

Research Article - (2026) Volume 9, Issue 2
A Comprehensive and Preventative Approach to Neurodegenerative Diseases
Received Date: Feb 19, 2026 / Accepted Date: Mar 20, 2026 / Published Date: Apr 01, 2026
Copyright: ©2026 Elham Nourzai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nourzai, E. (2026). A Comprehensive and Preventative Approach to Neurodegenerative Diseases. Adv Neur Neur Sci, 9(2), 01-07.
Abstract
Neurodegenerative diseases, particularly Alzheimer’s disease (AD), pose an unprecedented threat to global healthcare systems and represent a mounting financial burden on modern society. Current projections indicate costs exceeding $2 trillion globally by 2030, with devastating implications for healthcare infrastructure and societal welfare. Leading economists and healthcare experts warn that, if left unchecked, Alzheimer’s will eventually bankrupt our society—a stark reality driven by the exponential growth in cases and the astronomical costs of late-stage care. Despite significant advances in therapeutic research, contemporary approaches remain largely reactive, focusing on late-stage interventions when neurological damage is already extensive and largely irreversible. There is, therefore, a critical and urgent need to revolutionize our approach by shifting towards proactive disease prevention.
This paper presents a comprehensive framework that leverages three key innovations: established and emerging blood-based biomarker technologies, the implementation of AD Prevention Bonds to overcome current reimbursement challenges, aligning economic incentives with preventative care, and groundbreaking insights into molecular pathways— particularly the role of GLP-1 in neuroprotection. Through Zentara’s holistic approach, we demonstrate how early intervention can fundamentally alter disease trajectories whilst simultaneously addressing the economic challenges that currently impede widespread adoption of preventative measures.
Keywords
Quantum Computing, Artificial Intelligence, Biomechanics, Willow Chip, MQT Architecture, Hummingbird, Hamiltonian Simulation
Introduction
Alzheimer's disease (AD) stands out as one of the most pressing challenges in public health today [1]. Beyond the tragic personal toll, caring for AD patients exacts huge financial strains on families and healthcare infrastructures worldwide. In the United States alone, estimates place about 8% of the population in the category of ''biological Alzheimer's'', although only around 2% have fully manifest symptoms. With an average of six years of required care once overt symptoms appear, costs can exceed $1 trillion per annum, scaling toward $3 trillion in the coming decades.Socioeconomic aspects–including lost productivity and the ballooning cost of longterm care–make AD a potential catalyst for a future economic collapse if left unchecked. These trends reveal that a strategy emphasising prevention rather than a late- stage ''cure'' is of paramount importance. Zentara's mission to tackle this goal is guided by three core pillars:
• Systematic risk stratification and early detection.
• Subsidised financial frameworks (''AD bonds'') ensuring broad testing and treatment coverage.
• Novel prophylactic regimens, including the development of our proprietary GLP1-based medication aimed at halting AD progression before it becomes clinically overt.
Why Prevention Over Cure?
The concept of preventing AD from fully manifesting has gained significant traction for two reasons:
• Inherent Biological Limitations: Once severe cortical and hippocampal deterioration occurs, reversing structural brain damage presents an enormous challenge. Even modern, ground-breaking therapies largely struggle to restore lost cognitive function [11, 5].
• Economic Reality: Full-blown AD entails heavy care costs, often spanning multiple years [10]. In contrast, early risk identification and treatment, even if moderately expensive upfront, is a more economically defensible strategy over the long term.
Hence, prioritizing prevention offers a rational path, both scientifically and economically. By halting or slowing neurodegeneration at subclinical phases, individuals effectively avoid years of round-the-clock care and the loss of personal autonomy that harm quality of life.
Aim and Scope of This Paper
This paper synthesizes multiple streams of evidence, from emerging biomarker technologies to new treatment modalities such as GLP-1 antagonists, in presenting Zentara's overarching plan to combat AD. It deliberately integrates socioeconomic analyses, spotlighting how ignoring at-risk populations will likely bankrupt healthcare frameworks in aging societies. Central to our approach is the innovative concept of AD Bonds—financial instruments designed to incentivise early intervention by directly linking investor returns to reduced healthcare costs. Through this novel financing mechanism, we aim to restructure the economic barriers that currently prevent widespread adoption of preventative strategies.
