
Open Access Journal of Disease and Global Health(OAJDGH)
ISSN: 2993-6594 | DOI: 10.33140/OAJDGH
Impact Factor: 0.9


Research Article - (2024) Volume 2, Issue 1
Addressing the Role of Health Professions Students in Ebola Response Through Community Mobilization
2Seed Global Health, Boston, Massachusetts, United States
3Emergency Care Society of, Uganda
Received Date: Nov 24, 2024 / Accepted Date: Dec 25, 2024 / Published Date: Mar 28, 2024
Copyright: ©2024 Elvis Tamale, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Tamale, E., Nankya, S., Mulungi, J., Malinga, P., Mshilla, M., et. al. (2024). Addressing the Role of Health Professions Students in Ebola Response Through Community Mobilization. Ope Acce Jou Dis Glo Heal, 2(1), 01-11.
Abstract
Background: Uganda faced a 4-month Ebola Virus Disease (EVD) outbreak from September 2022 to January 2023, resulting in significant mortality, morbidity, and stigma. Health professions students, including frontline workers, played a crucial role in managing epidemics through community interventions. This project, led by health professional students, aimed to enhance prevention, preparedness, and response to current and future EVD epidemics in Mbarara.
Methods: A descriptive cross-sectional study was conducted, utilizing needs assessment tools developed based on WHO information on EBV and past COVID-19 recommendations. Trained undergraduates and postgraduates collected data on knowledge, attitudes, and perceptions regarding EVD from 220 participants, including health professions students, healthcare providers, and community members. Information, Education, and Communication (IEC) materials were distributed in various locations, accompanied by community sensitization in the local language.
Results: Survey participation was gender-balanced, with 94.7% of respondents aware of EBVD. Market vendors and traders showed higher awareness, primarily through radio (75.3%) and television (65.3%). While participants believed face masks could prevent Ebola, awareness campaigns clarified its non-airborne nature. Significant knowledge gaps were identified, especially among community leaders, regarding signs, symptoms, and proper personal protective equipment for handling suspected Ebola cases.
Conclusion: Epidemics, marked by morbidity and mortality, demand functional health systems and robust epidemic readiness. Health professions students, offering a substantial workforce, prove essential in epidemic response. Addressing knowledge gaps through targeted education and preparedness efforts is critical for effective community engagement and epidemic control.
Keywords
Ebola Virus Disease, Health Professions Students, Health Professions Students Against Ebola (HEPSE), Epidemic Response.
Introduction
Epidemics are devastating as they cause mortality, morbidity and are associated with extraordinary demands on the healthcare system [1]. Uganda experienced an outbreak of Ebola virus disease (EVD) declared by Ministry of Health (MoH) Uganda on 20th September 2022 and ending On 11 January 2023 [2]. Ebola Virus, a member of the filoviridae family, is a highly contagious viral hemorrhagic infection with a high mortality rate of up to 90% [3]. Initially, the rapid communicability and high mortality rates of Ebola virus disease presented multiple challenges to clinicians, health facilities, and national health sectors. These burdened healthcare workers encountered complex challenges in managing the increased number of suspected patients with Ebola virus disease while diagnosing those with other infectious diseases of similar clinical presentation, such as cholera, dengue, malaria, or typhoid fever.
Health profession students form a part of frontline providers in managing the epidemic through community interventions targeting prevention, preparedness, and emergency response [4]. They are usually the first to receive suspects and cases during triage and clinical clerkship, strategically placing them as spreaders (forming a gap) and controllers (forming a potential solution) of epidemics such as EVD.
