
International Journal of Orthopaedics Research(IJOR)
ISSN: 2690-9189 | DOI: 10.33140/IJOR
Impact Factor: 1.6

Research Article - (2025) Volume 8, Issue 3
Adaptation and Applicability of the Sane Scale in Brazil: Expanding the Use of the Validated Version
2Department of Orthopedics and Traumatology Hospital Nossa Senhora do Pari, Canindé, São Paulo, Brazil
3Department of Orthopedics and Traumatology HCI – Hospital das Clínicas Itajubá, Itajubá, Minas Gerai, Brazil
4Department of Orthopedics and Traumatology Pontifícia Universidade Católica de São Paulo, Campus Sor, Brazil
5Department of Orthopedics and Traumatology HMAP - Hospital Municipal de Aparecida de Goiânia, Aparec, Brazil
6Department of Orthopedics and Traumatology HC/UFG – Hospital das Clínicas, Universidade Federal de G, Brazil
7LAM – Movement Architecture Laboratory UFG – Universidade Federal de Goiás, Goiânia, Goiás, Brazil
Received Date: May 12, 2025 / Accepted Date: Jun 10, 2025 / Published Date: Jul 15, 2025
Copyright: ©2025 Fernanda Grazielle da Silva Azevedo Nora, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nora, F. G. D. S. A., Sales, M. A., De Andrade, S. C. V., Alberti, L. F., Neto, J. C. J., et al. (2025). Adaptation and Applicability of the Sane Scale in Brazil: Expanding the Use of the Validated Version. Int J Ortho Res, 8(3), 01-07.
Abstract
Objective: This study aimed to evaluate the functional recovery trajectory following total knee arthroplasty (TKA) and assess the effectiveness of the adapted M-SANE scale in monitoring post-surgical progress.
Methodology: A cross-sectional observational study was conducted with 120 patients who underwent unilateral primary TKA. Participants were categorized into three groups based on postoperative duration: 30 days, 6 months, and 12 months. Functional recovery was assessed using the M-SANE-DA scale, which evaluates six daily activities. Statistical analyses were performed using Student’s t-test for group comparisons.
Results: The study demonstrated significant functional improvement over time, with Group 3 (12 months post-TKA) exhibiting the highest scores across all activities. The most notable recovery was observed in stair climbing and prolonged standing, with statistically significant differences between groups (p < 0.001). However, tasks such as squatting and getting in and out of a car showed no significant variations, suggesting persistent biomechanical challenges.
Conclusion: The results highlight the importance of structured rehabilitation and long-term physiotherapy for optimizing functional outcomes following TKA. While significant improvements occur within the first year, certain activities require additional rehabilitation focus. The M-SANE-DA scale proved to be a reliable tool for monitoring functional recovery and guiding individualized rehabilitation interventions.
Keywords
Total Knee Arthroplasty, Functional Recovery, Rehabilitation, M-SANE-DA Scale, Physiotherapy
Introduction
The evaluation of joint function is a fundamental component of orthopedics and rehabilitation, being essential for monitoring the recovery of patients undergoing Total Knee Arthroplasty (TKA) [1]. Measuring the patient's perception of their recovery is a relevant aspect of clinical practice, as it complements the objective findings from physical examinations and imaging studies. For this purpose, standardized instruments, such as Patient-Reported Outcome Measures (PROMs), have been widely used, allowing for the collection of quantitative and reproducible data on joint functionality [2].
Among the available PROMs, the Single Assessment Numeric Evaluation (SANE) has gained prominence due to its simplicity and objectivity. This instrument consists of a single question in which the patient evaluates their joint function on a scale from 0 to 100, comparing it to a normal joint [3]. Previous studies have shown that SANE has a strong correlation with more extensive scales, such as the International Knee Documentation Committee (IKDC), the Knee Injury and Osteoarthritis Outcome Score (KOOS), and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), demonstrating its validity and reliability for assessing knee functions after surgical interventions [4].