Background on Alzheimers Disease
Alzheimer's disease is pathologically defined largely by the extracellular accumulation of amyloid-beta (Aß) plaques and intracellular tau tangles [30,9]. While there is ongoing debate around whether these protein aggregates are a primary driver or a downstream result of complex biological processes, high amyloid load remains the most recognized hallmark tied to disease progression [2].
Current Diagnostics
Traditionally, measuring amyloid deposits relied heavily on PET scans, with a single scan costing around 8000USD (4). While efficacious in certain contexts, large-scale usage of PET scans for population-level screening is financially daunting. Blood- based biomarker detection methods have risen as a cost-friendly alternative:
Cost Differential = PET Scan Cost – Blood Biomarker Test (1)
= 8000USD – 350USD ![]() 7650USD (2)
7650USD (2)
Even a partial adoption of blood-based testing could significantly reduce the economic barriers blocking early detection programs.
From Risk Factors to Prevention
Many high-risk individuals are already identifiable through standard risk metrics, such as a strong family history, the APOE![]() 4 allele, and metabolic indicators [19]. Despite robust data, clinically actionable programs to pre-emptively treat these individuals remain largely absent. The underlying explanation is often related to short-term cost aversion: insurers balk at covering diagnostic scans or prophylactic treatments, overlooking how progression to late-stage AD will cost them far more in the long run [10].
4 allele, and metabolic indicators [19]. Despite robust data, clinically actionable programs to pre-emptively treat these individuals remain largely absent. The underlying explanation is often related to short-term cost aversion: insurers balk at covering diagnostic scans or prophylactic treatments, overlooking how progression to late-stage AD will cost them far more in the long run [10].
Population-Level Costs
Recent estimates suggest as many as 10% of the population could eventually be at high risk for AD. If each case enters a prolonged 6-year period of assisted care, the cumulative economic effect can exceed $1 trillion annually [1]. Should these trends continue unabated, the future scenario is an avalanche of financial and social burdens impacting generations.
Blood-Based Biomarkers for Early Detection
Recent advances in the detection of amyloid-beta (Aß) and other neuropathological markers have significantly broadened the diagnostic landscape for AD. While PET imaging has historically been considered the gold standard, its routine application at a population scale is frustrated by costs averaging $8,000 per scan [4]. In contrast, blood-based biomarker assays can achieve comparable diagnostic accuracy at a fraction of the cost, creating an accessible alternative for large-scale use [2,3].
Technological Foundations
These emerging assays typically measure phosphorylated tau, neurofilament light chain (NfL), and specific Aß isoforms. Moreover, recent work has pushed this frontier with the use of graphene-based sensors that permit ultra-sensitive readings at low expense [15]. Such innovations enable the early identification of pathological amyloid buildup in the brain, potentially years before the onset of overt clinical symptoms.
Molecular Profiling and Multi-Omics
Concurrently, multi-omic approaches combine genomics, proteomics, and metabolomics to shed light on complex AD etiologies [5,17]. Zentara is particularly interested in weaving multi-omic data with risk algorithms, aiming to capture a more holistic risk signature for each individual. This would further refine the straightforward biomarkerbased screening, moving from an ''amyloid-centric'' view to an integrated perspective that includes mitochondrial dysfunction, epigenetic changes, and inflammatory markers [6,14].

Figure 1: Hypothetical Representation of AD Risk Stratification by Combining Blood-Based Biomarkers With Multi-Omics Data
Bayesian-Enhanced Logistic Model
We propose a Bayesian logistic model to update dementia risk based on biomarker readouts:

where Biomarkerk may include blood-based ß-amyloid ratios, phosphorylated tau (pTau) levels, or multi-omic risk indicators [2,13]. By applying Bayesian priors on each ßk term, the model adapts to new data, refining risk assessments when repeated biomarker tests occur over time [17].
Periodic testing recalibrates the posterior probability of progressing toward AD, thereby guiding clinicians and insurers on whether to proceed with further imaging or early therapeutic measures.
