls of blood type different from that of the mother versus those who have the same blood type as the mother.
In this regard, it does not seem to me that there is an official statistic and, furthermore, the percentages could fluctuate in different historical periods and different geographical areas, depending on many factors such as e.g. ethnic mosaic.
Peter D’Adamo with his studies on genome-based nutrition has been interested in blood types, but it does not seem to me that he has a comparative statistic of the blood type of the mother and that of the daughter.
Based on my experience, I can assume that the percentage of daughters with blood types different from that of the mother is around 8%. If we consider that Anorexia of the Female Adolescent concerns about 0.15% of the female population, and that, according to my theory, it concerns only girls of blood type different from that of the mother, for them the risk would represent approximately 2% (see figure 1).
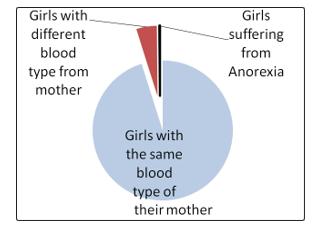
Figure 1: Just a small percentage of girls has to be considered for risk of Anorexia of the Female Adolescent: just the girls with a different blood type from their mothers (this graph has an indicative value: the percentages could fluctuate in different historical periods and different geographical areas, depending on many factors such as e.g. ethnic mosaic, nevertheless it is a good general approximation).
In addition, if we know that blood types mother/daughter are different and, moreover, we are able to determine whether there has been blood contact, e.g. caused by invasive surgical or diagnostic intrauterine interventions, and we know that the psychological and relational causes for Anorexia of the Female Adolescent are present in the daughter and her family, we can formulate not only an early diagnosis of Anorexia of the Female Adolescent, but we can also formulate a hypothesis of risk (predictive diagnosis) well before adolescence [1].
In case of predictive diagnosis, same as in case of early diagnosis, we could set a therapy without waiting for the girl to become skinny.
Being underweight constitutes a hazard for life and in any case having been for a long time underweight can lead to lifelong deficiency syndromes (such as osteopenia and osteoporosis) even if Anorexia of the Female Adolescent has been resolved.
This immunological, neurovegetative, physiological and emotional alarm – different blood types (0, A, B, AB) in mother and daughter coming into contact with each other during the pregnancy and/or at birth - is a real trauma that disturbs the mother/daughter relationship, especially during adolescence of the daughter. This alarmed relationship between mother and daughter is wrongly interpreted, by the environment and by them, as a conflict. My theory allows you to interpret the relationship between mother and daughter not as conflicting. The relationship is loaded with an alarm triggered by the immunological, neurovegetative, physiological, and emotional alarm due to trauma of contact between incompatible blood types. My theory brings a wave of peace within the family: one thing is to think that the relationship between mother and daughter is conflicting, and much else is to see that relationship as an alarmed relationship. The alarm is, however, a form of love, albeit dysfunctional. Interpreting the mother/daughter relationship as an alarmed and non-conflicting relationship leaves the family out of that shadow of shame and blame in which it would tend to be in the case of Anorexia of the Female Adolescent. Blame is often rampant in families with a daughter suffering from Anorexia of the Female Adolescent, but, typically and paradoxically, blaming simply leads to an intensification of the symptomatic behaviors. The word “anorexia” would no longer be a source of shame, but it would become a speakable word by the family at the first suspect and this would also facilitate access to therapy.
From this point of view the differences between mother and daughter can be interpreted as a source of enrichment for both, rather than a source of shame and blame. The family no longer needs to play the blame game: Who is to blame? The mother? The daughter? The father? The shadow of blame and shame can leave the family.
The vision of the scene changes completely: from the alarm to the peace. A daughter suffering from Anorexia of the Female Adolescent is no longer seen as hostile, but as a person seeking her identity. Respecting these differences between mother and daughter may actually encourage the young girl in her own differentiation and self-discovery.
Multidisciplinary Therapy
International Clinical Practice Guidelines agree that the prognosis of anorexia depends on: early diagnosis, continuity of treatment, multidisciplinary therapeutic approach [2]. It is clear how we all agree on the importance of early diagnosis.
Treatment of Anorexia of the Female Adolescent must be multidisciplinary, involving more health specialists, who need to deliver coherent messages, having unity in sharing a therapeutic plan.
Treatments must be articulated on multiple levels of intensity depending on the patient’s severity level: you go from ambulatory to hospitalization.
