

Research Article - (2026) Volume 10, Issue 1
Allogeneic Umbilical Cord Mesenchymal Stromal Cells for Knee Osteoarthritis: Systematic Review and Meta-Analysis of Controlled Injection Trials
Received Date: Jun 05, 2026 / Accepted Date: Jun 30, 2026 / Published Date: Jul 06, 2026
Copyright: ©2026 Kirk Sanford. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Sanford, K., Porras, F., Martinez, F., Ramos, H., et al. (2026). Allogeneic Umbilical Cord Mesenchymal Stromal Cells for Knee Osteoarthritis: Systematic Review and Meta-Analysis of Controlled Injection Trials. Stem Cell Res Int, 10(1), 01- 08.
Abstract
Background Knee osteoarthritis is a leading cause of chronic pain and reduced mobility worldwide. Intra-articular corticosteroids and hyaluronic acid injections are commonly used, but many patients experience limited durability of symptom improvement. Allogeneic umbilical cord derived mesenchymal stromal cells (UC-MSCs) have emerged as a regenerative medicine strategy intended to modulate inflammation and improve clinical outcomes.
Objective To evaluate controlled clinical trial evidence for intra-articular allogeneic UC-MSC therapy in symptomatic knee osteoarthritis, with emphasis on durability of pain improvement at 12 months.
Methods A systematic review was conducted to identify controlled clinical trials evaluating intra-articular allogeneic UC-MSCs for knee osteoarthritis with comparator injection arms. The primary endpoint was WOMAC pain at 12 months. Secondary outcomes included WOMAC total at 12 months. When trials did not provide numeric endpoint values in tables, values were extracted from published figures as estimated mean and dispersion measures. Outcomes were synthesized under a random effects framework with consideration of comparator type (hyaluronic acid vs corticosteroid).
Results Two controlled trials met criteria for quantitative synthesis at 12 months. Across comparator subgroups, UC-MSC therapy demonstrated lower WOMAC pain scores at 12 months compared with control injections. UC-MSC therapy also demonstrated lower WOMAC total scores at 12 months relative to comparator injection arms. One phase I single- arm study was included in qualitative synthesis for feasibility and safety interpretation but was not eligible for pooled analysis.
Conclusion Controlled clinical trial evidence suggests intra-articular allogeneic UC-MSC therapy may provide durable improvements in knee osteoarthritis pain at 12 months compared with standard injection-based comparators. Larger randomized trials with standardized reporting are needed to further define efficacy, durability, and safety across broader populations.
Keywords
Knee Osteoarthritis, Umbilical Cord Mesenchymal Stromal Cells, Allogeneic Stem Cells, Regenerative Medicine, Womac, Intra-Articular Injection, Meta-Analysis
Introduction
Knee osteoarthritis is among the most prevalent causes of chronic pain, impaired mobility, and functional decline. Symptom burden often progresses over time, contributing to reduced activity tolerance and loss of quality of life.
Standard injection-based therapies such as intra-articular corticosteroids and hyaluronic acid are commonly used for symptom management. While these approaches can provide benefit in some patients, durability is frequently limited and patients often seek strategies associated with longer-lasting improvements in pain and function.
Allogeneic umbilical cord derived mesenchymal stromal cells (UC-MSCs) have gained increased attention in regenerative medicine due to proposed immunomodulatory, anti-inflammatory, and tissue homeostasis effects within the osteoarthritic joint environment. Controlled clinical trials comparing UC-MSC therapy with standard injection approaches offer clinically relevant insight into relative durability and symptom improvement.
The objective of this study was to systematically evaluate controlled clinical trial evidence for intra-articular allogeneic UC-MSC therapy in symptomatic knee osteoarthritis, with emphasis on WOMAC pain outcomes at 12 months. Secondary evaluation of WOMAC total outcomes was also performed to support interpretation of overall symptom and functional improvement.