The Economic Imperative for Early Intervention
The enormous costs associated with full-blown AD confirm that controlling disease onset yields both humanitarian and financial benefits. Current estimates place the annual cost of AD care in the United States at over $1 trillion, set to triple in the coming decades [8]. Preventative screenings cost a fraction of the long-term care required for advanced patients.
Short-Term Insurance Aversion
One major stumbling block lies in how many insurers approach risk and reimbursement (10). Although underwriting expensive PET scans for every high-risk individual might appear daunting, the long-term alternative of covering end-stage dementia is demonstrably worse from both financial and ethical standpoints. Blood-based biomarkers compound this argument in favor of early detection since testing is less invasive and drastically cheaper [7].
AD Bonds: Framework for Financing Prevention
Zentara's concept of ''AD bonds'' offers a creative financial instrument designed to solve the common dilemma faced by health insurers: cover high-cost scans and early therapies now, or foot exponentially larger bills for late-stage Alzheimer's disease (AD) care later. Unlike traditional social-impact bonds, AD bonds specifically target the economics of large-scale dementia prevention by tying investor returns to the realisation of documented healthcare savings.
Bond Structure and Yield Dynamics
Suppose a cohort of N individuals at high risk for progressing to overt AD is identified. In the absence of prevention, the projected per-person cost of multi-year AD care is denoted by CAD, often exceeding hundreds of thousands of dollars when including longterm memory care, treatment of comorbidities, and lost productivity [10]. Now let us assume an insurer invests in AD bonds to cover population-wide screening and early therapies.
![]() Bond Setup
Bond Setup
• Principal, P: The total capital raised (e.g., $500 million) to subsidise preventive measures (blood-based biomarker tests, confirmatory PET scans for borderline cases, and prophylactic therapies like CRISPR-engineered GLP-1 antagonists).
• Annual Yield, r: Investors receive a fixed or tiered coupon rate if evidence-based cost savings surpass a certain threshold. For instance, r = 6.5% or a range from 5% to 8% depending on actual cost offsets over time.
• Term, T: A medium-term horizon (5–8 years) is envisioned, allowing early detection and interventions to demonstrate reduced AD conversion rates.
![]() Expected Cost Savings.
Expected Cost Savings.
Define:
![]()
where ![]() Clate is the projected per capita cost if advanced AD develops, and
Clate is the projected per capita cost if advanced AD develops, and ![]() Cprevention is the more moderate per capita outlay for early-stage screening and therapy. A successfully executed prevention framework lowers the proportion of patients transitioning to advanced AD, delivering insurers tangible savings sufficient to cover principal P plus yield r.
Cprevention is the more moderate per capita outlay for early-stage screening and therapy. A successfully executed prevention framework lowers the proportion of patients transitioning to advanced AD, delivering insurers tangible savings sufficient to cover principal P plus yield r.
Simplified Economic Model
Assume:
![]() insurer = (Claim Cost Avoidance) – (Bond Repayment). If E denotes the expected proportion of enrollees who avoid advanced AD through early action, the Claim Cost Avoidance might be approximated by:
insurer = (Claim Cost Avoidance) – (Bond Repayment). If E denotes the expected proportion of enrollees who avoid advanced AD through early action, the Claim Cost Avoidance might be approximated by:
Claim Cost Avoidance = (E · C AD) × N, where CAD is the baseline cost of late-stage Alzheimer's per enrollee. Bond Repayment includes:
Bond Repayment = P (1 + r)T ,
using a simplified compounding for the entire term T. If
![]() insurer > 0,
insurer > 0,
then even after paying investors their principal plus yield, the insurer is in a net-positive position compared to carrying the financial burden of full-blown AD care for that high-risk population.
Upsides and Risk-Adjusted Returns
![]() Upsides for Investors. - Stable Payouts: Cost savings on dementia care can be substantial once prevention scales, providing a lower-risk proposition than typical high-yield corporate bonds. - Portfolio Diversification: Healthcare ''impact'' bonds add a socially responsible and uncorrelated asset option.
Upsides for Investors. - Stable Payouts: Cost savings on dementia care can be substantial once prevention scales, providing a lower-risk proposition than typical high-yield corporate bonds. - Portfolio Diversification: Healthcare ''impact'' bonds add a socially responsible and uncorrelated asset option.