These same students are surrounded by a community of non- health professionals, academic and support staff, as well as civilians in common gathering places like churches and markets. These places are high-risk sites for EVD transmission since it is contagious [5]. In most epidemics, civilians have inadequate knowledge of disease recognition and prevention as well as the reporting mechanisms on suspects [6]. As with previous studies on the COVID-19 pandemic, health profession students have the capacity to support the response to health catastrophes like this epidemic [7]. These students are involved in patient care, are custodians of knowledge in their communities and avail a large workforce that can be leveraged [8]. The untimely demise of our colleagues at the frontline sparked us into action backed up by our numbers and our impact on the communities we often visit as custodians of health. Community engagement within health is crucial to achieving primary health care and promoting people- centered services as well as contributing to health systems responsiveness and strengthening [9- 12].
The resurgence of EVD and continuously registered cases beyond Mubende called for greater emphasis on the empowerment of the community, health profession students, and health workers. This project was therefore directed towards prevention, preparedness, and response to the current and future EVD epidemics within Mbarara and beyond.
This project provided an avenue for capacity building, and health information dissemination as well as availing crucial information for stakeholders on any gaps. The findings provided some potential strategies that can enable communities to follow health standards during similar outbreaks. Furthermore, this information may be utilized by the Ministry of Health in resource-limited settings to strengthen emergency response and prevent future epidemics.
As part of the community engagement IEC materials approved by the Ministry of Health Uganda were distributed and community outreaches to carry out baseline surveys.
Methods
A group of 21 undergraduates and postgraduate (Emergency medicine) students had a refresher on EVD to enable evidence- based communication among the potential participants they approached.
We assessed the knowledge, attitudes, and perceptions of health professions students, health care providers, and communities. In the communities, we mapped areas of perceived risk and through community leadership such as DHO Mbarara City, and institutional leaders through a physical meeting held at the DHO office. Part of the team met the Dean Faculty of Medicine online who represented MUST Faculty of Medicine as well as the director of MRRH. We met community leaders before approaching any member in the mapped areas. We reached out to these mapped areas and carried out baseline surveys using printed questionnaires.
After establishing the baseline, we pinned up Information, Education, and Communication (IEC) materials on EVD in hospitals, markets, worship centers and institutional premises parallel with sensitization of community members on the information on the flyers in the local language.
Key Stakeholders
In an African society, community entry and exit is key as it enables the researcher to leave behind more sustainable solutions from the desirable goals set out by the team.
• University administrators (5)
• Hospital administrators (1)
• District leaders (5)
• Community leaders and focal persons:
• Religious leaders (Catholic, Anglican, Moslem, and Pentecostal): 8
• Market leaders (Kola nolya, Rwebikona, and Central market Mbarara): 6
• Various Bodaboda stage leaders in Mbarara: 15
• Global Buses franchise leadership: 2
• Mbarara Bus and Taxi Park leaders:
Students
The team consisted of 21 students who were distributed daily according to the mapped areas focusing on 5 major area categorizations. In each area, the focus was on places of convergence such as markets, religious places, and bus and taxi parks. There was a focus on bodaboda riders as they were found to be critical in spreading information in the community. The students were sent in teams of 3 to each area. Each team had someone in charge of data collection and transcription.
Our study tool was informed by information shared by the World Health Organization
Course on Ebola Virus Disease as well as tools adapted from studies done during the COVID-19 pandemic. It focused on describing knowledge, attitudes, and perceptions of EBV as well as identifying gaps in epidemic response.
This needs assessment involved four main phases based on the objectives.
Phase 1: Researcher Training
Phase one involved the health professions students having a refresher course on Ebola Virus Disease in order to enable evidence-based communication with the potential participants they approach. The refresher course was tailored to the information from the World Health Organization course on Ebola Virus Disease. They were trained in how to use Information, Education, and Communication materials to engage with the community. They were also trained on how to ethically collect data from the community on their knowledge, attitudes and practices towards Ebola.
Phase 2: Mapping
Phase two consisted of reviewing suspect charts or registers at MRRH and health centers in Mbarara Health region for information on the socio-demographics, health characteristics, and common disease hotspots especially for past epidemics. It also involved engaging the District Health Office to map potential disease hot spot areas as well as convergence points in the community. Other sources of this information included community organizations working with the District Health Office and the Ministry of Health, which were identified by the DHO.