In Brazil, the cross-cultural adaptation of assessment instruments is essential to ensure their applicability and accuracy in different clinical and population contexts. A literal translation of an instrument is not sufficient to guarantee conceptual equivalence between the original and adapted versions; a rigorous adaptation process is required to prevent linguistic and cultural biases [7,8]. In this regard, a recent study conducted the translation, cross-cultural adaptation, and validation of the SANE scale into Brazilian Portuguese, specifically for patients undergoing TKA [9].
The validation process of the SANE in Brazil followed strict methodological guidelines, including translation, back-translation, review by a committee of experts, and pilot testing with the target population. The results indicated that the Brazilian version of SANE maintained its conceptual equivalence with the original version, being understandable and appropriate for Brazilian patients. Additionally, psychometric tests demonstrated high reliability (Cronbach's Alpha > 0.70) and excellent reproducibility (ICC > 0.75), consolidating the instrument's robustness for measuring joint function in patients undergoing TKA [2].
The cross-cultural adaptation of instruments such as SANE is essential to enable international comparisons and strengthen the evidence base on joint functionality in different populations [6]. Previous studies have shown that SANE has a strong correlation with widely used PROMs in orthopedics, such as KOOS Jr and PROMIS-10, making it an effective tool for capturing changes in joint function over time [1]. Furthermore, its simplicity allows for quick application in clinical practice, facilitating data collection in various settings, from outpatient clinics to rehabilitation centers [5].
Based on the validated version of SANE for Brazil, this study aims to expand its applicability to other clinical contexts, allowing its use in different orthopedic populations. The standardization of this instrument will contribute to obtaining more precise and comparable data, promoting advances in rehabilitation and functional follow- up of patients. Thus, the adoption of the adapted SANE may assist healthcare professionals in making clinical decisions and defining more effective therapeutic strategies, directly benefiting patients in their recovery journey.
Methodology
This study aimed to adapt the M-SANE Scale, previously validated in Brazil, to assess functional recovery in daily activities of patients undergoing Total Knee Arthroplasty (TKA). The adaptation process adhered to international guidelines for cross- cultural adaptation (Beaton et al., 2000; Guillemin et al., 1993), ensuring that the scale maintained conceptual and semantic equivalence while optimizing its applicability for evaluating functional performance in daily tasks.
Participants
This observational cross-sectional study involved 120 participants, all of whom had undergone unilateral primary total knee arthroplasty (TKA). Patients were recruited from specialized orthopedic rehabilitation centers, following predefined eligibility criteria. Participants were divided into three groups based on the postoperative period: Group 1 included patients who had undergone TKA 30 days prior (n = 40); Group 2 consisted of patients who had undergone TKA six months prior (n = 40); and Group 3 comprised those who had undergone TKA 12 months prior (n = 40). The inclusion criteria required participants to be over 60 years of age, to have undergone unilateral primary TKA, and to be actively engaged in a postoperative rehabilitation program. The exclusion criteria included individuals who had undergone bilateral TKA, had neurological disorders, or had cognitive impairments that could interfere with completing the scale.
Ethical Approval
The study was approved by the Research Ethics Committee of the Federal University of Goiás (Opinion No. 6.232.443; CAAE: 69749823.7.0000.5083), following the guidelines of Resolutions No. 466/2012 and No. 510/2016 of the National Health Council (CNS). Furthermore, it complied with the General Data Protection Law (LGPD - Law No. 13.709/2018), ensuring participant privacy and data security.
Cross-Cultural Adaptation Process
The adaptation of the M-SANE Scale for daily activities (M-SANE- DA) followed a structured process of modification and validation. Initially, a panel of specialists, including orthopedic surgeons, physiotherapists, occupational therapists, and researchers in functional assessment, identified key daily activities essential for evaluating functional independence in post-TKA patients. The original M-SANE Scale, which assessed general knee function, was redesigned to focus specifically on functional movements required for activities of daily living (ADLs). This adaptation was based on the translation, cross-cultural adaptation, and validation of the SANE Scale for patients undergoing total knee arthroplasty, as described by Silva Filho et al. (2025) [2].