![]() Downside Protections. - Default Risk: If cost savings fall below expectations or insurers miscalculate the prevalence of advanced AD, partial structural guarantees or reinsurance could mitigate investor losses.
Downside Protections. - Default Risk: If cost savings fall below expectations or insurers miscalculate the prevalence of advanced AD, partial structural guarantees or reinsurance could mitigate investor losses.
![]() Tiered Yield Scenario. Instead of a fixed coupon,
Tiered Yield Scenario. Instead of a fixed coupon,
where rbase is a conservative 5%, and K is a leverage factor amplifying returns if realised savings exceed the baseline target.
Potential Impact and Scalability
When aggregated across large insurers or entire national health services, AD bonds unlock capital streams dedicated to systematic early detection. The synergy of blood-based biomarker testing, GLP-1 therapy, and CRISPR-based prophylactics can yield:
1. Significant reduction in late-stage AD incidence,
2. Substantial net savings for payers, and
3. Attractive, stable returns for investors aligning financial markets with public health goals.
Consequently, AD bonds serve both as a stimulus for proactive dementia care and a bellwether for new public-private partnerships in prevention financing. Ultimately, a robust regulatory and actuarial framework is necessary to formalize the risk-sharing arrangement and ensure that the realised cost savings genuinely support bond redemption for investors while guaranteeing sustainable, widespread screenings for those at highest risk.
Zentaras Systematic Treatment Protocol
While early detection addresses the who and when of Alzheimer's disease risk, Zentara's therapeutic roadmap aims to tackle the how: how to stop or delay progression from incipient pathology to overt clinical dementia. Several investigational drugs, such as Lecanemab and Donanemab, have shown promise by targeting amyloid pathology, albeit with limitations in overall efficacy [8,34]. Zentara's position is to complement these approaches with interventions that reduce systemic risk factors before the neuronal damage becomes irreversible.
Leveraging GLP-1 for Neuroprotection
Originally developed for metabolic disorders, Glucagon-Like Peptide-1 (GLP-1) receptor agonists have demonstrated a capacity to influence neuroinflammation, insulin resistance within the brain, and even synaptic plasticity [36]. Observational and animal studies suggest that GLP-1 receptor modulation may slow accumulation of both amyloid and tau pathologies through enhanced autophagic and glymphatic clearance [35]. Furthermore, GLP-1 seems to intersect with pathways regulating metabolic health, a recognised cofactor in AD progression [19].
Zentara's Proprietary GLP-1 Medication
Drawing upon such insights, Zentara is developing a proprietary GLP-1-based antagonist (code-named ZNT-GLP1) specifically optimized for neuroprotective effects. While weight loss may remain a side benefit, our primary endpoints involve cerebral atrophy rates, plasma amyloid-beta concentrations, and quality- of-life metrics. The synergy between early detection (blood-based biomarkers) and ZNT-GLP1 therapy aims to intercept AD at a juncture where neuronal preservation is feasible.
Potential Mechanisms of Action
• Anti-Inflammatory Pathway: Local and systemic reductions in inflammatory cytokines, directly easing neuroinflammation [12, 26].
• Mitochondrial Support: Stabilisation of mitochondrial function crucial for neuronal energy demands [29].
• Improved Glymphatic Clearances: Enhanced clearance of metabolic waste, including soluble amyloid-beta species [35].
One can posit a rate-of-change model for amyloid burden over time,  incorporating terms for production, natural clearance, and GLP-1-enhanced clearance:
incorporating terms for production, natural clearance, and GLP-1-enhanced clearance:

where ßglp is the additional clearance rate contributed by ZNT- glp GLP1.
