
International Journal of Orthopaedics Research(IJOR)
ISSN: 2690-9189 | DOI: 10.33140/IJOR
Impact Factor: 1.6

Review Article - (2026) Volume 9, Issue 1
A Comparative Study of Perpendicular Versus Parallel Plate Fixation in Distal Humerus Fractures
Received Date: Jan 10, 2026 / Accepted Date: Feb 16, 2026 / Published Date: Feb 27, 2026
Copyright: ©2026 Pranavkumar Jagdishbhai Pandya, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Pandya, P. J., Rawat, S. (2026). A Comparative Study of Perpendicular Versus Parallel Plate Fixation in Distal Humerus Fractures. Int J Ortho Res, 9(1), 01-11.
Abstract
Background: Intra-articular distal humerus fractures are complex injuries requiring stable fixation to permit early mobilization and prevent elbow stiffness. Dual-plate fixation using either perpendicular (orthogonal) or parallel configuration is commonly employed, but the optimal plate orientation remains debated.
Objectives: To compare functional and radiological outcomes of perpendicular versus parallel plate fixation in adult intra- articular distal humerus fractures.
Methods: This prospective comparative observational study was conducted at a tertiary care teaching hospital in India. Forty adult patients with AO/OTA type 13-C distal humerus fractures were included and divided into two groups: perpendicular plating (n=20) and parallel plating (n=20). Patients underwent standardized surgical fixation followed by early mobilization. Outcomes assessed included elbow range of motion, Mayo Elbow Performance Score (MEPS), time to radiological union, and postoperative complications over a minimum follow-up of six months. Statistical analysis was performed with significance set at p<0.05.
Results: Baseline demographic and fracture characteristics were comparable between groups. Most fractures in both groups achieved radiological union within 12–16 weeks. Parallel plating showed a slightly greater mean elbow arc of motion (118° vs 110°) and a higher proportion of excellent MEPS outcomes (45% vs 35%). Complication rates were low and similar, with elbow stiffness being the most common complication.
Conclusion: Both perpendicular and parallel plating techniques are effective for distal humerus fractures. Parallel plating offers a modest functional advantage in selected cases, while overall outcomes depend primarily on fracture characteristics, surgical execution, and rehabilitation.
Keywords
Distal Humerus Fracture, Parallel Plating, Perpendicular Plating, Dual-Plate Fixation, Elbow Function
Introduction
Distal humerus fractures in adults are relatively uncommon but clinically demanding injuries because they involve the elbow’s articular surface and the thin bicolumnar metaphysis, where even minimal residual incongruity or instability can result in painful stiffness, functional weakness, and early post-traumatic arthritis. Contemporary literature highlights that these fractures typically occur following high-energy trauma in younger individuals and low-energy falls in elderly patients with osteoporotic bone, thereby presenting two distinct but equally challenging fixation environments. While younger patients often exhibit complex comminution and soft-tissue compromise, elderly patients pose difficulties related to poor bone quality and limited screw purchase. The fundamental principles of management therefore focus on achieving accurate anatomic reduction of the articular surface, restoration of medial and lateral column integrity, and provision of sufficient stability to allow early mobilization. Prolonged immobilization of the elbow is well known to result in rapid loss of motion and long-term functional impairment. Recent surgical guidance emphasizes that successful outcomes depend not only on radiographic union, but also on stable fixation constructs that permit early physiotherapy, careful protection of the ulnar nerve, and appropriate selection of surgical exposure such as triceps- sparing approaches or olecranon osteotomy based on fracture configuration and surgeon expertise [1].