The modified version of the scale underwent a thorough review by the expert panel to ensure that the selected activities were clinically relevant, culturally appropriate, and easily interpretable by patients. A semantic validation phase was then conducted,involving a focus group of 40 post-TKA patients who assessed the clarity, comprehensibility, and relevance of each item. Based on patient feedback, minor linguistic adjustments were made before finalizing the M-SANE-DA Scale.
M-SANE-DA Functional Assessment and Scoring System
The M-SANE-DA Scale quantitatively assesses functional recovery in daily activities using a numerical scale ranging from 0 to 100. Participants self-report their ability to perform six essential daily tasks, rating each on a scale from 0, representing complete functional impairment, to 100, indicating full functionality without pain or restriction. The final score is determined by evaluating each activity individually, assigning a score from 0 to 100 based on the patient’s perception of their functional capacity. The overall M-SANE-DA score is then obtained by calculating the mean of the six individual ratings, with higher scores reflecting better functional recovery and greater independence in daily life. Table 1 presents the M-SANE-DA Functional Assessment Form, which was utilized for data collection and clinical evaluation.
The M-SANE-DA Scale was designed as an objective and standardized tool for assessing functional independence in patients undergoing post-TKA rehabilitation.
This scale offers several advantages in both clinical and research settings. It provides a quantifiable functional assessment, offering an objective measure of functional recovery in daily activities. Additionally, it enhances rehabilitation monitoring by enabling clinicians and physiotherapists to track progress over time and adjust treatment strategies accordingly. The scale also improves patient-centered care by ensuring that rehabilitation efforts prioritize functional independence and quality of life.
Furthermore, it serves as a standardized outcome measure, facilitating comparative research on TKA recovery across different populations and intervention strategies. By refining the M-SANE Scale to specifically evaluate daily activities, this study contributes to the optimization of functional assessment tools in post-TKA rehabilitation in Brazil. The M-SANE-DA enhances the precision of rehabilitation monitoring,
|
M-SANE-DA – FUNCTIONAL ASSESSMENT FORM FOR DAILY ACTIVITIES POST-TKA |
||
|
Name: |
||
|
Age (Years): |
Gender: |
Surgery Date: |
|
Surgical Side: ( ) Right ( ) Left |
||
|
Post Operative Phase: ( ) 30 Days ( ) 6 months ( ) 12 months |
||
|
FUNCTIONAL ASSESSMENT – M-SANE-DA SCORE |
||
|
INSTRUCTIONS: |
||
|
Rate your ability to perform the following activities compared to a normal, pain-free joint. Score each activity on a 0 to 100 scale, where:
|
||
|
ACTIVITY |
|
|
|
|
SCORE |
|
|
WALKING INDOORS AND SHORT DISTANCES |
|
|
|
CLIMBING AND DESCENDING STAIRS |
|
|
|
STANDING UP AND SITTING DOWN |
|
|
|
GETTING IN AND OUT OF A CAR |
|
|
|
SQUATTING OR BENDING DOWN |
|
|
|
STANDING FOR PROLONGED PERIODS |
|
|
|
Final M-SANE-DA Score (average): |
||
Table 1: M-SANE-DA Functional Assessment Form
Statistical Analysis
The collected data were analyzed using Minitab statistical software (version 26.0). The Kolmogorov-Smirnov test was applied to assess data normality. Reliability of the scale was evaluated through Cronbach’s Alpha coefficient, with values above 0.70 considered acceptable for internal consistency. Inter- rater agreement was measured using the intraclass correlation coefficient (ICC). For group comparisons, Student’s t-test was used for independent samples, while the Mann-Whitney test was applied for non-parametric data. A significance level of p < 0.05 was adopted for all statistical analyses.