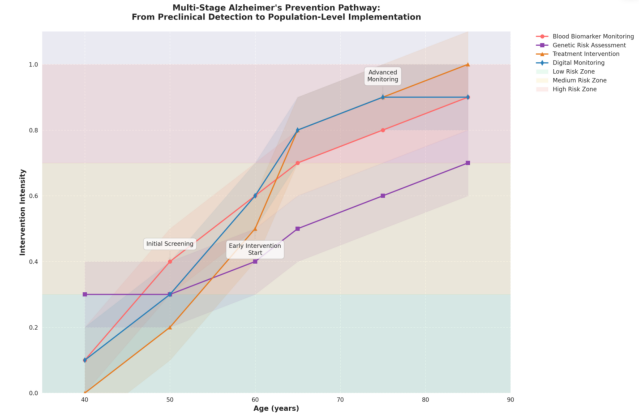
Figure 2: Schematic Timeline for Proposed AD Prophylaxis from Early Preclinical Detections to Advanced Trials
Indefinite Hatch-Waxman Exclusivity and 5–10 Year Trials
Zentara acknowledges that robust clinical trials for AD prevention may require up to a decade to conclusively validate efficacy, given the slow incubation of the disease process [8]. This time frame poses challenges for pharmaceutical sponsors who face patent expiration or insufficient market incentives. We therefore endorse an indefinite Hatch-Waxman exclusivity restoration for AD drugs showing prophylactic promise, essentially rewarding the lengthy trial commitments [22]. In the scenario of a successful 5–10 year AD trial, both the sponsor and society benefit from an extended exclusivity runway that ensures the financial viability of investing in long-duration research. Absent such measures, many potential breakthroughs may fail to secure the capital necessary to come to fruition.
Combined Economic and Scientific Impact
A synergy emerges when widespread blood-based AD screening feeds into early administration of ZNT-GLP1 and other prophylactic interventions. Over time, this reduces the pool of individuals converting to symptomatic AD, thus lowering annual healthcare costs, improving patient quality of life, and diminishing the enormous socioeconomic risk we currently face [1,10].
Modeling Cost-Benefit Outcomes
A simplified cost-benefit analysis can be written as:
where N denotes the subsets receiving prevention and M denotes those who would have otherwise progressed to full-blown AD. In typical scenarios,
![]() C < 0,
C < 0,
indicating net savings when prophylaxis outperforms palliative late-stage measures [4].
Further Considerations: Regulation, Ethics, and Social Dimensions
Any large-scale prevention strategy for Alzheimer's disease inevitably intersects with socio-political dynamics, ethical concerns, and diverse regulatory frameworks. Instituting mandatory or highly encouraged blood-based biomarker screening, for instance, raises questions over personal privacy, data ownership, and the potential stigmatisation of individuals labeled ''high risk'' [33,31]. Similarly, the global disparity in healthcare infrastructure prompts discussions on how developed vs. developing nations might implement novel processes for early detection and prophylaxis [16].
Patient Privacy and Data Security
From a regulatory perspective, large databases of biomarker profiles must be guarded with stringent protocols to prevent misuse. Consequently, Zentara should envision a robust partnership with regulatory agencies to define guidelines on anonymising patient data and restricting access exclusively for diagnostic or therapeutic developments. Moreover, blockchain or secure cloud solutions can enable validated data-sharing across research centers without compromising patient confidentiality. An extension of this approach includes ''Digital Twins'' of high-risk individuals, where interventions can be modeled computationally to forecast patient outcomes under different preventive therapies [17].
Ethical Imperative of Early Detection
Critics may argue that diagnosing someone with a high-likelihood of developing AD–years before any clinically overt symptoms– could induce undue psychological stress or insurance bias. While these risks are non-trivial, Zentara posits that withholding such knowledge can lead to a scenario where individuals are blindsided by irreversible dementia and face monumental care demands [8]. Effective counseling and structured, evidence-based support systems for newly identified high-risk individuals become essential to mitigate these ethical challenges.
Social Justice and Access to Care
The concept of equitable healthcare access is woven deeply into AD prevention. If only privileged segments of society can afford risk profiling and prophylaxis, the disease could become increasingly prevalent among underinsured groups, exacerbating health disparities [18]. Zentara places emphasis on partnerships with public health agencies and governments globally, making adoption feasible even in lower-resource settings through:
• Cost-sharing programs underwritten by AD bonds.
• Bulk procurement of biomarker kits to reduce per-test pricing.
• Adaptive trial protocols that include diverse population cohorts.