Methods
• Reporting Standards
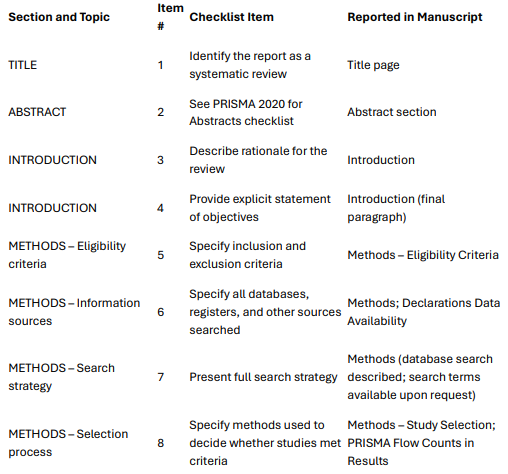
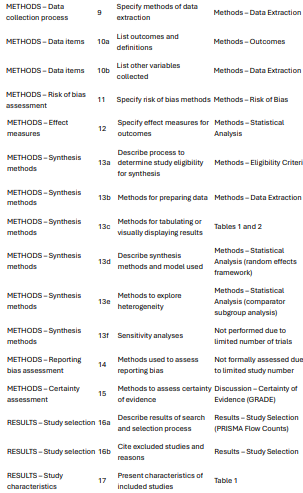
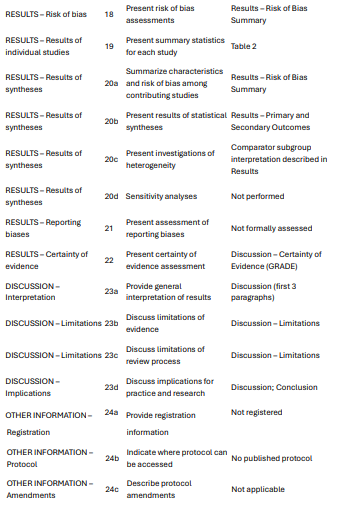
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. The completed PRISMA 2020 checklist is provided as a supplementary file.
PRISMA 2020 Checklist
Manuscript: Intra articular allogeneic umbilical cord mesenchymal stromal cells for knee osteoarthritis a systematic review and meta-analysis of controlled trials
• Study Design
This study was conducted as a systematic review and meta-analysis of controlled clinical trials evaluating intra-articular allogeneic UC-MSC therapy for knee osteoarthritis.
• Eligibility Criteria
Studies were eligible if they met the following criteria: human clinical trials enrolling adult patients with symptomatic knee osteoarthritis; intra-articular administration of allogeneic umbilical cord derived or umbilical cord tissue derived MSCs; inclusion of a comparator injection arm (placebo, sham, or active comparator); and reporting of WOMAC pain outcomes with follow-up available at, or near, 12 months.
Studies were excluded if they were reviews or meta-analyses, preclinical investigations, extracellular vesicle or secretome-only therapies without live MSC administration, or lacked a controlled comparator arm. Single-arm early-phase studies were retained for qualitative synthesis of feasibility and safety where appropriate.
• Outcomes
Primary outcome: WOMAC pain at 12 months. Secondary outcome: WOMAC total at 12 months. Additional outcomes included adverse events and supportive imaging findings when reported.
• Data Extraction
Study characteristics, comparator type, sample sizes, intervention protocols, and outcomes were extracted. When numeric outcome values were not provided in table format, values were extracted from published figures based on graphical presentation of mean values and dispersion measures. Extracted figure-based values were treated as approximations and were transparently described.
• Risk of Bias
Risk of bias was assessed using structured domains aligned with randomized trial methodology, including randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting.
• Statistical Analysis
Outcomes were interpreted using a random effects synthesis framework due to expected clinical and methodological heterogeneity. Comparator type was evaluated as a clinical subgroup (hyaluronic acid vs corticosteroid). Given the limited number of controlled studies, quantitative findings were interpreted cautiously as an early synthesis of controlled evidence.
• Protocol and Registration
This study is a systematic review and meta-analysis of previously published controlled trials and does not constitute a prospective clinical trial conducted by the authors. Therefore, clinical trial registration is not applicable.
Results
Study Selection (PRISMA Flow Counts)
Records identified through database searching: 36
Records screened (title/abstract): 36
Records excluded after title/abstract screening: 30
Full-text articles assessed for eligibility: 6
Full-text articles excluded: 3
Studies included in qualitative synthesis: 3
Studies included in quantitative synthesis (meta-analysis): 2
Reasons for full-text exclusion included review articles, non-controlled designs, or non-eligible interventions.
