
Japanese Journal of Medical Science(JJMS)
ISSN: 2996-2536 | DOI: 10.33140/JJMS

Case Report - (2024) Volume 2, Issue 2
Acute Aortic Insufficiency
2Hospital Angeles del Carmen Guadalajara, Jal, USA
Received Date: Jul 30, 2024 / Accepted Date: Aug 22, 2024 / Published Date: Aug 29, 2024
Copyright: ©©2024 Jose Fernando Guadalajara-Boo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Guadalajara-Boo, J. F., Hern
Abstract
52-year-old male patient arrives at the emergency room with dyspnea at rest orthopnea, recumbent cough, “blody” expectoration, heart rate 90 per minute, and Blood Pressure 80/50 mmHg, with audible pulmonary crackles at distance, and at the mitral area strong first sound with a grade II systolic murmur with non lisent second sound.
Introduction
Presentation of a Case of Acute Aortic Insufficiency
52-year-old male patient arrives at the emergency room with dyspnea at rest orthopnea, recumbent cough, “blody” expectoration, heart rate 90 per minute, and Blood Pressure 80/50 mmHg, with audible pulmonary crackles at distance, and at the mitral area strong first sound with a grade II systolic murmur with non lisent second sound.
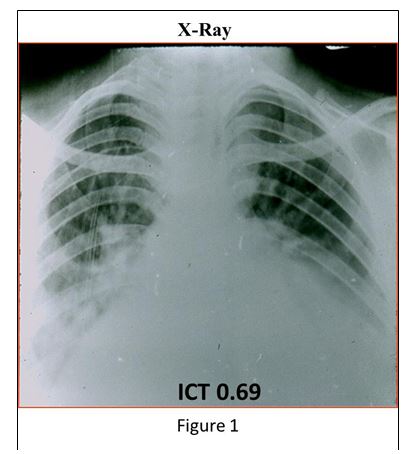
The chest X-Ray shows important enlargement of the heart with pulmonary edema (Figure 1).
The M-mode echocardiogram demonstrates significant dilation of the right ventricle with thinned interventricular septum, great dilation of the left ventricle with thinned posterior wall, and greatly increased LV systolic diameter. The shortening fraction was 23% (figure 2). Conclusion: Severe global heart failure.
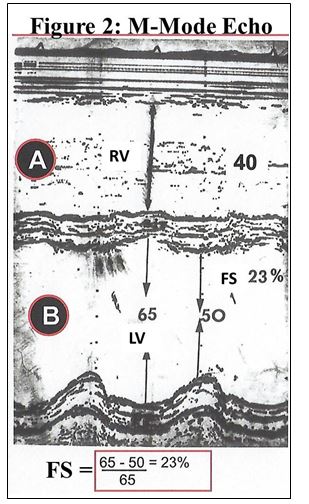
A) The M-Mode Echo recording clearly shows the early closure of the mitral valve, which incontrovertibly establishes the diagnosis of Acute Aortic Insufficiency; I emphasize that with this simple method, the diagnosis of Acute Aortic Insufficiency can be immediately established in an exact, bloodless, fast and cheap manner, which makes it possible to clarify the precise diagnosis to attempt the immediate treatment of this rapidly fatal disease.
B) The simultaneous recording of aortic and left ventricular pressures quantifies the exact levels of intracavitary pressures between the aorta and the left ventricle. In this case, it should be noted that the LV diastolic pressure is combined with the aortic pressure and the D2 of the LV is quantified at 40 mmHg, which explains the very serious situation that the patient presents with acute lung edema in the presence of 40 mmHg. venocapillary pressure; If this condition is not corrected immediately, the patient dies from intractable acute pulmonary edema. (figure 3)
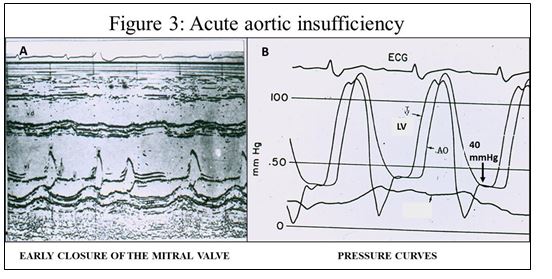
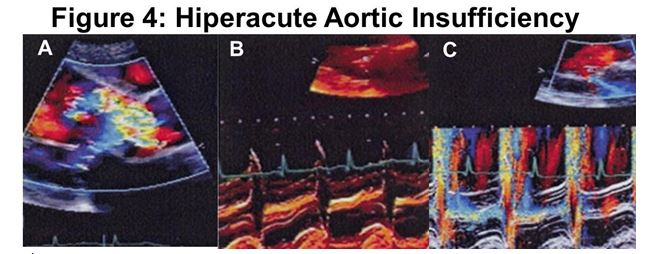
Figure 4:
A) The parasternal long axis view with color-coded Doppler shows that the regurgitant flow covers 90% of the aortic annulus: extreme large aortic insufficiency.