Results
Table 2 presents a comparative analysis of functional activities among elderly patients who underwent total knee arthroplasty (TKA) at different postoperative periods. The evaluated activities include walking indoors and short distances, climbing and descending stairs, standing up and sitting down, getting in and out of a car, squatting or bending down, and standing for prolonged periods. The values are expressed as mean scores with standard deviation, and the statistical significance (p-value) was determined using appropriate statistical methods.
|
Evaluated Activity |
Group 1 |
Group 2 |
Group 3 |
p-value |
|
Walking Indoors and Short Distances |
84.3 |
78.94 |
98.13 |
< 0.001* |
|
Climbing and Descending Stairs |
92.61 |
96.08 |
96.12 |
< 0.001* |
|
Standing Up and Sitting Down |
87.48 |
95.83 |
93.54 |
< 0.001* |
|
Getting in and Out of a Car |
83.83 |
84.38 |
95.19 |
0.187 |
|
Squatting or Bending Down |
88.24 |
96.75 |
95.19 |
0.452 |
|
Standing for Prolonged Periods |
87.48 |
95.83 |
93.54 |
< 0.001* |
|
Legend: Group 1: Elderly patients who underwent TKA 30 days ago; Group 2: Elderly patients who underwent TKA 60 days ago; Group 3: Elderly patients who underwent TKA 12 months ago. Values are presented as mean ± standard deviation; The p-value was calculated using appropriate statistical methods. |
||||
Table 1: Comparison of Functional Activities among Evaluated Groups
The table presents a comparative analysis of functional activities among three groups of elderly patients who underwent total knee arthroplasty (TKA) at different postoperative periods: Group 1 (30 days post-TKA), Group 2 (6 months post-TKA), and Group 3 (12 months post-TKA). The evaluated activities include walking indoors and short distances, climbing and descending stairs, standing up and sitting down, getting in and out of a car, squatting or bending down, and standing for prolonged periods. The values represent the mean performance scores for each group, and the statistical significance (p-value) was calculated to determine differences between the groups.
Patients in Group 3 (12 months post-TKA) demonstrated the highest mean score (98.13), indicating significant functional recovery over time. Group 1 (30 days post-TKA) scored 84.3, while Group 2 (6 months post-TKA) had a lower score of 78.94. The p-value (< 0.001) suggests a statistically significant improvement in walking ability over time. This finding highlights the importance of long-term rehabilitation in regaining mobility.
Patients in Groups 2 (96.08) and 3 (96.12) showed similar scores, both significantly higher than Group 1 (92.61). The p-value (< 0.001) indicates a significant difference among the groups. This suggests that stair-climbing ability improves notably after the early postoperative period, likely due to muscle strengthening and balance recovery.
The results indicate a significant increase in functional ability over time in Standing Up and Sitting Down. Group 2 (95.83) exhibited the highest score, slightly above Group 3 (93.54), while Group 1 (87.48) had the lowest. The p-value (< 0.001) confirms that the observed differences are statistically significant. This improvement reflects better quadriceps strength and joint stability as rehabilitation progresses.
This activity Getting in and Out of a Car showed minimal variation across groups, with Group 3 (95.19) performing slightly better than Groups 1 (83.83) and 2 (84.38). However, the p-value (0.187) suggests that the difference is not statistically significant. This could indicate that getting in and out of a car is an activity that does not heavily rely on the postoperative period but rather on factors such as flexibility and coordination.
There Squatting or Bending Down was no significant difference among the groups in squatting or bending down, as reflected by the p-value (0.452). Group 2 (96.75) had the highest mean score, followed by Group 3 (95.19) and Group 1 (88.24). These results suggest that even after prolonged recovery, squatting remains a challenging task for many TKA patients, possibly due to joint stiffness or discomfort.
A Standing for Prolonged Periods significant improvement over time was observed for this activity, with Group 2 (95.83) and Group 3 (93.54) achieving higher scores than Group 1 (87.48). The p-value (< 0.001) indicates a statistically significant difference. This suggests that endurance and weight-bearing capacity improve significantly with rehabilitation and time post-surgery.