Let’s see the health professionals who are involved.The central figure is the psychotherapist.The nutritionist is absolutely indispensable for a proper diet re-education of the girl and possibly of the whole family, which often has bad food habits.
One or more family therapists are also needed. The patient’s family should be therapeutically followed to help the girl and because the family is often involved in the pathogenesis of her eating disorder.
These figures (patient’s psychotherapist, nutritionist physician, and family therapists) are needed for Anorexia of the Female Adolescent therapy. Sometimes the matter can be more complicated. The new forms of Anorexia of the Female Adolescent are often characterized by: lowering the onset of anorexia, association with autolesive behavior, suicidal ideation, and attempted suicide. Self-harm and suicidal behaviors require pharmacotherapy, so in these cases the figure of the psychiatrist is also needed.
At this point to further clarify the therapy I think it is good to present a clinical case. Initially I was interviewed by a mother who wanted to be helped to manage her daughter’s anorexia. The mother has blood type 0, daughter A and father A. In the medical history, the mother had had blood loss during the first months of her pregnancy and had had amniocentesis. The delivery was relatively traumatic and the mother suffered an episiotomy to avoid tearing.
It is likely that the mother, blood type 0, had come into contact with the blood of her daughter, blood type A. In this case, the mother would have activated, for pure biological reasons, the traumatic alarm of incompatible blood type. The mother, who was a ballet dancer in adolescence, had a history of severe Anorexia of the Female Adolescent and did not feel able to cope with that of her daughter.
She wanted her husband to take care of this problem. The idea that her daughter should go to therapy was not yet conceivable in that familiar context. So I accepted her husband as a patient because I thought he needed therapy and also that it was the only way to open a therapy path for her daughter.
Being the father’s therapist, following the universally recognized guidelines, I later didn’t take on other roles in the therapy of the girl suffering from Anorexia of the Female Adolescent.
Subsequently, the girl chose a woman, Junghian Analytical Orientation Psychotherapist and EMDR (Eye Movement Desensitization and Reprocessing) Practitioner.
The parents chose a psychotherapist for parental support. She later became the mother’s therapist. The role of the nutritionist was hired by a medical doctor, specialist in Food & Nutritional Science.
The girl initially showed a lot of resistances to therapy and her slimming continued. In Anorexia of the Female Adolescent, treatment resistance is very common. This resistance is intrinsic to anorexia, because the patient has deep ambivalence of wanting to heal and of not wanting to heal. Living without eating is the “basso continuo” that accompanied this patient.
The patient expressed her deep rage by not eating.
The slimming became a weapon to assert herself against the parents, that is, an unconscious psychological defense.There is a disorder of the person’s maturation about attachment and connection processes. These processes have been problematic and perhaps even traumatic in early childhood and fetal life for various causes, to which we add: mother/daughter blood type difference + blood contact between the two. The patient with these attachment dynamics is in need of to be approved, but for her ambivalence this need blends with the need to fight using fasting as a weapon.
In treating this patient, as always in the therapy of Anorexia of the Female Adolescent, one must keep in mind that the psychic-somatic problem becomes a somatic-psychic problem.
Let me explain better: a psychic dynamic creates a somatic situation that, in turn, tends to keep up the psychic dynamic. In fact, fasting, which begins by a psychic dynamics, has a dopaminergic effect on soma. Dopamine makes the person feel full of energy, euphoric and satisfied: it is the hormone of pleasure and reward. At the basis of the gratification given by reduced food intake there is the dopaminergic system of reward which leads to an increase in the push towards food restriction in order to keep the dopamine production high. The dopaminergic system gives a gratification also if the hunger persists [3].
The patient’s weight decreased to 36 kg / 1.60 meters in height (79,3 lb / 5,25 ft).The clinical case of this patient gives us the opportunity to describe the mechanism of dopamine even in those anorexic girls who, for top-level sports performances (eg ballet dance, artistics gymnastics, cycling), undergo sacrifices and efforts that appear inconceivable to those who are not under the dopaminergic effect caused by inadequate nutritional support. In the athletes there is a so-called “athlete’s triad”, consisting of: nutritional deficiency, amenorrhea, osteoporosis.
Our patient, as happens with athletes, also shows an initial osteoporosis to bone densitometry despite adequate electrolytes and vitamins, including Vitamin D, prescribed by the nutritionist. A serious osteoporosis always characterizes severe Anorexia of the Female Adolescent and may be the cause of osteoporosis for the rest of life with an increased risk of fractures.