Phase 3: FGDs, KIs, Electronic Data Collection
Key leaders in the different community places were interviewed about their knowledge, attitudes and perceptions during the Ebola Virus Disease epidemic as well as community response in case of a suspected case.
Data was collected using an electronic form and we had a minimum of 2 abstractors who consulted the key abstractor (the principal investigator) in case of any conflicts? The perspectives of the community, providers, and students were obtained through focus group discussions (FGDs) and in-depth interviews (IDIs) to better identify and discuss their knowledge, attitudes, and perceptions. We chose to use two different data collection methods to improve the accuracy of data collected, minimize biases arising from weaknesses associated with particular single methods, provide a comprehensive picture of our topic of interest and allow triangulation of findings.
Focus group discussions consisted of 5 - 8 study participants in Mbarara. Each FGD had one moderator or facilitator, a timekeeper, and a field notes taker/observer who would take observational notes during the discussions and summary notes after each focus group discussion.
Each FGDs lasted approximately 20 -30 minutes which is within the range of time focus group interviews have been shown to usually last for about 1–2 hours, based on the complexity of the topics under investigation, number of questions, and participants [13]. IDIs took on average 10 - 20 minutes depending on the topic, interviewer, and interviewee, which duration is within the range of average time for healthcare interviews [14]. In one-to- one interviews, the interviewer endeavored to make summary notes of each interview through memorization. We also had a notes taker for recording the interview outcomes.
Interview schedules for both the FGDs and IDIs contained questions that explored community knowledge, attitudes, and perceptions. These questions invited participants to share their experiences.
PHASE 4: IEC Distribution
We used information, education, and communication material in the form of posters and flyers highlighting the cause of EBV, how it is contracted, symptoms, case definition, and what to do if suspected if met with a suspect or contact. These were posted and distributed in designated areas in the community, at MRRH, and in health facilities within Mbarara after seeking permission from relevant authorities.
We had a stratified study sample with separate groups of community sets such as market vendors, motorcyclists, health workers, and traders representing the community in Mbarara.
Findings and Discussion
We visited 5 major areas in Mbarara city and educated more than 1000 people on the mode of spread, signs and symptoms, and prevention of Ebola virus disease (EBVD). We also interviewed 380 persons in the community to establish baseline knowledge about EBVD. All interviewed people provided verbal consent.
These people interviewed reflected the areas we visited and included: Market vendors, bodaboda riders, cobblers, waitresses, shopkeepers, charcoal sellers, Religious leaders, salonists, butcher men, community nurses, and drug sellers among others. The interviews focused on community leaders and ensured that various categories of the population were reached so as to have a clear picture of the knowledge, attitudes, and perceptions among the community population sects.
There were slightly more males, 50.3% (191/380), and the majority of the respondents, 94.7% (360/380) had heard about EBVD. However, there was considerable heterogeneity in the baseline knowledge with some interviewed persons having no knowledge about EBVD. Even among those who had previously heard about EBVD, there were considerable myths and misinformation.
The females in the community had heard more about EBVD (51.6%) than males. Amongst both males and females, the market vendors and traders had heard more about EBVD. Figure 2 details the different community population sects, their gender and if they had heard about Ebola.