Figure 2 illustrates the comparative analysis of functional recovery among groups over time. The data demonstrates the progressive improvement in functional capacity, with Group 3 (12 months post- TKA) achieving higher scores in most evaluated activities. The use of distinct colors for each group allows for clear differentiation and better visualization of trends.
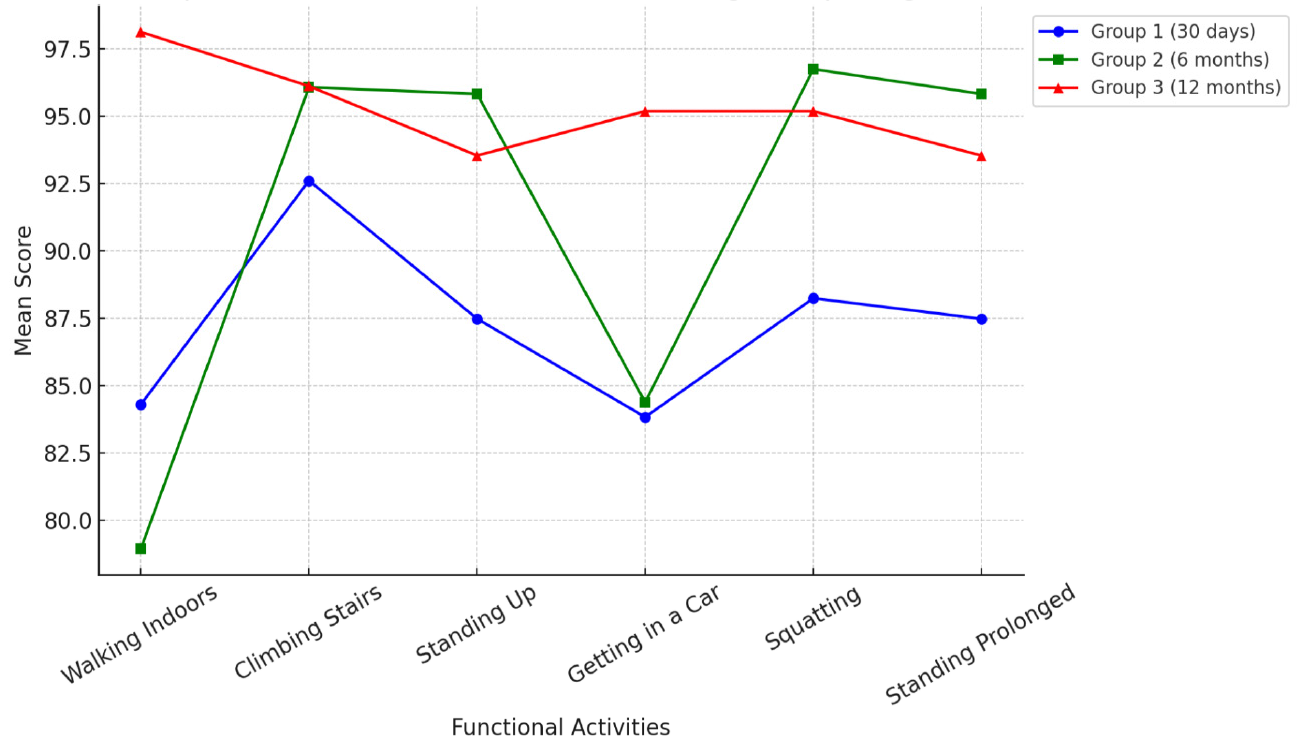
Figure 2: Comparison of Functional Activities among Groups
Discussion
The findings of this study align with existing literature, demonstrat- ing that functional recovery after total knee arthroplasty (TKA) follows a progressive improvement trajectory over time. Research indicates that knee functionality significantly improves within the first-year post-surgery, with the most substantial gains occurring in the initial six months (Sonesson et al., 2021) [10]. The statistically significant differences observed between the evaluated groups em- phasize the necessity of continuous physiotherapeutic intervention to optimize recovery and enhance long-term functional outcomes (Gutierrez-Zúñiga et al., 2021; Winterstein et al., 2013) [4].
