
International Internal Medicine Journal(IIMJ)
ISSN: 2837-4835 | DOI: 10.33140/IIMJ
Impact Factor: 1.02



Case Report - (2024) Volume 2, Issue 12
Advancing Physiatric Care with Laser Therapy and Hydrotherapy Integration in a Single Case Following Femoral Head and Neck Resection
Received Date: Nov 12, 2024 / Accepted Date: Dec 17, 2024 / Published Date: Dec 19, 2024
Copyright: ©©2024 Miriam Caramico,et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Caramico, M., De Dominicis, S. (2024). Advancing Physiatric Care with Laser Therapy and Hydrotherapy Integration in a Single Case Following Femoral Head and Neck Resection. Int Internal Med J, 2(12), 01-11.
Abstract
Hip dysplasia is a prevalent hereditary condition affecting dogs and cats, characterized by inadequate de-velopment of the hip joint. This condition leads to pain due to capsular distension, microfractures, and joint incongruity in young animals, ultimately progressing to osteoarthritis in adult and elderly animals. The pursuit of pain relief and improved quality of life for individuals with osteoarthritis has been a focal point in several studies. In this context, veterinary physiotherapy has gained prominence in small animal practice, serving as both palliative care and a supportive modality in the clinical or post-surgical management of degenerative joint diseases. Laser therapy and hydrotherapy, recognized for their analgesic effects and capacity to promote muscle mass gain, have garnered attention for their potential efficacy in treating joint diseases. This study aims to evaluate the therapeutic effects of super pulsed laser therapy and controlled low-impact exercises (water treadmill) on a patient recovering from surgery involving. bilateral femoral head and neck resection. We observed positive outcomes, including pain resolution, improved muscle mass, and enhanced range of motion, contributing to the patient's overall recovery.
Keywords
Orthopedic Rehabilitation Physical Therapy, Orthopedic Surgery, Osteoarthritis, Musculoskeletal System, Photo Biomodulation; Balance And Stability, Orthopedic Pain
Introduction
Coxofemoral dysplasia (CFD) (figure 01) is a prevalent orthopedic disease characterized by joint incongruity and subsequent osteoarthritis and pain, influenced by complex interactions of multiple genes and environ-mental factors impacting disease susceptibility [1-4]. Although the coxofemoral joint is normal at birth, the imbalance between skeletal and muscular system growth rates during development imposes excessive loads on the femoral head, altering acetabular conformation and leading to irregular joint surface remodeling [5-7].
CFD can progress to painful secondary osteoarthritis and affect the dog's behavior, manifesting as chronic lameness, muscle atrophy, and exercise reluctance [8-10]. While medical and surgical management can alleviate pain, they do not address underlying skeletal muscle conditions, which necessitates physiotherapy for effective treatment [11-13].
Clinical signs of CFD include pain, lameness, stiff gait, and muscle atrophy, with diagnosis relying on com-prehensive medical history, clinical evaluation, and imaging [5,14,15]. Manifestations may remain latent for extended periods, becoming apparent with the onset of degenerative joint disease [16,12,13].
The pathophysiology involves muscle contractures, joint inflammation, and increased intra-articular pressure, contributing to pain and joint dysfunction [2,5,17,18]. Contractures of the adductor muscles, notably the pectineus, can cause microfractures during growth remodeling, exacerbating the condition. Figure 01 sche-matically represents the congruence or incongruence of the hip joint (coxofemoral joint) in a normal hip, a hip with a moderate degree of dysplasia, and a hip with a severe degree of dysplasia [19].
In patients with osteoarthritis, increased intra-articular pressure and subchondral bone ischemia are prominent contributors to pain [2,5,17]. Understanding the multifaceted etiology and clinical manifestations of CFD is essential for targeted therapeutic interventions.
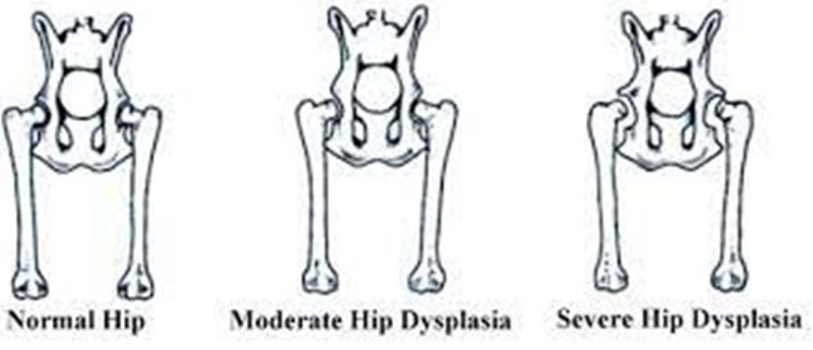
Figure 1: Normal Hip X Dysplasia [45]
The selection of an appropriate treatment strategy for coxofemoral dysplasia (CFD) hinges upon various factors, including the patient's age, the severity of dysplasia, and the presence of any concurrent pathologies. The primary objectives are to alleviate pain, enhance limb function, and optimize the patient's overall quality of life.
Conventional surgical interventions are often inadequate for addressing the complex anatomical alterations associated with CFD. Instead, comprehensive symptom management can be effectively achieved through physiotherapy (rehabilitation) combined with the integration of nutraceuticals. Unlike surgical approaches, physiotherapy specifically targets the underlying muscular, tendinous, and ligamentous changes associated with CFD [16,20-22].