|
Have you heard about Ebola? |
|||||||
|
|
No |
Yes |
|
||||
|
Occupation |
Female |
Male |
Total |
Female |
Male |
Total |
Grand Total |
|
Trader |
|
2 |
2 |
22 |
19 |
41 |
43 |
|
Banker |
|
|
|
2 |
1 |
3 |
3 |
|
Bodaboda rider |
|
2 |
2 |
|
35 |
35 |
37 |
|
Chairman LC1 |
|
|
|
1 |
5 |
6 |
6 |
|
Cobbler |
|
|
|
|
1 |
1 |
1 |
|
Customer |
|
|
|
|
1 |
1 |
1 |
|
Grocery |
|
|
|
7 |
3 |
10 |
10 |
|
Health worker |
1 |
|
1 |
17 |
12 |
29 |
30 |
|
Market vendor |
2 |
4 |
6 |
52 |
23 |
75 |
81 |
|
Police officer |
|
|
|
1 |
4 |
5 |
5 |
|
Religious leader |
|
|
|
5 |
2 |
7 |
7 |
|
Restaurant |
|
|
|
8 |
5 |
13 |
13 |
|
Saloonist |
1 |
|
1 |
3 |
2 |
5 |
6 |
|
Student |
|
|
|
6 |
9 |
15 |
15 |
|
Supermarket |
|
|
|
2 |
|
2 |
2 |
|
Tailor |
|
|
|
6 |
2 |
8 |
8 |
|
Grand Total |
4 |
8 |
12 |
132 |
124 |
256 |
268 |
Figure 1: Have you heard about Ebola
Among the respondents 0.3% had never heard about Ebola virus disease while 0.3% didn't know if they have ever heard about Ebola.
Among the respondents who had ever heard about Ebola virus disease, the most common source of information as reported by the respondents was radio stations (75.3%) followed television (65.3%). Other sources of information included social media, friends and family. Frequencies of other sources of EBVD information are shown in figure 3.

Figure 2: Sources of Ebola Information
The most commonly reported mode of spread of EBVD was touching an infected person (reported by 85% of respondents). Unexplained bleeding was the most commonly reported symptom of EBVD (80.3%). In contrast, the early symptoms such as fever, headache and muscle pain were less commonly reported (61.6%, 46.8% and 26.6% respectively) as shown in Figure 4 below. 84.7% of the population knew at least 2 symptoms with only 23.7% knowing more than 2 symptoms.

Figure 3: Signs and Symptoms of Ebola
Only 194/380 (51%) knew to call in case they suspected a person to have EBVD. 20% knew who to call and what number to call; Most people would call the police first in cases of a suspected EBVD case.
|
Community response in case of an EBVD suspect |
|||||||
|
|
No |
Yes |
|
||||
|
Occupation |
Female |
Male |
Total |
Female |
Male |
Total |
Grand Total |
|
Trader |
3 |
2 |
5 |
11 |
8 |
19 |
24 |
|
Banker |
|
|
|
2 |
1 |
3 |
3 |
|
Bodaboda rider |
|
6 |
6 |
|
20 |
20 |
26 |
|
Chairman LC1 |
|
|
|
1 |
3 |
4 |
4 |
|
Grocery |
|
|
|
6 |
1 |
7 |
7 |
|
Health worker |
|
|
|
14 |
11 |
25 |
25 |
|
Market vendor |
6 |
1 |
7 |
15 |
7 |
22 |
29 |
|
Police officer |
|
|
|
1 |
3 |
4 |
4 |
|
Religious leader |
|
|
|
4 |
2 |
6 |
6 |
|
Restaurant |
1 |
1 |
2 |
3 |
1 |
4 |
6 |
|
Saloonist |
|
|
|
2 |
|
2 |
2 |
|
Student |
|
1 |
1 |
5 |
6 |
11 |
12 |
|
Supermarket |
|
|
|
2 |
|
2 |
2 |
|
Tailor |
3 |
|
3 |
3 |
1 |
4 |
7 |
|
Grand Total |
13 |
11 |
24 |
69 |
64 |
133 |
157 |
Figure 4: Response in Case of an EBVD Suspect
Other information including knowledge of the modes of EBVD spread and methods of prevention was also collected.
We found that some people held a belief that Ebola could be prevented by wearing face masks. We educated them that Ebola is not an airborne illness like Covid-19. However, we asserted that wearing face masks is important to prevent spread of COVID-19.