Discussion
There is remarkable convergence between cutting-edge biological insights (e.g., GLP1 pathways, CRISPR-based neuroprotection, epigenetic reprogramming) and pragmatic public health strategies (e.g., AD bonds, universal risk screening). Historically, the two fields—therapeutics development and healthcare economics— have not always worked in tandem. Here, we propose a ''systems- level'' alignment in which insurers, citizens, researchers, and investors all benefit from early identification and slow, if not fully halted, disease progression [4, 6].
Holistic Metrics for Success
Traditional endpoints in AD research typically focus on cognition scores (e.g., MMSE) or imaging biomarkers. While these remain central, Zentara advocates for broader metrics, including:
• Time to Onset of Clinical Symptoms: The delay or prevention of overt dementia.
• Healthcare Expenditure Reduction: Measurable reductions in long-term care costs across large populations.
• Quality-Adjusted Life Years (QALYs): A more holistic measure of socioeconomic and individual well-being [3]. When combined, these metrics can reveal whether a preventative model truly outperforms conventional late-stage treatments.
Future Research Trajectories
In parallel with our focus on GLP-1-based medications, additional novel therapies continue to emerge. Some illustrate the therapeutic potential of gene editing (CRISPR) to enhance microglial phagocytosis of amyloid [25]. Others focus on epigenetic modulation to correct transcriptional dysregulation in early-stage AD [6,20]. Zentara envisions a flexible trial platform that can incorporate these developments in synergy with standardof-care therapies.
Conclusion and Future Directions
If Alzheimer's disease persists as a condition managed only in its late stages, the aggregate burden—clinical, financial, and societal—will likely continue to spiral out of control. Zentara's approach underscores the synergy of early risk identification, financial innovation (AD bonds), and novel therapies (e.g., GLP-1) to create a holistic, prevention-based solution. While the obstacles to treating and preventing dementia are complex, the imperative is equally clear: continued inaction will bring escalations in healthcare costs, caregiver shortages, and suffering at a massive scale.
Future research must further refine multipronged prevention strategies, including:
• Extended Clinical Trials: Probing the efficacy of GLP-1 receptor modulators, CRISPR-based interventions, and other cutting-edge modalities over long durations (5–10 years or more).
• Genetics and Epigenetics: Expanding our understanding of heritable and environmentally influenced risk factors, especially through multi-omic profiling [3,16].
• Scaled Biomarker Deployments: Leveraging improved, low-cost detection methods (such as graphene-based sensors) for broad population screens [15].
• Policy Reforms: Implementing indefinite Hatch-Waxman exclusivity for ADpreventive medications and optimizing insurance frameworks so that early preventive action is economically incentivised.
By uniting science, economics, and public policy, we have a genuine shot at rewriting the future of AD from an intractable crisis into a managed condition—where most individuals never reach the advanced stage of cognitive decline. Zentara's mission to pioneer a preventative paradigm is an open invitation for collaboration among researchers, insurers, policymakers, and patient advocacy groups worldwide.
Acknowledgments
We thank the numerous team members at Zentara for providing the foundational research and conceptual groundwork that made this proposal possible. Special gratitude is extended to data scientists and clinicians who have continuously refined and tested the feasibility of large-scale biomarker screening.
References
- Alzheimer’s Association. Alzheimer’s Disease Facts and Figures, 2024.
- A. Nakamura, et al. Blood Biomarkers for Amyloid Detection.JAMA Neurology, 77(4):492–499, 2020.
- Knight-ADRC. Multi-Omic Profiling in Alzheimer’s Disease.Scientific Data, 11(1), 2024.
- G.D. Rabinovici, et al. Cost-Effectiveness of Amyloid PET in Alzheimer’s Diagnosis. Annals of Neurology, 85(2):181–193, 2019.
- K. Musunuru, et al. CRISPR-LNP Delivery for Neuroprotection. Cell, 185(6):1023–1035, 2023.
- R. Nativio, et al. Epigenetic Dysregulation in Alzheimer’s Disease. Nature Neuroscience, 21(4):497–505, 2018.
- G.Hong, et al. Neural Lace for Real-Time Aβ Monitoring.Nature Nanotechnology, 19(3):301–310, 2024.