For example:
• Pain in Extension, Adduction, and Flexion of the Joint Resection of the Head and Femoral Strain: No significant influence Rehabilitation: Controls pain and resolves issues with extension and adduction
• Intermittent Claudication and Paresis of Hind Limbs Resection of the Head and Femoral Strain: Improvement is observed, though often Rehabilitation: Always leads to improvement due to muscle mass gain
• Intra-articular Pressure Resection of the Head and Femoral Strain: Resolves the issue Rehabilitation: Controlled through a sequence of passive mobilization exercises
• Pectineus and Iliopsoas Contracture Resection of the Head and Femoral Strain: No significant influence Rehabilitation: Resolves contracture
• Hypertrophy of the Gluteus, Quadriceps, and Biceps Femoris Resection of the Head and Femoral Strain: No significant influence Rehabilitation: Promotes hypertrophy
• Pain in the Sacral Loin and Lumbar-Thoracic Spine Resection of the Head and Femoral Strain: No significant influence Rehabilitation: Controls pain and improves biomechanics
• Muscle and Joint Capsule Pain Resection of the Head and Femoral Strain: No significant influence Rehabilitation: Resolves pain through exercises and laser therapy
• Inflammation and Retraction of the Joint Capsule
Resection of the Head and Femoral Strain: Resolves the issue Rehabilitation: Resolves through exercises and laser therapy
Intra-articular pressure improvement following a Femoral Head Ostectomy (FHO) is not about pressure within a traditional joint space but rather about the reduction of abnormal pressure and pain caused by the presence of a dysfunctional or malformed joint. FHO involves removing the femoral head and neck, which effectively eliminates the source of abnormal joint pressure and inflammation. The surgical procedure aims to create a false joint or pseudoarthrosis, which allows for the development of a fibrous joint capsule and reduces the abnormal stresses and pressures that were present before the surgery. Consequently, this leads to a decrease in pain and improvement in function, as the pressure that was previously causing discomfort is alleviated [23].
Rehabilitation plays a crucial role in managing and improving joint function in the long term, particularly after surgeries like FHO. The goals of rehabilitation include enhancing the strength and flexibility of the surrounding muscles, improving joint stability, and promoting proper movement patterns. Through targeted physiotherapy exercises, muscle strengthening, and joint mobilization techniques, rehabilitation helps to redistribute forces and reduce strain on the affected area. This process supports the formation of a functional pseudoarthrosis and helps to normalize joint mechanics. Over time, effective rehabilitation can lead to improved joint function and reduced pain, contributing to the overall resolution of pressure-related issues and enhancing the long-term outcomes of the surgical intervention [23,24]. These techniques included:
• Manual Treatment: Application of massage and stretching protocols to promote joint mobility and tissue flexibility.
• Balance and Proprioceptive Exercises: Activities designed to enhance proprioception and stability, crucial for improving limb function and gait.
Therapeutic Exercises: Prescribed exercises targeting specific muscle groups to promote strength and en-durance.
Aquatic Treadmill Therapy: Utilization of an aquatic treadmill to facilitate low-impact exercise, fostering muscle conditioning and joint mobilization.
Super-Pulsed Class I Laser Therapy: Utilization of the ACTIVet PRO® device from Multi Radiance Medical (Solon, OH, USA) for laser therapy sessions. This therapy is known for its analgesic and anti-inflammatory effects, aiding in pain management and tissue healing. (table2)
Laser therapy is categorized into different classes based on power output and safety considerations. Class 1 lasers, which have a power output generally less than 0.5 milliwatts (mW), are considered safe for use without protective eyewear and pose no significant risk of eye or skin damage [25,26].
Class 3R lasers, with a power output of up to 5 milliwatts (mW), present a low risk of eye injury with normal use; however, protective eyewear is recommended in certain conditions to ensure safety [25,26].
Class 3B lasers, ranging from 5 to 500 milliwatts (mW), carry a potential risk of eye damage if directly viewed. Therefore, protective eyewear is necessary to prevent injury.
Class 4 lasers, which exceed 500 milliwatts (mW), have a high risk of eye and skin damage. As such, strict safety protocols and the use of protective eyewear are mandatory when working with these lasers [25,26].
These classifications are crucial for determining the appropriate laser type for various therapeutic applications and ensuring the safety of both patients and practitioners [25,26].

Table 2: This Table Shows the Characteristics of the Laser Active Pro
Recent studies indicate that various physical therapeutic modalities can contribute to the conservative or post-surgical treatment of Canine Hip Dysplasia (CHD) in dogs. Physiotherapy induces biological effects through physical action mechanisms, triggering biochemical responses in the body. The primary therapies recommended for individuals with osteoarthritis include laser therapy, due to its analgesic effects and low-impact exercises on an underwater treadmill.