People in the community were receptive to the education and many requested for similar education about other epidemic diseases such as cholera, COVID-19 and others. In addition, community members appreciated the smartness of the medical students and their safety precautions through wearing masks and having hand sanitizers.
We found myths that EBVD could be spread through insects, especially grasshoppers. We re-assured the community that this wasn’t evidence based. There were also circulating stories of a family of 7 people who contracted EBVD after exhuming their dead EBVD victim to re-bury them according to traditional rituals. This story was cited by many people as the reason they started taking EBVD seriously. It also reasserted the ministry of health guideline to bury EBVD victims by trained burial teams.
We observed a challenge of inadequate hand-washing stations in
many of the places we visited, especially market places. Many of them lacked hand-washing stations at entry and exit points, despite the Ministry of Health emphasizing hand-washing as a preventive strategy to prevent spread of EBVD. Surprisingly, we found that some community health workers interviewed lacked knowledge of the presenting signs and symptoms of EBVD. In addition, many did not know the standard personal protective equipment needed before handling a person suspected to be infected with Ebola. In some health settings the key personnel in charge were reluctant; An intern scared of handling an EBVD suspect (Patient was bleeding from the eyes) consults with the Infectious disease expert who just glances once and says,” that cannot be EBVD” and walks away. They advised that CMEs be organized to educate them about EBVD. Amongst the 228 health care workers and health profession students who filled the online tool, the respondents reflected different specialties and cadres in the healthcare profession: Nurses, Medical Officers, Pharmacists, Clinical Officers, Family Physicians, Public Health Specialists, Social workers, Pediatricians, Emergency Medicine Physicians, Rehabilitation specialists, Physiotherapists, Entomologists, Laboratory Technicians, Midwives, Interns and Various health professional Students among others. The survey focused on ensuring that various categories of the population are reached so as to have a clear picture of the knowledge, attitudes and perceptions. There were slightly more males 62.7% (143/228) and the majority of the respondents, 99.1% (226/220) had heard about EBVD with the commonest source of information from the online tool respondents being social media (86%) followed by television (68.4%). Frequencies of other sources of EBVD information are shown in figure 6 below.

Figure 5: Sources of Ebola Information from Online Respondents
Concerning how to approach an EBVD suspect, 59.2% of the respondents were sure of what to do, 21.1% didn't know and 19.7% were not sure.
<img src=" https://www.opastpublishers.com/scholarly-images/7232-6937aaa19afb4-addressing-the-role-of-health-professions-students-in-ebola-.png" width="500" height="200">
Figure 6: How to Approach an Ebola Suspect
63.6% of the respondents knew how to appropriately use Personal Protective Equipment in an EBVD suspect environment but only 33.3% had access to the appropriate Personal Protective Equipment as seen in Figure 6 below.
<img src=" https://www.opastpublishers.com/scholarly-images/7232-6937aae5e14c6-addressing-the-role-of-health-professions-students-in-ebola-.png" width="500" height="200">
Figure 7: Knowledge on PPE use
Only 29.4% of the respondents were not afraid of EBVD as shown in Figure 7
<img src=" https://www.opastpublishers.com/scholarly-images/7232-6937ab23a538b-addressing-the-role-of-health-professions-students-in-ebola-.png" width="500" height="200">
Figure 8: Attitude towards Ebola Suspect from Online Respondents
There were significant gaps in baseline knowledge about Ebola among different categories of people interviewed. This can probably be explained by different levels of formal education and accessibility to information. However, a small proportion of the population didn’t have any knowledge about the disease, underscoring the need to disseminate such information to the lowest community level. Notably, a significant number of people considered information about the spread, presentation, and prevention of COVID-19 to be the same as that for Ebola. The influence of workplaces on awareness is yet to be determined. Myths and misconceptions are probably derived from already existing information about previous pandemics like COVID-19, personal beliefs, and misinterpretation of information picked from the media about Ebola.
