
Advances in Hematology and Oncology Research(AHOR)
ISSN: 2692-5516 | DOI: 10.33140/AHOR
Impact Factor: 1.2


Case Report - (2024) Volume 7, Issue 2
An Uncommon Culprit: Pancreatic Neuroendocrine Tumor in a Patient with Uncontrolled Diabetes
2Johnston Memorial Hospital, United States
Received Date: Aug 01, 2024 / Accepted Date: Aug 23, 2024 / Published Date: Aug 30, 2024
Copyright: ©Â©2024 Supriya Peshin, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Peshin, S., Borda, M. S., Dhakal, A. (2024). An Uncommon Culprit: Pancreatic Neuroendocrine Tumor in a Patient with Uncontrolled Diabetes. Adv Hema Onco Res, 7(2), 01-03.
Abstract
Pancreatic Neuro Endocrine Tumors (NETs) are rare neoplasms that originate from the endocrine tissues of the pancreas, accounting for only 1-2% of pancreatic tumors. Despite their low incidence, these tumors present with a wide range of symptoms and have the ability to secrete hormones, posing significant challenges for their diagnosis and treatment. There are two distinct types of pancreatic NETs: functioning and nonfunctioning. Functioning tumors are characterized by hormone-related clinical syndromes, while nonfunctioning tumors are often found incidentally. The pathogenesis of pancreatic NETs involves both sporadic and hereditary factors, including syndromes such as MEN1, VHL, and NF1. Typically, these tumors are diagnosed in individuals between the ages of 40 and 60, and their effective management requires a multidisciplinary approach. Diagnostic imaging techniques, such as CT and EUS, play a crucial role in accurate diagnosis, while PET scans aid in staging and treatment planning. Histological analysis is essential for determining the tumor grade and predicting prognosis. Treatment strategies are tailored to the tumor's characteristics and the patient's overall health. These may include the use of somatostatin analogs, such as Lanreotide and Octreotide, to control hormone secretion and inhibit tumor growth, as well as systemic therapies like everolimus, sunitinib, and PRRT for metastatic disease. This case report describes the clinical course of a 66-year-old male with a well-differentiated pancreatic NET who initially presented with persistent hyperglycemia. Further investigations revealed a sizable pancreatic mass and liver metastases. Diagnostic evaluation confirmed a grade 1 Neuro Endocrine Tumor, and the patient was started on treatment with Lanreotide. However, his management was complicated by the development of hepatic encephalopathy, which necessitated treatment with lactulose and rifaximin. This case highlights the importance of considering pancreatic NETs in cases of atypical diabetes presentations and emphasizes the need for a multidisciplinary team to provide optimal care. Given the complex nature of pancreatic NETs, a comprehensive diagnostic workup and personalized treatment approach are essential for improving patient outcomes.
Introduction
Pancreatic Neuro Endocrine Tumors (NETs) are tumors that develop from the hormone-producing tissues of the pancreas. They account for only 1-2% of all pancreatic tumors but are clinically significant, with an incidence rate of less than one case per 100,000 individuals per year. Pancreatic NETs are classified as functioning or nonfunctioning based on their ability to produce hormones. Functioning tumors can produce hormones such as insulin, gastrin, glucagon, and vasoactive intestinal peptide, leading to specific clinical syndromes that often serve as the initial indication of the disease. On the other hand, nonfunctioning tumors do not produce hormones and are usually found incidentally or due to symptoms such as abdominal pain or obstructive jaundice.
Pancreatic NETs can develop sporadically or be associated with hereditary syndromes such as Multiple Endocrine Neoplasia type 1 (MEN1), Von Hippel-Lindau (VHL) syndrome, and neurofibromatosis type 1 (NF1). Although these tumors can occur at any age, they are most commonly diagnosed in individuals in their forties to sixties. A comprehensive and multidisciplinary approach is necessary for diagnosing and managing pancreatic NETs. Imaging studies, particularly Computed Tomography (CT) and Endoscopic Ultra Sound (EUS), play a crucial role in the diagnostic process. CT scans provide detailed anatomical information, while EUS provides high-resolution images and enables fine-needle aspiration biopsies to obtain tissue samples for histopathological examination. Positron Emission Tomography (PET) scans using radiolabeled somatostatin analogs are particularly useful for staging and identifying somatostatin receptor expression, which has implications for treatment.