Materials and Methods
Patient Details A 7-Year-Old Male Canine Setter, 23 kg was the Subject of this Study

Figure 2: Pre-Surgery X-ray (Lateral Position) Showing Bilateral Coxofemoral Dysplasia and the Presence of Metallic Artifacts (Lead Pellets from a Firearm with which the Animal was Unfortunately Shot)
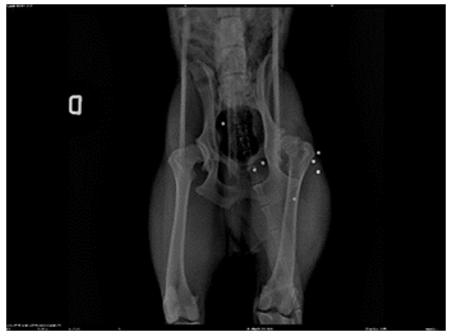
Figure 3: Pre-Surgery X ray -(Ventro Dorsal Position) Showing Bilateral Coxofemoral Dysplasia and the Presence of Metallic Artifacts (Lead Pellets from a Firearm with which the Animal was Unfortunately Shot
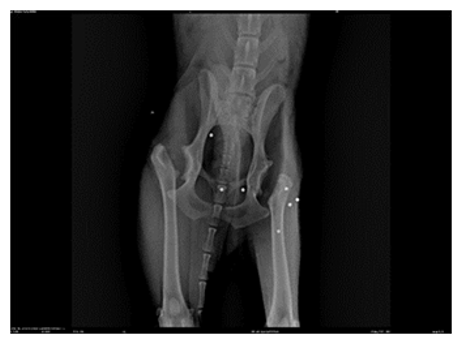
Figure 4: X-ray After the Second Surgery -(Ventro Dorsal Position) with Bilateral Excision of the Femoral Head and Neck
In Figures 2 and 3, we observe the bilateral coxofemoral joint in a ventrodorsally and lateraly view, where severe bilateral coxofemoral joint incongruence is noted, with evident femoral head luxation in the left limb. The presence of osteophytes along the acetabular margins and bilateral atrophy of the thigh muscles are also observed. In Figure 4, the absence of the coxofemoral joint is evident, showing the radiograph following the second surgery, where bilateral ostectomy was performed. The presence of acetabular osteophytes and bilateral atrophy of the thigh muscles is highlighted
History
The canine was discovered abandoned near the municipal kennel and subsequently rescued. Following a medical examination and X-rays, the dog was diagnosed with severe coxofemoral dysplasia, necessitating femoral head ostectomy due to joint dislocation (Figures 2 and 3). The initial surgery took place in March 2022 the left limb followed by a subsequent procedure in August 2022. (figure4)for the rigth limb.
The treatment chosen for this patient (bilateral ostectomy) was the decision of the surgeon, as well as the decision to start physiotherapy two months after the last surgery.
Between the two surgeries, no rehabilitation procedures were performed; only anti-inflammatory (non-steroidal anti- inflammatory drugs) and antibiotics were administered. The patient was referred for physiotherapy evaluation late (two months after the second surgery) because it was not walking well, exhibiting a grade four lameness, difficulty in rising and sitting, and in positioning to urinate. As the medical therapy was ineffective, the patient was referred for rehabilitation.
Assessment
In October 2022, when the physiatric consultation was conducted to initiate the physiotherapy process, the patient exhibited pelvic extension pain, gluteal muscle atrophy, quadriceps and biceps femoris contractures, iliopsoas muscle contracture, thoracolumbar spine pain, and joint capsule retraction (on joint palpation, a sensation of 'cavitation' or changes in resistance were noted, along with a reduction in the range of joint motion, signs of inflammation such as pain, edema, and increased temperature, and resistance during joint stress maneuvers). The dog demonstrated difficulty in sitting and standing. Goniometric measurements indicated left hip flexion of 48º and extension of 158º, and right hip flexion of 47º and extension of 157º (normal flexion being 50º and extension 162º) [12]. Goniometry was consistently performed with the same goniometer, with the patient in lateral recumbency, depending on the limb being assessed. For instance, to measure the angles of the right pelvic limb, the patient was positioned in left lateral recumbency (with the left limb resting on the floor).
Even though a reduction of 4–5 degrees in the extension angle may seem relatively modest, it is important to recognize that this small change can have a meaningful impact on the biomechanics of the dog. Even slight reductions in joint extension can influence how forces are distributed during movement, affecting overall gait and mobility [11,12].
In clinical terms, this minor reduction can significantly impact the dog's ability to perform certain activities and may contribute to a decrease in overall mobility and comfort. The biomechanical adjustments resulting from this change can alter the way the dog bears weight and moves, potentially leading to compensatory changes that affect other parts of the body [11,13].
Therefore, while a 4–5 degree change might appear minor, it can have clinically relevant effects on the dog's movement patterns and functional abilities. Addressing these changes through appropriate management and rehabilitation can help mitigate any negative impacts and support improved mobility and quality of life for the dog [11,13,27].
Circumference measurements of the thigh were 28 cm (right) and 29 cm (left). Circumference measurements were taken with a Gulick (fig. 6) tape measure, which accurately tracks muscle mass circumference values over the course of treatment. The device must always be positioned in the same location. The balls in the spring tension area become visible when tension is applied to the tape measure, ensuring that a constant tension is maintained during measurements. The Gulick was consistently positioned at 70% of femoral length, and measurements were performed with the patient in a standing position.

Figure 6: Gulick [28] 31

Figure 7: Illustration of Canine Hip Goniometry in Flexion (A) and Extension (B) [13] 57
Methods
The patient was referred by a fellow surgeon, already having undergone bilateral ostectomy; therefore, no surgical authorization or consent for invasive therapies was requested.