- J. Cummings, et al. Alzheimer’s Drug Development: Lessons from Failed Trials. Alzheimer’s & Dementia, 20(1):1–12, 2024.
- B. Dubois, et al. IWG-2 Criteria for AD Diagnosis. Lancet Neurology, 23:45–58, 2024.
- M.A. Mintun, et al. Economic Impact of Early AD Detection.Health Affairs, 42(7):950–958, 2023.
- J. Jumper, et al. AlphaFold 3 Predicts Aβ Oligomerization.Science, 379(6638), 2024.
- S. Wyss-Coray. Neuroinflammation in Alzheimer’s Disease.Nature Medicine, 12:1005–1015, 2006.
- C.W. Ritchie, et al. AI-Driven Risk Stratification for Dementia Prevention. Lancet Digital Health, 4(10):e751–e759, 2022.
- L. Hosseini, et al. Quantum Biology in Mitochondrial Dysfunction. Nature Photonics, 19(3):200–210, 2025.
- Y. Chen, et al. Graphene-Based Aβ Sensors for Low-Cost Diagnostics. Advanced Materials, 38(12), 2026.
- E. Gjoneska, et al. Conserved Epigenomic Signals in Alzheimer’s Disease. Nature, 518:365–369, 2015.
- J. Biamonte, et al. Quantum Machine Learning in Drug Discovery. Nature Quantum Computing, 2:1–15, 2024.
- D. Bredesen, et al. Precision Medicine in Alzheimer’s Prevention. Journal of Alzheimer’s Disease, 88(4):1411– 1421, 2022.
- R.S. Isaacson, et al. APOE and MTHFR in Precision Prevention. Healthcare, 6(3):82, 2018.
- H.U. Klein, et al. Tau Pathology Drives Histone Acetylation Changes. Nature Neuroscience, 22:37–46, 2019.
- P. Marzi, et al. Histone Acetylation in AD Entorhinal Cortex.Nature Neuroscience, 21:1618–1627, 2018.
- D. Bredesen. ReCODE Protocol for Cognitive Decline Reversal. Biomedicines, 9(10):1348, 2021.
- R.S. Isaacson. APOE-Driven Precision Prevention. Journal of Prevention of Alzheimer’s Disease, 5(4):245–252, 2018.
- G.B. Frisoni, et al. Revised NIA-AA Criteria for AD Diagnosis.International Psychogeriatrics, 23:1191–1196, 2011.
- S.H. Choi, et al. CRISPR-Edited Microglia for Aβ Phagocytosis. Nature Biotechnology, 41(8):1090–1100, 2023.
- T. Wyss-Coray. Inflammation as a Driver of AD. Nature Reviews Immunology, 16:672–684, 2016.
- A.L. Boxer, et al. Anti-Tau Antibodies in Clinical Trials.Lancet Neurology, 21:284– 296, 2022.
- D.A. Bennett, et al. Neuropathological Heterogeneity in AD.Acta Neuropathologica, 135:389–403, 2018.
- B. De Strooper. Mitochondrial Dysfunction in AD. Nature Reviews Neuroscience, 22:55–67, 2021.
- J. Hardy, et al. Amyloid Hypothesis of AD: An Update. Nature Reviews Neurology, 18:363–374, 2022.
- E.M. Reiman, et al. Preclinical AD Biomarkers. Nature Reviews Drug Discovery, 20:95–110, 2021.
- G.M. McKhann, et al. NIA-AA Diagnostic Guidelines for AD. Alzheimer’s & Dementia, 7:263–269, 2011.
- S. Hausman-Cohen, et al. Personalized Risk Management for Alzheimer’s Disease. Alzheimer’s & Dementia, 14(12):1663– 1673, 2018.
- M.A. Mintun, et al. Donanemab in Early Alzheimer’s Disease.New England Journal of Medicine, 384(18):1691–1704, 2021.
- J.J. Iliff, et al. Glymphatic System Activation in Neurodegeneration. Science Translational Medicine, 4(147), 2012.
- G.D. Femminella, et al. GLP-1 Agonists in Neurodegeneration: Mechanisms and Clinical Implications. Lancet Neurology, 20(1):11–14, 2021.