Histological analysis is vital in determining the grade of pancreatic NETs and guiding treatment decisions. Well-differentiated NETs generally have a better prognosis compared to poorly differentiated neuroendocrine carcinomas, which are aggressive and progress rapidly. Treatment strategies for pancreatic NETs are diverse and personalized, considering the individual patient's tumor characteristics and overall health. Somatostatin analogs such as Lanreotide and Octreotide are commonly used to manage symptoms of hormone hypersecretion and may also inhibit tumor growth. For metastatic disease, systemic therapies such as molecularly targeted agents like everolimus and sunitinib, as well as Peptide Receptor Radioligand Therapy (PRRT), are employed.
This case report presents the case of a 66-year-old male with a significant medical history who experienced hyperglycemia and was subsequently diagnosed with a well-differentiated neuroendocrine tumor of the pancreas. The complexity of his condition and the challenges faced in managing his disease highlight the importance of a comprehensive diagnostic evaluation and personalized treatment plan. This case also emphasizes the need to consider pancreatic NETs in patients with atypical presentations of diabetes and underscores the critical role of a multidisciplinary team in delivering optimal care.
Case Presentation
A 66-year-old male with a significant medical history including insulin-dependent diabetes mellitus type 2, GERD, hyperlipidemia, hypertension, diabetic neuropathy, BPH, and hypothyroidism, presented to the clinic after visiting the emergency department for hyperglycemia. He reported gastrointestinal symptoms from Metformin, which led to its discontinuation. Subsequently, he was prescribed insulin glargine (10 units in the morning), but despite dose adjustments and CGM for better glucose monitoring, his blood glucose levels remained erratic.
Due to persistent hyperglycemia and fluctuating glucose levels, a pancreatic malignancy was suspected. A CT scan of the chest, abdomen, and pelvis revealed a large mass measuring 10 cm in the pancreatic head, neck, and body region, with the pancreas appearing atrophic and displaced (Figure). There was also dilation of the pancreatic duct and multiple low-density liver lesions suggestive of metastasis. The patient was referred for further evaluation and management at a university medical center.
Further diagnostic workup included a PET scan consistent with stage IV cancer, EGD with EUS of the pancreas, which revealed a well-differentiated neuroendocrine tumor grade 1, and a CT-guided liver biopsy confirming metastatic pancreatic neuroendocrine tumor. The patient was started on Lanreotide 120mg subcutaneously every four weeks. His clinical course was further complicated by episodes of hepatic encephalopathy, necessitating treatment with lactulose and rifaximin requiring multiple hospitalizations.
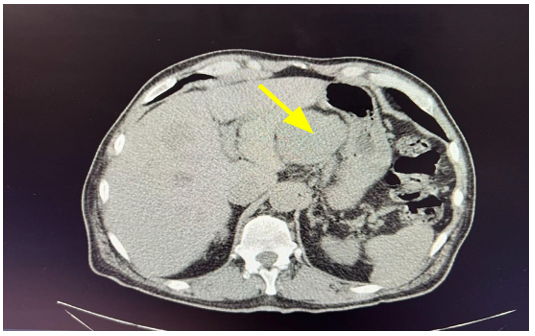
Figure: Metastatic Pancreatic Neuro Endocrine Tumor (Yellow Arrow)
Discussion
Pancreatic Neuro Endocrine Tumors (NETs) present unique challenges in terms of diagnosis and management due to their diverse clinical manifestations and potential for metastasis, particularly to the liver. These tumors are often incidentally discovered during imaging for other conditions or when symptoms related to hormone hypersecretion or mass effect become apparent.