The treatment plan comprised 20 physiotherapy sessions utilizing the ACTIVet PRO® laser (Multi Radiance Medical, Solon, OH, USA) for pain and osteoarthritis management, aquatic treadmill for muscular rein-forcement, Additionally, Alevica® 1 tablet per day for 60 days (Palmitoylethanolamide (30%), mono- and diglycerides of fatty acids esterified with organic acids (diglyceride of benzoic acid), sodium pyrophosphate, yeast, lupin flour, sodium chloride, sunflower seed oil, magnesium salts of organic acids (stearate)) was ad-ministered for pain control, and Condrostress® 1 tablet per day for 60 days (Egg membrane (10.8%), mono- and diglycerides of fatty acids esterified with organic acids (benzoic acid), sodium pyrophosphate, inactivated yeast, lupin protein flour, sodium chloride, vegetable oils (sunflower seeds), magnesium salts of organic acids (stearic acid) Nutritional additive: Vitamin E (42916 mg/kg). Coloring agent: 2a104 (2500 mg/kg). was pre- scribed to enhance cartilage hydration and synovial fluid viscosity in degenerative diseases such as coxofemoral dysplasia.
Rehabilitation sessions included super-pulsed laser therapy and aquatic treadmill exercises administered twice weekly for two months, followed by once-weekly sessions for the final two weeks. The primary goals of laser therapy were to expedite healing, control inflammation and pain, and alleviate muscle contractures. Specific laser treatments were targeted at pain in the thoracolumbar region, chronic pain at the surgical site, and pectineus muscle contracture.
Super-pulsed laser therapy, also known as cold laser therapy, represents a revolutionary advancement in technology. This therapy utilizes a technology called 'super pulsing,' which offers a safer and more effective treatment compared to traditional methods, such as Class IV lasers, due to its lack of thermal output (classified as Class 1). This innovative super-pulsing technology facilitates deeper tissue penetration than lasers of the same wavelength and power output. The absence of heat production enhances patient comfort, eliminates the need for specialized rooms or equipment, and allows the laser to be maintained in a single position for optimal treatment. Continuous movement of the laser is unnecessary. The scope of this case report is to assess whether this technology can be used over metallic implants without causing overheating or burns.
Laser treatment aimed to control pain in the thoracolumbar spine was performed in all sessions at 1000 Hz for 5 minutes, in direct contact, with the emitter moved slowly (1 cm per second) across the thoracolumbar region to stimulate endorphin release. For chronic pain and inflammation at the surgical site, treatment was applied during the first two weeks once pain subsided, at 50 Hz around the joint where the femoral head would be, in direct contact without trichotomy, scanning for 10 minutes. To manage pectineus muscle contracture, treat-ment was applied in all sessions at 1000- 3000 Hz in static mode, with the laser in direct contact with the muscle, also without trichotomy, for 5 minutes. All applications utilized the pulsed mode with both red and infrared lights, using the dome probe.
Hydrotherapy sessions progressed through different water levels: hip joint level during the first two weeks, totaling 4 sessions (two sessions per week) of 10 minutes each; mid-femur level during the subsequent sessions, totaling 4 sessions (two sessions per week) of 15 minutes each; and knee-deep water for the remaining sessions, totaling 12 sessions (two sessions per week) of 20 minutes each. Significant improvements were noted in muscle contracture, range of motion, and weight-bearing in the hind limbs after the fourth session figure 8

Figure 8: Hydrotherapy Last Session
The surgical procedure aims to create a false joint or pseudoarthrosis, which allows for the development of a fibrous joint capsule and reduces the abnormal stresses and pressures that were present before the surgery. Consequently, this leads to a decrease in pain and improvement in function, as the pressure that was previously causing discomfort is alleviated [11,23,24].
The assessment of improvements in muscle contracture and intra-articular pressure (post-surgery) was con-ducted clinically, as imaging techniques such as ultrasonography and pressure sensors were not available. For evaluating muscle contracture, the examination begins with palpation of the affected muscles. The veterinarian assesses the firmness, texture, and length of the muscles, which should become progressively less rigid and more elastic. Subsequently, the range of motion (ROM) is evaluated; a reduction in ROM can indicate muscle contracture. Passive movements of the joints help identify limitations and muscular resistance. To observe improvements, we need to see an enhancement in ROM and evaluate the joint angles using goniometry. Additionally, muscle strength assessments, such as resistance to passive and active movements, help identify areas of weakness or rigidity. Stretching tests are also performed to check the muscle’s ability to stretch and return to its normal position. Restrictions during stretching may indicate muscle contracture [11,23,29].
Physiotherapy continued for two months to restore muscle mass, improve joint amplitude, and achieve total pain control. Condrostress® was administered indefinitely to enhance the quality of the remaining joints, given that the coxofemoral joint no longer exists. The surgical procedure aims to create a false joint or pseudoarthrosis, which allows for the development of a fibrous joint capsule and reduces the abnormal stresses and pressures that were present before the surgery. Consequently, this leads to a decrease in pain and improvement in function, as the pressure that was previously causing discomfort is alleviated [11, 23,24].
The assessment of improvements in muscle contracture and intra-articular pressure (post-surgery) was con-ducted clinically, as imaging techniques such as ultrasonography and pressure sensors were not available. For evaluating muscle contracture, the examination begins with palpation of the affected muscles. The veterinarian assesses the firmness, texture, and length of the muscles, which should become progressively less rigid and more elastic. Subsequently, the range of motion (ROM) is evaluated; a reduction in ROM can indicate muscle contracture. Passive movements of the joints help identify limitations and muscular resistance. To observe improvements, we need to see an enhancement in ROM and evaluate the joint angles using goniometry. Additionally, muscle strength assessments, such as resistance to passive and active movements, help identify areas of weakness or rigidity. Stretching tests are also performed to check the muscle’s ability to stretch and return to its normal position. Restrictions during stretching may indicate muscle contracture [11,23,24].