The most common source of information reported by the community participants was radio followed by television which emphasizes the need for awareness campaigns to mainly focus on the aforementioned platforms. In particular, social media informed a smaller number of people than normally expected. It’s probably used more by people of higher education backgrounds and socio-economic status. Most importantly, a significantly small proportion of the participants reported getting information from friends and family, highlighting the need to encourage the population to actively take part in sharing credible information about Ebola.
Furthermore, the majority of the respondents knew about a touch of body fluids of an infected person as a mode of spread. However, other modes of spread were less reported. This could probably be caused by gaps in information being shared through media platforms. It is crucial that every aspect of daily life that can contribute to the spread of Ebola is emphasized while broadcasting such information. Surprisingly, a section of health workers lacked some information about the presentation and PPE used in Ebola prevention which highlighted the need for immediate training of this particular group in the face of the pandemic given they are the frontline team that handles suspected and confirmed cases.
Study Limitations
Our study has several limitations. It did not categorize the population sections and sample them accordingly which could have one population section participate more than another. Consequently, we may not have captured the full range of perspectives and opinions within the faculty regarding mentoring.
Conclusion
Epidemics are devastating and associated with a lot of morbidity and mortality. Functional Health systems with proper surveillance, epidemic readiness, response, and readiness are a necessity to combat epidemics. Health professions students provide a necessary large workforce that can be utilized in epidemic response.
Annex
Annex 1: Photo Album

A Subgroup of the HEPSE Team Educating Vendors at Kora Nolya Market

A Member of the Team Putting up Flyer at a Boda Stage in Rwebikoona
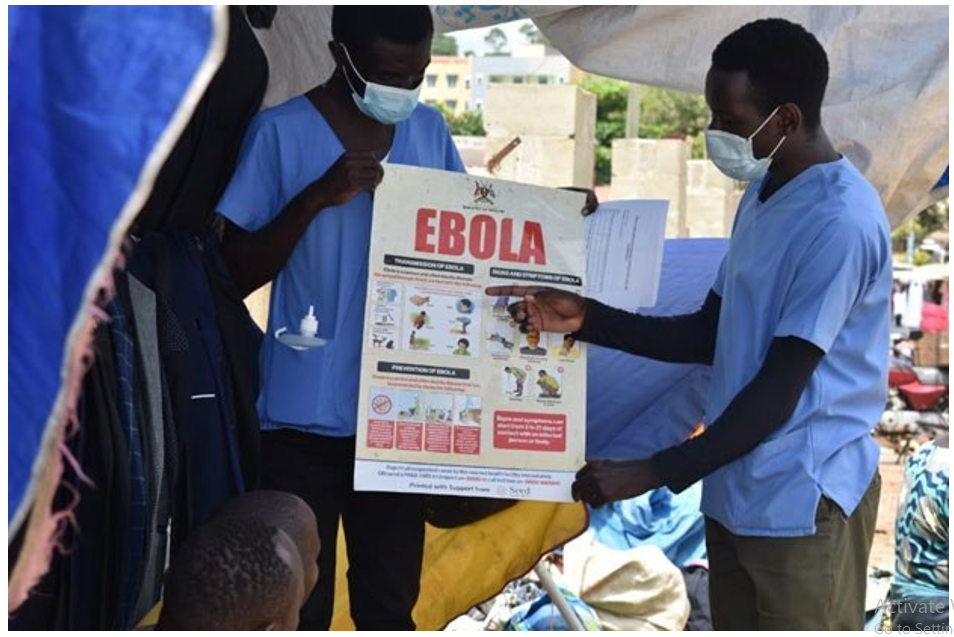
A Subgroup of a Team Teaching Clothes Vendors on Market Day About Ebola

A Team Educating a Lady at Central Market Mbarara about Ebola
Recommendations
Important next steps include; To Researchers: Future studies should explore the capacity of health workers to handle various epidemics as well as the avenues for multi sectorial collaboration in epidemic response
To Medical institutions: Efforts to equip health professions students with knowledge on epidemic surveillance, preparedness, and response
Declaration
acknowledgement
Ethical Approval and Consent to participate
The study was performed as operational research with permission to collect data from participants being granted by the dean of students at MUST. All participants voluntarily gave informed consent to be enrolled in the study enrolment.