The limitations observed in Group 1 (30 days post-TKA) can be attributed to the acute effects of surgery, including pain, edema, and muscle weakness, which hinder the execution of demanding functional activities [10]. These results are consistent with studies showing that the initial postoperative period is critical, as targeted rehabilitation protocols can significantly influence long-term recovery [11]. Torchia et al. (2020) similarly emphasized the role of structured physiotherapy programs in accelerating functional improvements [9].
Vogel et al. (2020) found that structured rehabilitation during the first postoperative month significantly reduces pain and improves mobility. This supports the necessity of immediate physiotherapeutic interventions to prevent muscle atrophy and joint stiffness. The lower performance of Group 1 in activities such as walking indoors and short distances (84.3) and standing for prolonged periods (87.48) highlights the impact of the early postoperative period on mobility and endurance [12].
The functional improvements observed in Group 2 (6 months post-TKA) reflect advancements in motor control and muscle strengthening due to rehabilitation. Patients at this stage demonstrate greater functional independence, which is consistent with previous studies indicating accelerated recovery between the second and third postoperative months (Kvist et al., 2020) [13]. Marques (2020) emphasized that targeted exercise programs during this period enhance stability and range of motion, facilitating smoother transitions to more advanced rehabilitation phases. The mean score for walking indoors and short distances (78.94) aligns with reported values in similar studies, reinforcing the benefits of adherence to postoperative rehabilitation programs (Vogel et al., 2020).
Near-complete recovery in Group 3 (12 months post-TKA) corroborates research suggesting that full functional rehabilitation is typically achieved within one year following surgery. Studies indicate that patients adhering to structured and progressive rehabilitation protocols experience superior functional outcomes and are more likely to resume daily and recreational activities (Fomin et al., 2020; Marques, 2020) [14]. Additionally, research by Austin et al. (2020) and O’Connor et al. (2019) supports the reliability of the SANE scale as a valid tool for monitoring long- term recovery [8].
Return to physical activities remains a significant concern for TKA patients. O’Connor et al. (2019) found that patients engaged in long-term physiotherapy programs achieved higher functional scores, particularly in dynamic activities such as stair climbing and prolonged standing. These findings align with the present study, where Group 3 participants demonstrated superior performance in all measured activities, with significant gains in climbing and descending stairs (96.12) and standing for prolonged periods (93.54).
Despite general improvements, certain activities did not exhibit statistically significant differences among groups. For example, getting in and out of a car (p = 0.187) and squatting or bending down (p = 0.452) showed no significant changes between postoperative stages, suggesting that these activities may pose additional challenges requiring biomechanical adaptations and prolonged rehabilitation [15]. Similar studies have reported persistent difficulties in high-impact movements, with running scores remaining stable over time due to the knee’s limited capacity to absorb impact forces (Nazari et al., 2020).
Biomechanical adaptations post-TKA remain a crucial area of study. Floyd et al. (2021) observed that some patients continue to experience gait alterations, affecting their ability to perform high-intensity activities [16]. This underscores the importance of incorporating gait retraining exercises into rehabilitation protocols to restore normal biomechanics. Physiotherapeutic strategies, including targeted muscle strengthening, proprioceptive training, and functional re-education, are essential for optimizing safe progression toward full knee functionality (Vines et al., 2016; Marot et al., 2021) [6,17]. Progressive loading and gradual return- to-activity strategies significantly reduce secondary complications and improve long-term joint function (Kvist et al., 2020; Torchia et al., 2020) [9,13].
Patient education is also a critical component of rehabilitation success. Bradbury et al. (2013) emphasized the importance of ensuring that patients understand the necessity of continued physiotherapy to enhance adherence and maximize recovery outcomes [18]. Motivation and social support play crucial roles in rehabilitation adherence, as studies indicate that higher engagement in physiotherapeutic treatment leads to better functional recovery and reduced residual pain [4,15].