Results
In the last evaluation, the patient exhibited no signs of pain and demonstrated ease in sitting and standing. The post-surgery treatment effectively restored the patient's function and quality of life. Radiographic assessment revealed no developmental signs of osteoarthritis and an increase in muscle mass.
Significant improvements were observed in muscle contracture and joint pressure after the fourth session.
The owner reported substantial improvement, indicating that the patient is no longer hesitant to walk, sit, or stand.
Thigh perimetry measurements showed improvement, with the right thigh measuring 30 cm and the left thigh measuring 31 cm.
And in the measurements [30]
1. Goniometry of the left coxofemoral joint pre-treatment: flexion 48º extension 158º (normal flexion 50º extension 162º) Post treatment flexion 50º extension 160º
2. Goniometry of the right coxofemoral joint pre-treatment: flexion 47º extension 157º (normal flexion 50º extension 162º) Post treatment flexion 50º extension 159º
3. Pre-treatment perimeter left thigh 28 cm left thigh 29 cm
4. Post treatment Right thigh perimetry 30 cm; left thigh 31 cm. The change in angulation was not very large but was significant, as was the change in perimeter measurements. This small alteration was sufficient to observe clinical improvement and almost complete physiological recovery in goniometry (when compared to the normal values referred to in the publications) [12,13].3.1. Figures

Figure 5: X-ray after the Second Surgery. -(Ventro Dorsal Position) with Bilateral Excision of the Femoral Head and Neck Post 10 Session, Where you Can See Greater Muscle Mass in Relation to Photo 04
Discussion
The evolution of rehabilitation has provided substantial scientific evidence supporting the effectiveness of non-surgical interventions for treating hip dysplasia, especially in cases without joint luxation. This case report highlights the importance of rehabilitative measures even after corrective surgery. Surgical techniques such as osteotomy, denervation, or prosthesis placement do not address alterations in soft tissues like muscles and the joint capsule. Therefore, integrating pre- and post-surgery physiotherapy into all hip dysplasia treatment protocols is crucial for enhancing and accelerating patient recovery.
In this context, the use of super pulsed lasers is particularly noteworthy. Unlike continuous-wave lasers, super pulsed lasers do not generate significant heat during application. This characteristic is essential for patients with metallic artifacts, such as those resulting from firearm injuries, as it reduces the risk of thermal injury to surrounding tissues. The therapeutic effects of super pulsed lasers are achieved without heating, making them safe for use in the presence of metallic artifacts that could otherwise complicate treatment if heated.
In this study, a clinically relevant improvement was observed, with a 2 cm increase in thigh circumference. Although the increases in muscle circumference and goniometric measurements were relatively small, they are significant because they approach the anatomical values described in the literature and the normal values for the patient. This improvement in thigh circumference, along with enhanced joint angulation, contributes to better overall biomechanics. By increasing muscle mass and improving joint alignment, the patient’s overall movement and functionality are enhanced, leading to more effective rehabilitation and recovery. Incorporating super pulsed laser therapy into the rehabilitation protocol effectively addresses soft tissue alterations and supports these improvements, aligning with the goal of comprehensive rehabilitation and emphasizing the role of advanced technologies in optimizing patient outcomes.
Conclusions
Recent studies have established the efficacy of various physical therapeutic modalities in the conservative and post-surgical treatment of canine coxofemoral dysplasia (CFD) [18,28,31]. Physiotherapy utilizes biological mechanisms that trigger biochemical responses in the body. Laser therapy, known for its analgesic effects, is recommended for managing pain, while low- impact exercises on a hydro treadmill are beneficial for individuals with osteoarthritis [25,32-37].
Hydrotherapy is particularly effective in managing joint conditions due to the buoyancy of water, which reduces the relative weight of the animal and decreases joint overload [38,39]. The increased density of water provides more resistance to muscle activity than air, making underwater treadmills and swimming ideal for arthritic animals [40,27]. These exercises also play a significant role in the multimodal treatment of canine obesity, contributing to better weight management and less joint impact [27,26,40,38]. Additionally, the thermal effect of heated water promotes relaxation and improves joint mobility [31,41].
In this study, treatment began with water levels set at the coxofemoral joint to maximize buoyancy and minimize overload, which aimed to improve range of motion and pain control. As treatment progressed, water levels were increased to mid-femur and then knee-depth to enhance resistance and stimulate muscle growth [31,41].
Laser therapy further complements this approach by controlling joint pain and chronic conditions. It operates through photobiomodulation of the inflammatory response, enhancing cellular ATP synthesis and transforming inflammatory mediators to exert anti-edematous and anti-inflammatory effects [42]. Notably, super pulsed laser therapy poses minimal risk, as it does not cause burns or abrasions and is safe to use even with the presence of metallic implants, such as lead pellets from previous injuries. This safety profile allows for effective pain management and anti- inflammatory benefits without contraindications [11].
In summary, the integration of hydrotherapy and laser therapy in the treatment of CFD proves effective in addressing muscle contractures, improving joint extension, and enhancing overall strength. These interventions significantly contribute to the quality of life for canine patients. To validate and expand on these findings, further studies and comparative analyses of various treatment modalities, including both conservative and surgical approaches, are recommended [15,16,18].