Consent to Publish
Not Applicable
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article [and its supplementary information files
Competiting Interest
No financial and non-financial interests declared
Funding
This work was not funded
Author Contributions
Allan Nsubuga TE & PMK developed the idea of the Program TE, JM, SN, and Mkavita MP designed and administered the monitoring and evaluation tools. TE & SN analyzed the data and wrote the first manuscript draft. SN, JM, PM, AN, and PMK reviewed and edited. All authors read and approved the final manuscript.
Acknowledgements
We would acknowledge Dr Joseph Ngonzi, Dean, Faculty of Medicine, MUST, Mbarara District Health leaders, and Seed Global Health for their significant contribution towards the success of this project. We also appreciate the participants of the study
References
- Madhav, N., Oppenheim, B., Gallivan, M., Mulembakani, P., Rubin, E., & Wolfe, N. (2018). Pandemics: risks, impacts, and mitigation.
- Ministry of Health Uganda Reports. (2023).
- World Health Organization. (2021). Healthy and sustainable diets: key workstreams in the WHO European Region: factsheet 2021 (No. WHO/EURO: 2021-2192-41947-57624). World Health Organization. Regional Office forEurope.
- Chapman, H. J., Animasahun, V. J., Tade, A. E., & Naveed,A. (2016). Addressing the role of medical students using community mobilization and social media in the Ebola response. Perspectives on Medical Education, 5, 186-190.
- Verter, F., & Couto, P. S. Newsletter-November 2015.
- Cénat, J. M., Rousseau, C., Dalexis, R. D., Bukaka, J., Derivois, D., Balayulu-Makila, O., & Birangui, J. P. (2021). Knowledge and misconceptions related to the Ebola Virus Disease among adults in the Democratic Republic of the Congo: The venomous snake under the table of prevention.Public Health in Practice, 2, 100178.
- McLean, S., Charlesworth, L., May, S., & Pollard, N. (2018). Healthcare students’ perceptions about their role, confidence and competence to deliver brief public health interventions and advice. BMC medical education, 18, 1-9.
- Stachteas, P., Vlachopoulos, N., & Smyrnakis, E. (2021). Medical students during the COVID-19 pandemic: Considerations and arguments on their clinical engagement. Journal of Advances in Medical Education & Professionalism, 9(4), 238.
- Erku, D., Khatri, R., Endalamaw, A., Wolka, E., Nigatu, F., Zewdie, A., & Assefa, Y. (2023). Community engagement initiatives in primary health care to achieve universal health coverage: A realist synthesis of scoping review. Plos one, 18(5), e0285222.
- Yuan, M., Lin, H., Wu, H., Yu, M., Tu, J., & Lü, Y. (2021).Community engagement in public health: a bibliometricmapping of global research. Archives of Public Health, 79, 1-17.
- Durrance-Bagale, A., Marzouk, M., Tung, L. S., Agarwal, S., Aribou, Z. M., Ibrahim, N. B. M., ... & Howard, N. (2022). Community engagement in health systems interventions and research in conflict-affected countries: a scoping review of approaches. Global Health Action, 15(1), 2074131.
- Odendaal, W., Atkins, S., & Lewin, S. (2016). Multiple and mixed methods in formative evaluation: Is more better? Reflections from a South African study. BMC Medical Research Methodology, 16, 1-12.
- Rabiee, F. (2004). Focus-group interview and data analysis.Proceedings of the nutrition society, 63(4), 655-660.
- Gill, P., Stewart, K., Treasure, E., & Chadwick, B. (2008). Methods of data collection in qualitative research: interviews and focus groups. British dental journal, 204(6), 291-295.