B) Early closure of the mitral valve shows that it is Acute Aortic Insufficiency.
C) Protodiastolic aortic regurgitant flow is demonstrated (colored mosaic). Throughout mitral closure, a mosaic of colors is observed between the two leaflets that begins in the middle of diastole (before the R wave) and continues until the next opening of the mitral valve; That is to say, it is a Diastolic Mitral regurgitant flow: Diastolic Mitral Insufficiency. This is due to the fact that the intraventricular diastolic pressure is so high that it overcomes the mitral valve and allows blood to return during diastole.
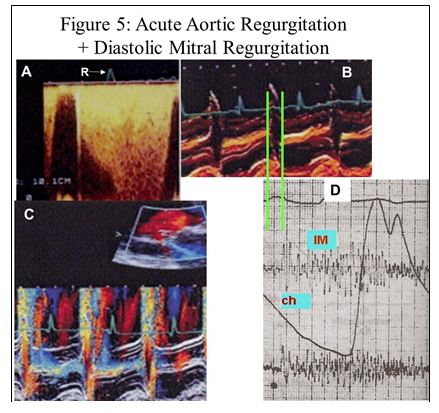
Figure 5:
A) Mitral regurgitation flow that begins before the R wave (see arrow) (diastolic mitral regurgitation).
B) The M-mode echo shows early closure of the mitral valve (green line) that coincides with the onset of the systolic murmur (diastolic mitral regurgitation). Clicking mitral valve closure (Ch) takes the place of a IV sound and is confused with a I sound.
C) Note the mosaic of colors that appears during diastole and reflects diastolic mitral insufficiency.
D) The phonocardiogram shows that the closing click is before the 1st sound which is muted, meaning that it shows that the 1st sound really appears in diastole followed by the mitral regurgitant murmur that begins in diastole until the end of the following
systole. Note the bisferiens carotid pulse (clinical sign of Severe Aortic Insufficiency) and the absence of slit, which speaks of very severe aortic insufficiency (1).
Note: Mitral regurgitation is not only diastolic, see that in the phonocardiogram it is also systolic: 1st known case in which mitral regurgitation is continuous (systolic and diastolic)
The patient was taken to the operating room and died during the transfer.
Conclusion
Acute Aortic Insufficiency is the sudden onset disease that can be considered the most serious in the cardiology clinic due to the rapid evolution towards death. This is why the patient must arrive at the cardiology hospital as soon as possible and The study for diagnosis must be as quick as possible, since, as happened in this patient, all the diagnostic elements were in place until cardiac catheterization was performed to take him to the operating room (2), unfortunately we did not have time to enter surgery. Most frequent etiologies reported in the literature are; acute aortic dissection and infectious endocarditis (3), in the case presented here we had no evidence of either acute aortic dissection or infectious endocarditis, unfortunately when taken to the operating room the patient died and we were not able to have the autopsy study to know the cause of this serious illness.
References
1. Fishleder BL. Exploración cardiovascular y fonomecanocardiografia clinica. 2a Ed. La Prensa Medica Mexicana, Pag. 619.
2. MORGANROTH, J., PERLOFF, J. K., ZELDIS, S. M., & DUNKMAN, W. B. (1977). Acute severe aortic regurgitation: pathophysiology, clinical recognition, and management. Annals of Internal Medicine, 87(2), 223-232.
3. Hamirani, Y. S., Dietl, C. A., Voyles, W., Peralta, M., Begay, D., & Raizada, V. (2012). Acute aortic regurgitation. Circulation, 126(9), 1121-1126.