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
Thank you for the support from the University of Teramo and for the support and as-sistance from Multi Radiance. I thank the reviewers from Multi Radiance for their valuable assistance in reviewing this manuscript
References
- Bettini CM, et al. (2007). Incidence of coxofemoral dysplasia in Border Collie dogs. Unipar Veterinary and Zoological Sciences Archive, 10(1), 21-25.
- Minto, B. W., Souza, V. D., Brandão, C. V. S., Mori, E. S., Morishin Filho, M. M., & Ranzani, J. J. T. (2012). Clinical evaluation of acetabular denervation in dogs with hip dysplasia attended at veterinary hospital of FMVZ-Botucatu-SP.
- Rocha FPC, et al. (2008). Coxofemoral dysplasia in dogs.Revista Cientí Eletrônica de Medicina Veterinária, 4(11), 1-7.
- Henrigson, B., Norberg, I., & OLSSONS, S. E. (1966). On the etiology and pathogenesis of hip dysplasia: a comparative review. Journal of Small Animal Practice, 7(11), 673-688.
- Mostafa, A. A., Berry, C. R., & Nahla, M. A. (2023). Quantitative assessment of hip mor-phology to enhance the identification of hip dysplasia in German Shepherd Dogs. American Journal of Veterinary Research, 84(3).
- Harper, T. A. (2017). Conservative management of hip dysplasia. Veterinary Clinics: Small Animal Practice, 47(4), 807-821.
- Honmura, A., Yanase, M., Obata, J., & Haruki, E. (1992). Therapeutic effect of Gaâ?Alâ?As diode laser irradiation on experimentally induced inflammation in rats. Lasers in surgery and medicine, 12(4), 441-449.
- McLauglin, R. J., & Tomlinson, J. (1996). Radiographic diagnosis of canine hip dysplasia.
- Crestani, M. V., Telõken, M. A., & Gusmão, P. D. F. (2006). Impacto femoroacetabular: uma das condições precursoras daosteoartrose do quadril. Rev. bras. ortop, 285-293.
- MVS Hospital for Pets. Hip Dysplasia. MVS Hospital for Pets.
- Matera, J. M., Tatarunas, A. C., & Oliveira, S. M. (2003). Uso do laser arseneto de gálio (904nm) após excisão artroplástica da cabeça do fêmur em cães. Acta Cirúrgica Brasileira, 18, 102-106.
- Nganvongpanit, K., Boonchai, T., Taothong, O., & Sathanawongs, A. (2014). Physiological effects of water temperatures in swimming toy breed dogs. KAFKAS ÜNÄ°VERSÄ°TESÄ° VETERÄ°NER FAKÜLTESÄ° DERGÄ°SÄ°, 20(2).
- Petazzoni, M., & Jaeger, G. H. (2008). Atlas of clinical goniometry and radiographic measurements of the canine pelvic limb. Merial.
- Virag Y, Gumpenberger M, Tichy A, Lutonsky C, Peham C, Bockstahler B. (2022). Center of pressure and reaction forces of the soil in Labradors and Golden Re-trievers with and without coxofemoral dysplasia at 4, 8 and 12 months of age. Front Vet Sci. Dec 22(9):1087693.
- Doust, S. J., Rajabioun, M., Mehrjerdi, H. K., & Mirshahi, A. (2018). Preliminary study of the hip dysplasia incidence based on clinical and radiographical examination in large breed dogs referred to veterinary teaching hospital of Ferdowsi University of Mashhad.
- Edge-Hughes, L. (2007). Hip and sacroiliac disease: selected disorders and their man-agement with physical therapy. Clinical techniques in small animal practice, 22(4), 183-194.
- Diniz R. (2018).Ortopedia, displasia coxofemural. In: Lopes RS, Diniz R, editors. Fisiatria em Pequenos Animais. São Paulo: Editora Inteligente, 156-162.
- Duff, R., & Campbell, J. R. (1977). Long term results of excision arthroplasty of the canine hip. The Veterinary Record, 101(10), 181-184.
- McCarthy, G., O’Donovan, J., Jones, B., McAllister, H., Seed, M., & Mooney, C. (2007). Randomised double-blind, positive-controlled trial to assess the efficacy of glucosa- mine/chondroitin sulfate for the treatment of dogs with osteoarthritis. The Veterinary Journal, 174(1), 54-61.
- Brown, D. C., Boston, R. C., Coyne, J. C., & Farrar, J. T. (2008). Ability of the canine brief pain inventory to detect response to treatment in dogs with osteoarthritis. Journal of the American Veterinary Medical Association, 233(8), 1278- 1283.
- Gomes, M. V. F., Rahal, S. C., Santos, I. F. C. D., Dadalto, C.R., Mamprim, M. J., Negrão, R. R., ... & Gómez Álvarez, C. B. (2023). Long-Term Effects of Whole-Body Vibration on Hind Limb Muscles, Gait and Pain in Lame Dogs with Borderline- to-Severe Hip Dyspla-sia—A Pilot Study. Animals, 13(22), 3456.
- Kyriazis, A., & Prassinos, N. N. (2016). Canine hip dysplasia: part i: aetiopathogenesis & diagnostic approach. Hellenic Journal of Companion Animal Medicine, 5(1), 22-47.
- Zink, C., & Van Dyke, J. B. (2018). Canine Sports Medicine and Rehabilitation.
- Engstig, M., Vesterinen, S., Morelius, M., Junnila, J., &Hyytiäinen, H. K. (2022). Effect of femoral head and neckosteotomy on canines’ functional pelvic position and locomo- tion. Animals, 12(13), 1631.