Diagnostic Assessment
Imaging: Computed Tomography (CT) and Endoscopic Ultra Sound (EUS) play a vital role in detecting pancreatic NETs, with EUS offering high sensitivity and the ability to perform fine-needle aspiration for histological diagnosis. Positron Emission Tomography (PET) scans using radiolabeled somatostatin analogs are useful for staging and evaluating receptor expression, aiding in treatment guidance. Histological Examination: Biopsy and tumor grading (well-differentiated vs. poorly differentiated) are crucial for determining prognosis and treatment planning. In this particular case, the tumor was well-differentiated, which generally indicates a more favorable prognosis and necessitates a different treatment approach compared to poorly differentiated neuroendocrine carcinomas.
Treatment
A) Somatostatin Analogs: Lanreotide and octreotide are effective in managing symptoms of hormone hypersecretion and may also exert antiproliferative effects. In this patient's case, Lanreotide was initiated.
B) Systemic Therapy: Options for systemic therapy include molecularly targeted agents such as everolimus, sunitinib, and cabozantinib, all of which have demonstrated efficacy in prolonging progression-free survival in metastatic pancreatic NETs. Peptide Receptor Radioligand Therapy (PRRT) is another option for tumors positive for somatostatin receptors.
C) Management of Complications: Hepatic encephalopathy, a complication experienced by this patient, was treated with lactulose and rifaximin.
Conclusion
Pancreatic Neuro Endocrine Tumors (NETs) are rare tumors that present challenges in diagnosis and treatment. This case study focuses on a 66-year-old man diagnosed with a well-differentiated pancreatic NET, highlighting key points in managing this condition. The patient had difficulty controlling high blood sugar levels despite insulin therapy. This underscores the importance of considering underlying cancer when managing problematic diabetes. Diagnostic imaging studies, such as CT and PET scans, played a crucial role in identifying a large tumor in the pancreas, as well as liver metastases. The detection of a well-differentiated neuroendocrine tumor through EUS and biopsy guided the subsequent treatment plan, which involved using Lanreotide to control hormone overproduction and slow tumor growth. Managing complications, including hepatic encephalopathy, requires an individualized approach. In this case, the patient received lactulose and rifaximin. Comprehensive care relies on a team of specialists, including endocrinologists, oncologists, gastroenterologists, and radiologists.
Treatment options for pancreatic NETs include somatostatin analogs, targeted therapies, and PRRT. The choice of treatment should consider tumor characteristics, stage, and the patient's overall health. In this case, Lanreotide effectively reduced symptoms and slowed disease progression, despite episodes of hepatic encephalopathy. This highlights the importance of promptly recognizing and accurately diagnosing pancreatic NETs, as it allows for timely treatment and better outcomes. The complex nature of these tumors requires a thorough diagnostic evaluation and a personalized treatment plan that addresses both the primary tumor and any metastatic disease. In conclusion, a high level of suspicion and a comprehensive diagnostic approach are crucial when dealing with pancreatic NETs. Using somatostatin analogs, targeted therapies, and supportive care for complications is vital for effective management. This case emphasizes the importance of a multidisciplinary approach and considering pancreatic NETs as a possible cause in patients with unexplained metabolic abnormalities [1-5].
References
- Dasari, A., Shen, C., Halperin, D., Zhao, B., Zhou, S., Xu, Y.,... & Yao, J. C. (2017). Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA oncology, 3(10), 1335-1342.
- Yao, J. C., Hassan, M., Phan, A., Dagohoy, C., Leary, C., Mares, J. E., ... & Evans, D. B. (2008). One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. Journal of clinical oncology, 26(18), 3063-3072.
- Vinik, A. I., Woltering, E. A., Warner, R. R., Caplin, M.,O'Dorisio, T. M., Wiseman, G. A., ... & Go, V. L. W. (2010). NANETS consensus guidelines for the diagnosis of neuroendocrine tumor. Pancreas, 39(6), 713-734.
- Halfdanarson, T. R., Rabe, K. G., Rubin, J., & Petersen, G.M. (2008). Pancreatic neuroendocrine tumors (PNETs): incidence, prognosis and recent trend toward improved survival. Annals of oncology, 19(10), 1727-1733.
- Klimstra, D. S., Modlin, I. R., Coppola, D., Lloyd, R. V., & Suster, S. (2010). The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas, 39(6), 707-712.