• Included Studies
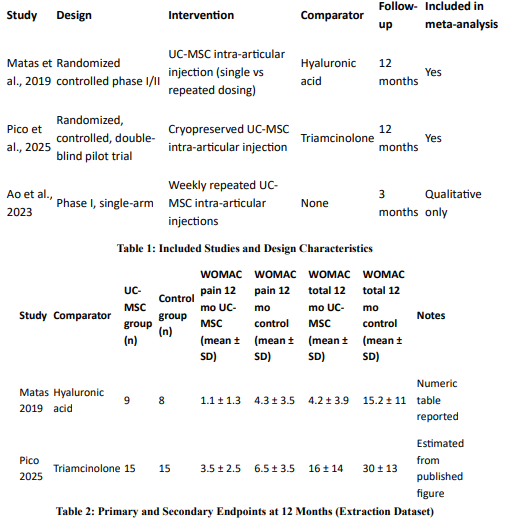
Two controlled trials were eligible for pooled quantitative synthesis at 12 months, with active comparator injection arms including hyaluronic acid and intra-articular corticosteroid. One phase I single-arm study evaluating repeated UC-MSC injections was included in qualitative synthesis for feasibility and safety interpretation only.
• Risk of Bias Summary
Overall risk of bias across the included controlled trials was considered low to moderate. Primary limitations were related to modest sample sizes and incomplete numeric reporting of follow-up outcomes in one trial, requiring figure-based data extraction for quantitative synthesis. No evidence of selective reporting within the primary pain outcome domain was identified.
• Primary Outcome: WOMAC Pain at 12 Months
Across controlled trials, UC-MSC therapy demonstrated lower WOMAC pain scores at 12 months compared with standard comparator injections. In the hyaluronic acid comparator trial, repeated UC-MSC dosing resulted in substantially lower WOMAC pain at 12 months relative to hyaluronic acid control. In the corticosteroid comparator trial, UC-MSC therapy demonstrated sustained improvement through 12 months compared with triamcinolone, supporting a durability advantage relative to intra-articular corticosteroid. Random effects synthesis favored UC-MSC therapy at 12 months for WOMAC pain, with consistent directionality across comparator subgroups. The characteristics of the included studies are summarized in Table 1.
• Secondary Outcome: WOMAC Total at 12 Months
Two controlled trials reported 12-month WOMAC total outcomes comparing UC-MSC therapy with active comparator injections. Across both comparator subgroups, UC-MSC therapy was associated with lower WOMAC total scores at 12 months compared with control injections, supporting broader improvement in symptom severity and function in addition to pain reduction. Extracted outcome data for WOMAC pain and WOMAC total at 12 months are shown in Table 2.
• Safety and Tolerability
No clear signal of severe treatment-related adverse events was identified across controlled trials included in the quantitative synthesis. The phase I qualitative study further supported feasibility and tolerability of repeated UC-MSC administration, though larger controlled trials are required to characterize rare risks and refine optimal dosing strategies.
Discussion
This systematic review and meta-analysis evaluates controlled clinical trial evidence for intra-articular allogeneic UC-MSC therapy in symptomatic knee osteoarthritis, with emphasis on durability of pain improvement at 12 months. Across controlled trials with active comparator injection arms, UC-MSC therapy demonstrated consistently favorable WOMAC pain outcomes relative to comparator injections including hyaluronic acid and intra-articular corticosteroid.
Durability of symptom improvement is a key clinical priority in knee osteoarthritis. Conventional injection-based therapies may provide temporary symptom relief, whereas UC-MSC therapy in controlled trial settings has demonstrated sustained improvements through 12 months. The consistent direction of benefit across comparator subgroups supports clinical relevance and justifies continued evaluation in larger randomized trials.
The observed clinical improvements may reflect joint microenvironment modulation through immunoregulatory and anti-inflammatory effects that influence pain signaling and functional limitation. Osteoarthritis pain is multifactorial and may improve through reductions in synovial inflammation and inflammatory signaling even when structural imaging endpoints do not uniformly demonstrate change over intermediate follow-up. This dissociation between symptomatic outcomes and imaging findings is consistent with broader osteoarthritis research and regenerative medicine trial experience.