- Cardinet, G. H., Kass, P. H., Wallace, L. J., & Guffy, M. M. (1997). Association between pelvic muscle mass and canine hip dysplasia. Journal of the American Veterinary Medical Association, 210(10), 1466-1473.
- Prankel, S. (2008). Hydrotherapy in practice. In practice,30(5), 272-277.
- König, H. E., & Liebich, H. G. (2021). Anatomia dos animais domésticos-: Texto e atlas colorido. Artmed Editora.
- Ginja, M. M. D., Silvestre, A. M., Gonzalo-Orden, J. M., & Ferreira, A. J. A. (2010). Diag-nosis, genetic control and preventive management of canine hip dysplasia: a review. The Veterinary Journal, 184(3), 269-276.
- Piermattei D. (2011). Arthroplasty for excision of the coxofemoral joint in dogs and cats. Vet Comp Orthop Traumatol, 24(1):89.
- Baker, S. G., Roush, J. K., Unis, M. D., & Wodiske, T. (2010). Comparison of four com-mercial devices to measure limb circumference in dogs. Veterinary and comparative Or- thopaedics and traumatology, 23(06), 406-410.
- Millis, D. L., & Levine, D. (1997). The role of exercise and physical modalities in the treatment of osteoarthritis. Veterinary clinics of north america: small animal practice, 27(4), 913-930.
- Ali, Q., Paneh, A., Banoo, A., & Saami, S. (2018). Low energy laser effects in relieving pain in patients with knee osteoarthritis. International Journal of Medicine and Public Health, 2(1), 6-10.
- Jaegger, G., Marcellin-Little, D. J., & Levine, D. (2002). Reliability of goniometry in Lab-rador Retrievers. American journal of veterinary research, 63(7), 979-986.
- Bockstahler, B., Kräutler, C., Holler, P., Kotschwar, A., Vobornik, A., & Peham, C. (2012). Pelvic limb kinematics and surface electromyography of the vastus lateralis, biceps femoris, and gluteus medius muscle in dogs with hip osteoarthritis. Veterinary Sur-gery, 41(1), 54-62.
- Bockstahler, B. A., Prickler, B., Lewy, E., Holler, P. J., Vobornik, A., & Peham, C. (2012). Hind limb kinematics during therapeutic exercises in dogs with osteoarthritis of the hip joints. American journal of veterinary research, 73(9), 1371-1376.
- Cartlidge, H. (2015). Hydrotherapy for the osteoarthritic dog: why might it help and is there any evidence?. The Veterinary Nurse, 6(10), 600-606.
- Mendes, S., Coutinho, M. I., & Rebelo, P. (2015). Hidroterapia canina. Revista Portuguesa de Ciências Veterinárias, 110(595- 596), 160-164.
- Chauvet, A., Laclair, J., Elliott, D. A., & German, A. J. (2011). Incorporation of exercise, using an underwater treadmill, and active client education into a weight management program for obese dogs. The Canadian Veterinary Journal, 52(5), 491.
- Denning, W. E., Bressel, E., & Dolny, D. G. (2010). Underwater treadmill exercise as a potential treatment for adults with osteoarthritis. International journal of aquatic research and education, 4(1), 9.
- REUSING, M. S. D. O. (2019). EFEITOS TERAPÊUTICOS DO EXERCÍCIO EM ESTEIRA AQUÁTICA E DA LASERTERAPIA DE BAIXA INTENSIDADE EM CÃES COM DISPLASIA COXOFEMORAL.
- Morales, J. A., Ruiz-Gómez, M. J., Gil-Carmona, L., Souviron, A., & Martínez-Morillo, M. (1995). He-Ne laser has no effect on cell cycle phases of human colon adenocarcinoma cells. Journal of Physiology and Biochemistry, 51(1), 43-47.
- Bjordal, J. M., Couppé, C., Chow, R. T., Tunér, J., & Ljunggren, E. A. (2003). A systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders. Australian journal of physiotherapy, 49(2), 107-116.
- Mueller, M., Bockstahler, B., Skalicky, M., Mlacnik, E., & Lorinson, D. (2007). Effects of radial shockwave therapy on the limb function of dogs with hip osteoarthritis. Veterinary Record, 160(22), 762-765.
- Morgan, J. P., Wind, A., & Davidson, A. P. (2000). Elbow dysplasia. Morgan JP, Wind AP, Davidson AP: Hereditary bone and joint diseases in the dog. Schlutersche GmbH, Hannover, 41-94.
- Off, W., & Matis, U. (2010). Excision arthroplasty of the hip joint in dogs and cats. Veterinary and Comparative Orthopaedics and Traumatology, 23(05), 297-305.
- Barr, A. R. S., Denny, H. R., & Gibbs, C. (1987). Clinical hip dysplasia in growing dogs: the longâ?term results of conservative management. Journal of Small Animal Practice, 28(4), 243-252.
- Bender, T., Nagy, G., Barna, I., Tefner, I., Kadas, E., & Geher,P. (2007). The effect of physical therapy on beta-endorphin levels. European journal of applied physiology, 100, 371-382.
- Collard, F., Maitre, P., Quang, T. L., Fau, D., Carozzo, C., Genevois, J. R., ... & Viguier, E. (2010). Canine hip denervation: comparison between clinical outcome and gait analysis.
- Diniz R. Hidroterapia. (2018). In: Lopes RS, Diniz R, editors. Fisiatria em Pequenos Animais. São Paulo: Editora Inteligente, p. 156-162.