Psychosocial factors also influence TKA recovery. O’Connor et al. (2019) found that anxiety and fear of movement could negatively impact rehabilitation outcomes. This suggests that integrating psychological support into the recovery process may further optimize functional improvements. Additionally, long-term follow-up programs are essential to monitor joint function and prevent degenerative changes that may occur even after successful rehabilitation [11].
Standardized assessment tools such as the SANE scale play a fundamental role in tracking recovery progression among TKA patients. Nazari et al. (2020) validated the psychometric properties of the SANE scale, confirming its reliability in evaluating post-TKA functionality. Studies by Austin et al. (2020) also demonstrated strong correlations between SANE scores and other functional assessment measures, making it an effective tool for orthopedic rehabilitation research. Intergroup comparisons using validated tools contribute to the development of more effective physiotherapeutic interventions [5,19-24].
Conclusion
This study highlights the progressive improvement in functional recovery following total knee arthroplasty, with significant gains observed within the first-year post-surgery. The findings emphasize the necessity of structured physiotherapy, early rehabilitation interventions, and patient adherence to long-term recovery protocols. Although substantial improvements were observed across most functional activities, certain tasks, such as getting in and out of a car and squatting, continue to pose challenges, necessitating further research into biomechanical adaptations and rehabilitation strategies. Future studies should explore the integration of personalized rehabilitation programs and technological advancements to optimize patient outcomes. A multidisciplinary approach, including physical therapy, patient education, and psychological support, remains essential for achieving optimal long-term recovery and enhancing the overall quality of life for TKA patients
References
- Austin, D. C., Torchia, M. T., Werth, P. M., Lucas, A. P., Moschetti, W. E., & Jevsevar, D. S. (2019). A one-question patient-reported outcome measure is comparable to multiple- question measures in total knee arthroplasty patients. The Journal of Arthroplasty, 34(12), 2937-2943.
- SILVA FILHO, U.C. et al. (2025). Translation, Cross-Cultural Adaptation, and Validation of the SANE Scale for Patients Undergoing Total Knee Arthroplasty. Revista Brasileira de Fisioterapia, 29(142), 14-19.
- SHELBOURNE, K. D., et al. (2012). Single Assessment Numeric Evaluation method for knee documentation. American Journal of Sports Medicine, 27(5), 571-574.
- Winterstein, A. P., McGuine, T. A., Carr, K. E., & Hetzel, S. J. (2013). Comparison of IKDC and SANE outcome measures following knee injury in active female patients. SportsHealth, 5(6), 523-529.
- Torchia, M. T., Austin, D. C., Werth, P. M., Lucas, A. P., Moschetti, W. E., & Jevsevar, D. S. (2020). A SANE approach to outcome collection? Comparing the performance of single- versus multiple-question patient-reported outcome measures after total hip arthroplasty. The Journal of Arthroplasty, 35(6), S207-S213.
- MAROT, V., et al. (2021). Cross-cultural adaptation and validation of the Single Assessment Numeric Evaluation (SANE) for Brazilian Portuguese-speaking patients undergoing total knee arthroplasty. Revista Brasileira de Ortopedia, 56(3), 302-308.
- Marot, V., Justo, A., Alshanquiti, A., Reina, N., Accadbled, F., Berard, E., & Cavaignac, E. (2021). Simple Knee Value: a simple evaluation correlated to existing knee PROMs. Knee Surgery, Sports Traumatology, Arthroscopy, 29, 1952-1959.
- AUSTIN, M. S., et al. (2019). Patient-reported outcome measures: current status and future directions. Bone & Joint Journal, 101(8), 901-906.
- TORCHIA, M. T., et al. (2020). Use of the Single Assessment Numeric Evaluation (SANE) score to assess postoperative outcomes following total hip and knee arthroplasty. Journal of Arthroplasty, 35(7), 1938-1942.
- Sonesson, S., Gauffin, H., & Kvist, J. (2021). Early knee status affects self-reported knee function 1 year after non-surgically treated anterior cruciate ligament injury. Physical Therapy in Sport, 50, 173-183.