We are not tired of saying anorexia is characterized by: weight loss and menstrual cycle loss for more than three months. We repeat this to warn the doctor who, in the face of amenorrhoea resulting from anorexia that probably did not investigate and diagnose, thinks to subject the patient to hormone therapy. The main therapeutic strategy of amenorrhea due to anorexia is the improvement of nutritional support with psychological support.
This patient has also become amenorrhoeic during anorexia and the menstrual cycle is resumed only after proper weight rebalancing.
The therapy of an anorexic patient, which is already not easy to do because of the patient’s resistance, is sometimes even more complicated because of “clinicians’ negative reactions to treatment-resistant or stigmatized patient groups. Some research has found that clinicians across professional disciplines react negatively to patients with eating disorders. Inexperienced clinicians appeared to hold more negative attitudes toward patients with eating disorders than toward other patient groups. Clinician negative reactions in regard to patients with eating disorders typically reflected frustration, hopelessness, lack of competence, and worry” [4].
“Clinicians may play an inadvertent role in perpetuating eating disordered behaviour. Interpersonal reactions are of particular relevance as clinicians (as family members) may react with high expressed emotion and unknowingly encourage eating disorder behaviours to continue. Hostility in the form of coercive refeeding in either a hospital or outpatient setting may strengthen conditioned food avoidance and pessimism may hamper motivation to change” [5].
Clinicians must be careful not to get caught in the patient’s play, that is, to have a countertransference of pity, impotence, servility, despair, and even in their opposite of anger, therapeutic fury, refusal to the patient, unfounded hope. A healthy understanding of the patient’s reasons allows the clinician to avoid counter-aggression.
The clinician, in the forms of severe anorexia, must handle the distress of death he perceives regarding the patient. Faced with the blackmail of the patient to suicide also by fasting, this anxiety would lead the clinician to a discouragement that leads him to increased anger and control over the patient or lowering his arms.
There was this risk with our patient which, despite the therapy, had reached 36 kg at 1.60 meters (79,3 lb / 5,25 ft). But thanks to the expertise and firmness of each of the clinicians and thanks to a clear therapeutic contract, which each clinician had stipulated for achieving attainable goals, discouragement was avoided.
It was also necessary to disarm the alarm that the mother projected on her daughter. For this alarm, the mother used to repeat insistently “Did you eat?”, “You have to eat!” This insistence increased her daughter’s blackmail towards her parents by not eating.
I did some sessions of therapy to disable mother’s alarm. This therapeutic process began by making the mother aware of how the alarm she had about her daughter probably depended on that alarm she had suffered during pregnancy (there had been many events that could have been cause of contact with the incompatible blood type of her daughter: blood loss during the first months of pregnancy, amniocentesis and episiotomy).
This awareness, that the alarm was due to biological facts she was not responsible for, allowed the mother to calm herself a little at a time.
It was thus possible to carry out an appropriate trauma therapy. There are many trauma therapies available today such as, for example, Lawrence Heller’s NARM NeuroAffective Relational Model, Peter Levine’s SE Somatic Experincing, Francine Shapiro’s EMDR Eye Movement Desensitization and Reprocessing, Nader Butto’s FEEL Fast Emotional Elaboration and Liberation and many others. The most important thing is that the therapist uses a trauma therapy with which he/she is very familiar. In this case, I used NeuroAffective Relational Model and Somatic Experiencing, with good results [6-9].
The mother accepted in good faith that her daughter’s nutrition was entirely taken care of by her husband. He did not have a past of anorexia as she was, in this respect not only was it very serene but was indeed a gourmet. His father started cooking delicious things, in keeping with the nutritionist’s point of view, and attending good restaurants with his daughter.
And so, with everyone’s commitment, the patient slowly came to accept a healthier way of controlling nutrition and lifestyle.
The weight began to rise. At this point an error, which one could commit, is uncontrolled refeeding that can lead to “refeeding syndrome”. It occurs for sudden and excessive intake of foods after a long period of fasting, especially if they are made up of large amounts of carbohydrates. After a long fast, the sugars eaten quickly go into the bloodstream. Cells absorb these sugars very quickly and require a large amount of electrolytes to metabolize them. These electrolytes are subtracted to the blood, which already has few electrolytes due the long fasting. An electrolyte imbalance is likely, in particular due to phosphorus deficiency, and it can also be deadly for acute heart failure. In fact, refeeding syndrome occurs when no gradual refeeding is planned with adequate amounts of nutrients, electrolytes, vitamins.