- Eginton, K. A., & Gordon-Evans, W. J. (2024). Lifetime cost of surgical treatment for canine hip osteoarthritis is less than conservative management in dogs under eight years of age. Journal of the American Veterinary Medical Association, 1(aop), 1-5.
- Greshake, R. J., & Ackerman, N. (1993). Ultrasound evaluation of the coxofemoral joints of the canine neonate. Veterinary Radiology & Ultrasound, 34(2), 99-104.
- Gulick Tape Measure. (n.d.). VBS Group. Retrieved August 4, 2024.
- Gusi, N., Tomasâ?Carus, P., Häkkinen, A., Häkkinen, K., & Ortegaâ?Alonso, A. (2006). Ex-ercise in waistâ?high warm water decreases pain and improves healthâ?related quality of life and strength in the lower extremities in women with fibromyalgia. Arthritis Care & Research: Oficial Journal of the American College of Rheumatology, 55(1), 66-73.
- Lai, D., Zhou, S., Cheng, S., Liu, H., & Cui, Y. (2022). Laser therapy in the treatment of melasma: a systematic review and meta-analysis. Lasers in Medical Science, 37(4), 2099-2110.
- Lewis, G., & Cert, S. H. B. S. H. P. (2018, October). The Effects of Low-level Laser Therapy on the Gait of the Osteoarthritic Canine Hindlimb. In BVNA Congress 2018.
- Nielsen, C., & Pluhar, G. E. (2005). Diagnosis and treatment of hind limb muscle strain injuries in 22 dogs. Veterinary and Comparative Orthopaedics and Traumatology, 18(04), 247-253.
- Parkinson, S., Wills, A. P., Tabor, G., & Williams, J. M. (2018). Effect of water depth on muscle activity of dogs when walking on a water treadmill. Comparative Exercise Physiology, 14(2), 1-12.
- Pereira, F. C., Parisi, J. R., Maglioni, C. B., Machado, G. B., Barragánâ?Iglesias, P., Silva, J. R., & Silva, M. L. (2017). Antinociceptive effects of lowâ?level laser therapy at 3 and 8 j/cm2 in a rat model of postoperative pain: Possible role of endogenous Opioids. Lasers in surgery and medicine, 49(9), 844-851.
- Piotti, P., Albertini, M., Lavesi, E., Ferri, A., & Pirrone, F. (2022). Physiotherapy improves dogs’ quality of life measured with the Milan pet quality of life scale: is pain in-volved?. Veterinary Sciences, 9(7), 335.
- Raghuvir, H. B., Shivrajsinh, K. J., Dipak, N. S., Harit, D. B., Chirag, A. B., & Naresh, H. K. (2013). Treatment of canine hip dysplasia: a review. J. Anim. Sci. Adv, 3(12), 589-597.
- Remedios, A. M., & Fries, C. L. (1995). Treatment of canine hip dysplasia: a review. The Canadian Veterinary Journal, 36(8), 503.
- Saleh, M. S., Shahien, M., Mortada, H., Elaraby, A., Hammad,Y. S., Hamed, M., & Elshennawy, S. (2024). High-intensity versus low-level laser in musculoskeletal disor-ders. Lasers in Medical Science, 39(1), 179.
- Syrcle, J. (2017). Hip dysplasia: clinical signs and physical examination find-ings. Veterinary Clinics: Small Animal Practice, 47(4), 769-775.
- Reusing, M., Brocardo, M., Weber, S., & Villanova Jr, J. (2020). Goniometric evaluation and passive range of joint motion in chondrodystrophic and non-chondrodystrophic dogs of different sizes. VCOT Open, 3(02), e66-e71.
- Reusing, M.S.O. (2019). Therapeutic Effects of Underwater Treadmill Exercise and Low-Level Laser Therapy in Dogs with Hip Dysplasia. Master's Thesis, Pontifícia Universidade Católica do Paraná, School of Life Sciences, Graduate Program in Animal Science, Curitiba, Brazil.
- Tai, G., Tai, M., & Zhao, M. (2018). Electrically stimulated cell migration and its contribution to wound healing. Burns & trauma, 6.
- Upariputti, R., Vijarnsorn, M., Niyom, S., & Boonyong, S. (2018). Effect of interferential current therapy on ground reaction force in dogs with hip osteoarthritis: A randomized placebo controlled cross-over clinical trial. The Thai Journal of Veterinary Medicine, 48(1), 111-116.
- Vince, K. J. (2007). Canine hip dysplasia: surgical treatment for the military working dog. Army Medical Department Journal, 44-50.
- Wallace, L. J. (1992). Pectineus tendon surgery for the management of canine hip dys-plasia. Veterinary Clinics of North America: Small Animal Practice, 22(3), 607-621.
- Weigel, J. P., Cartee, R. E., & Marich, K. W. (1983). Preliminary study on the use of ul-trasonic transmission imaging to evaluate the hip joint in the immature dog. Ultrasound in medicine & biology, 9(4), 371-378.
- Wong, E. (2011). Swim to recovery: canine hydrotherapy healing. Veloce Publishing Ltd.
- Zink, C., & Carr, B. J. (2018). What is a canine athlete?. Canine sports medicine and re-habilitation, 1-22.
- Alvarez, L. X., Repac, J. A., Kirkby Shaw, K., & Compton,N. (2022). Systematic review of postoperative rehabilitation interventions after cranial cruciate ligament surgery in dogs. Veterinary Surgery, 51(2), 233-243.