- Gobbi, A., & Francisco, R. (2006). Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: a prospective clinical investigation. Knee Surgery, Sports Traumatology, Arthroscopy, 14(10), 1021-1028.
- Dietvorst, M., Reijman, M., Van Groningen, B., Van Der Steen, M. C., & Janssen, R. P. A. (2019). PROMs in paediatric knee ligament injury: use the Pedi-IKDC and avoid using adult PROMs. Knee Surgery, Sports Traumatology, Arthroscopy, 27, 1965-1973.
- Kvist, J., Filbay, S., Andersson, C., Ardern, C. L., & Gauffin, H. (2020). Radiographic and symptomatic knee osteoarthritis 32 to 37 years after acute anterior cruciate ligament rupture. The American Journal of Sports Medicine, 48(10), 2387-2394.
- Fomin, S., Gauffin, H., & Kvist, J. (2020). Short-term recovery of physical activity and knee function after an acute knee injury. BMJ Open Sport & Exercise Medicine, 6(1).
- Chavez, T. J., Garvey, K. D., Collins, J. E., Lowenstein,N. A., & Matzkin, E. G. (2020). Resilience as a predictor of patient satisfaction with nonopioid pain management and patient-reported outcome measures after knee arthroscopy. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 36(8), 2195-2201.
- Floyd, S. B., Oostdyk, A., Cozad, M., Brooks, J. M., Siffri, P., & Burnikel, B. (2021). Assessing the patient-perceived monetary value of patient-reported outcome improvement for patients with chronic knee conditions. Journal of Patient- Centered Research and Reviews, 8(2), 98.
- Vines, J. B., Aliprantis, A. O., Gomoll, A. H., & Farr, J. (2016). Cryopreserved amniotic suspension for the treatment of knee osteoarthritis. The journal of knee surgery, 29(06), 443-450.
- Bradbury, M., Brosky, J. A., Walker, J. F., & West, K. (2013). Relationship between scores from the Knee Outcome Survey and a single assessment numerical rating in patients with patellofemoral pain. Physiotherapy Theory and Practice, 29(7), 531-535.
- Robins, R. J., Anderson, M. B., Zhang, Y., Presson, A. P., Burks,
R. T., & Greis, P. E. (2017). Convergent validity of the patient- reported outcomes measurement information system's physical function computerized adaptive test for the knee and shoulder injury sports medicine patient population. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 33(3), 608-616.
- Tenan, M. S., Dekker, T., & Dickens, J. F. (2023). An Exploratory Factor Analysis of the National Institutes of Health Patient-Reported Outcomes Measurement Information System and the Single Assessment Numeric Evaluation in Knee Surgery Patients. Military medicine, 188(3-4), 456-462.
- Burton, D. A., Schaefer, E. J., Shu, H. T., Bodendorfer, B. M., & Argintar, E. H. (2021). Primary anterior cruciate ligament repair using suture tape augmentation: a case series of 29 patients with minimum 2-year follow-up. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 37(4), 1235-1241.
- Erasmus, P. J., Pieterse, L., & Dillon, E. (2008). Do patients prefer a unicompartmental to a total knee replacement?. SA Orthopaedic Journal, 7(1), 44-49.
- Li, S., Luo, P., Huang, Y., Xia, H., Wei, W., Wei, W., ... Xu, K. (2022). Retrospective Comparison of Postoperative Fascia Iliaca Block and Multimodal Drug Injection on Early Function of the Knee in Femoral Fractures Using Retrograde Intramedullary Nailing. Pain Research and Management, 2022(1), 7027637.
- Stewart, B. P., Hawthorne, B. C., Dorsey, C. G., Wellington, I. J., Cote, M., Mazzocca, A., & Cote, M. (2023). Reverse shoulder arthroplasty patients younger than 60 years old exhibit lower clinically significant single assessment numeric evaluation (SANE) scores compared to older patients. Cureus, 15(10).