Secondary analyses supported the primary findings. Across controlled trials, UC-MSC therapy was associated with lower WOMAC total scores at 12 months compared with comparator injection arms, suggesting broader improvement in overall symptoms and function in addition to pain reduction.
Safety remains essential in allogeneic cell therapy. Across the controlled evidence included here, no clear signal of severe treatment-related adverse events was identified. Early-phase repeated dosing data further support feasibility and tolerability, though larger controlled trials are required to establish rare risk profiles and confirm optimal dosing strategies.
Limitations
This analysis is limited by the small number of controlled trials currently available for quantitative synthesis, variability in comparator injection type, and differences in dosing strategies across studies. Additionally, complete numeric endpoint values were not uniformly reported in all included trials, requiring figure-based extraction for at least one 12-month outcome. Despite these limitations, the controlled study designs and consistent directionality of outcomes across comparator subgroups support a meaningful durability signal warranting further controlled investigation.
• Clinical Relevance
Intra-articular corticosteroids and hyaluronic acid are commonly used for knee osteoarthritis symptom management, but many patients experience limited durability of improvement. Controlled trial evidence synthesized here suggests allogeneic UC-MSC therapy may provide greater long-term symptom improvement at 12 months compared with standard injection approaches, supporting potential clinical value for patients seeking longer-lasting outcomes.
• Certainty of Evidence (GRADE)
Certainty of evidence for WOMAC pain at 12 months was considered low to moderate due to the limited number of controlled trials, modest sample sizes, and comparator heterogeneity. Despite these limitations, directionality of benefit was consistent across comparator subgroups.
Conclusion
Controlled clinical trial evidence suggests intra-articular allogeneic UC-MSC therapy may provide durable improvements in knee osteoarthritis pain at 12 months compared with standard injection-based comparators. While the controlled evidence base remains limited, consistent directionality of benefit supports continued evaluation in larger randomized trials designed to define durability, comparative efficacy, and safety in broader patient populations [1-3].
Author Contributions
Kirk Sanford conceptualized the study, supervised project execution, and contributed to manuscript drafting and final review. Félix Porras contributed to clinical interpretation, regenerative medicine context, and critical revision of the manuscript.
Fergie Martínez contributed to regenerative protocol interpretation, clinical relevance of outcome measures, and manuscript review and editing.
Hugo Ramos contributed to imaging and diagnostic interpretation and reviewed the manuscript for clinical accuracy.
Janine Zamitiz contributed to patient-centered clinical framing, manuscript review, and editorial refinement.
Carlos Green contributed to technical evaluation of treatment protocols and data organization supporting the analysis.
Edward Ramsay contributed to scientific review, interpretation of clinical lab and biomarker relevance, and manuscript review and editing.
All authors reviewed and approved the final manuscript.
Declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent to Publish
Not applicable.
Data Availability
Not applicable.
Conflict of Interest
The authors declare no conflicts of interest.
Funding
No external funding was received for this study.
References
- Matas, J., Orrego, M., Amenabar, D., Infante, C., Tapia-Limonchi, R., Cadiz, M. I., ... & Espinoza, F. (2019). Umbilical cord-derived mesenchymal stromal cells (MSCs) for knee osteoarthritis: repeated MSC dosing is superior to a single MSC dose and to hyaluronic acid in a controlled randomized phase I/II trial. Stem cells translational medicine,8(3), 215-224.
- Pico, O. A., Espinoza, F., Cádiz, M. I., Sossa, C. L., Becerra-Bayona, S. M., Salgado, M. C. C., ... & Arango-Rodríguez, M.L. (2025). Efficacy of a single dose of cryopreserved human umbilical cord mesenchymal stromal cells for the treatment of knee osteoarthritis: a randomized, controlled, double-blind pilot study. Cytotherapy, 27(2), 188-200.
- Ao, Y., Duan, J., Xiong, N., Qian, N., Zhang, R., Yang, L.,... & Wang, F. (2023). Repeated intra-articular injections of umbilical cord-derived mesenchymal stem cells for knee osteoarthritis: a phase I, single-arm study. BMC musculoskeletal disorders, 24(1), 488.