But this problem has not occurred with our patient thanks to the good work of the nutritionist. Three years later father and daughter are on summer holiday near the sea. During school time, the daughter spends a lot of time in the kitchen between homework and school hours. So, on this particular holiday, they decide to take a break from the kitchen, as well as from the studies. They run along the Ligurian Riviera looking for gastronomic delicacies, without bias or preference: street food in local food festivals, gourmet restaurants and popular taverns. The idea of a gourmet holiday was absolutely new.
Now father and daughter can write: “A few years before, the girl, now an adult, had fallen into a complex trap which is called Anorexia of the Female Adolescent. Her parents, as usually happens, were also confused. It was a situation of shared pain, and nobody had an idea as to what could be done. The dilemma was that the girl knew what she wanted to do: eat as little as possible and eventually reach a state in which she wouldn’t eat anything at all.
Escaping that pain was very difficult, a battle with ups and downs. But which battle are we talking about? Who was the enemy? We found the closest description of this battle in the theory about anorexia of Dr. Lorenzo Bracco. For the first time, as a result of this discovery (the alarm due to contact during pregnancy between different mother and daughter blood types, alarm that deeply disrupted their relationship), each family member, including the daughter, found their way of peace with each other beyond conflict. The feeling of being lost, the blame game, and the self-blame into which the family had hopelessly fallen, was slowly replaced by a sense of collaboration against the problem” [10-14].
Now she is 23-year-old girl, normal weight, has a boyfriend, loves cooking, studying oriental languages at university. Now, for the second time, she attends an intensive Japanese language course of six months in Tokyo, leaving her parents alone with her dog.
References
- Bracco L (2014) ANOREXIA: The Real Causes: Blood Types and Trauma. Amazonhttps://www.amazon.com/ Anorexia-Causes-Blood-Types Trauma/dp/1499702787/ lorenzo+bracco+anorexia&qid=1564040918&s=books&sr=1_1_1?keywords=lorenzo+bracco+anorexia&qid=1564040918&s=books&sr=1-1
- Clinical Practice Guidelines (2006) American Psychiatric Association-APA https://www.psychiatry.org/psychiatrists/practice/clinical-practice-guidelines
- Zink CF & Weinberger DR (2010) Cracking the moody brain: The rewards of self starvation, Nature Medicine 16: 1382-1383.
- Thompson-Brenner E, Satir DA, Franko DL & Herzog DB (2012) Clinician Reactions to Patients With Eating Disorders: A Review of the Literature. Psychiatric Services 63: 73-78.
- Treasure J, Crane A, McKnight R, Buchanan E & Wolfe M (2011) First do no harm: iatrogenic maintaining factors in anorexia nervosa. Eur Eat Disord Rev19: 296-302.
- Heller L & LaPierre A (2012) Healing Developmental Trauma. (Berkeley, Ca). North Atlantic Books. https://www. northatlanticbooks.com/shop/healing-developmental-trauma/
- Levine PA & Frederick A (1997) Waking the Tiger: Healing Trauma : The Innate Capacity to Transform Overwhelming Experiences. North Atlantic Books.https://www. northatlanticbooks.com/shop/waking-the-tiger-healing-trauma/
- Shapiro F (2017) Eye Movement Desensitization and Reprocessing (EMDR) Therapy. Guildford Press.https:// www.guilford.com/books/Eye-Movement-Desensitization-and-Reprocessing-EMDR-The rapy/Francine-Shapiro/9781462532766
- Butto N (2016) Unified Integrative Medicine: A new Holistic model for personal growthspiritual evolution http://it.naderbutto.co.il/wp-content/ uploads/2015/08/51SGHpePafL._SY344_BO1204203200_.jpg
- Voltolini D & Voltolini E (2014) Così abbiamo fatto pace con il cibo (And So, We Became Friends With Food), Corriere della Sera. http://lettura.corriere.it/cosi-abbiamo-fatto-pace-con-il-cibo/
- Lowen A (1975) Bioenergetics. New York, Coward, McCann & Geoghegan Inc. https://openlibrary.org/books/OL5070674M/Bioenergetics
- Management of Really Sick Patients with Anorexia Nervosa (Marsipan 2010) https://www.rcpsych.ac.uk/docs/default-source/improving-care/better-mh-policy/college-reports/ college-report-cr189.pdf?sfvrsn=6c2e7ada_2
- National Institute for Clinical Excellence (NICE 2017) https://www.nice.org.uk
- Royal Australian and New Zealand College of Psychiatrist(RANZCP 2014) https://www.ranzcp.org/home