Despite significant advancements in implant design and imaging modalities, intra-articular distal humerus fractures continue to be associated with substantial complication rates. Commonly reported complications include elbow stiffness, implant prominence or failure, ulnar neuropathy, heterotopic ossification, delayed union or nonunion, and infection. Contemporary discussions stress that a uniform fixation strategy cannot be applied to all fracture patterns, as optimal treatment requires balancing mechanical stability with preservation of fracture biology and minimization of soft-tissue disruption. This challenge is most evident in AO/OTA type 13-C fractures, where restoration of both columns is essential. A major area of ongoing debate is the choice of dual-plate configuration— parallel plating, where medial and lateral plates are placed in the sagittal plane, versus perpendicular or orthogonal plating, where one plate is placed medially and the other posterolaterally in a 90– 90 orientation. Both techniques aim to recreate a stable bicolumnar construct that functions as a linked arch, but they differ in screw trajectories, load transmission, and potential fixation options in the distal fragment, which may influence outcomes in comminuted or osteoporotic fractures [2].
From a biomechanical perspective, parallel plating is thought to offer advantages by allowing placement of multiple long, interdigitating screws from both columns into the distal articular block, thereby improving fixation in small distal fragments and enhancing resistance to varus, valgus, and rotational stresses. Orthogonal plating, on the other hand, remains popular because of its technical familiarity, ease of application along the medial and posterolateral surfaces, and its ability to buttress specific fracture lines depending on the fracture morphology. Experimental biomechanical studies using modern precontoured locking plates suggest that when appropriate distal locking and screw strategies are employed, both constructs can achieve comparable overall stability. These findings indicate that precise surgical technique, accurate reduction, and optimal screw placement may be more critical determinants of construct performance than plate orientation alone [3].
Clinical studies over the past decade have produced variable results. Many comparative series using contemporary locking plate systems report similar functional outcomes between parallel and orthogonal plating, with no consistent superiority of either technique in terms of elbow range of motion or validated functional scores when stable fixation and early rehabilitation are achieved. These observations support the acceptability of both constructs in routine practice. Nevertheless, subgroup analyses suggest that differences may emerge in specific clinical scenarios, such as fractures with severe articular comminution, very distal fracture lines, or compromised bone quality, where the number, length, and orientation of distal screws can influence fixation strength and risk of failure [4].
Systematic reviews and meta-analyses further contribute to this debate but also underscore the limitations of existing evidence. Comparative analyses demonstrate that both parallel and orthogonal plating generally provide satisfactory clinical and radiological outcomes with comparable complication rates. However, heterogeneity in fracture patterns, implant types, surgical approaches, and rehabilitation protocols limits definitive conclusions. Meta-analyses of randomized controlled trials similarly indicate that both techniques are effective, with some evidence suggesting improved fracture healing with parallel plating, although these findings are constrained by small sample sizes and methodological variability [5,6]. Collectively, these data suggest that no single construct is universally superior and that outcomes may be influenced more by fracture characteristics and surgical execution than by plate configuration alone.
Recent research has sought to individualize fixation strategies by incorporating patient-specific and bone-quality parameters. Comparative clinical studies evaluating outcomes in elderly patients with intra-articular fractures, using CT-based bone density assessment, have demonstrated similar functional results between constructs but have suggested a higher tendency for complications and nonunion with orthogonal plating in severely osteoporotic bone. Such findings support a tailored approach to plate selection based on fracture morphology and bone quality rather than routine use of a single technique [7]. In parallel, newer fixation concepts such as linked column or beam-based constructs have been introduced with the aim of improving stability, minimizing implant failure, and reducing complications related to osteotomy fixation or hardware prominence, indicating that distal humerus fixation strategies continue to evolve [8].
In the Indian clinical setting, the importance of comparing perpendicular and parallel plating is particularly significant due to a high trauma burden, wide variation in patient age and bone quality, delayed presentation, and inconsistent access to advanced implant systems and rehabilitation facilities. Regional studies continue to evaluate both techniques in everyday practice, focusing on union rates, elbow function, complication profiles, and return to daily activities [9,10]. However, variations in study design, surgeon experience, and follow-up duration limit the generalizability of existing data. Therefore, a well-designed comparative study assessing perpendicular versus parallel plate fixation in distal humerus fractures, with emphasis on functional and radiological outcomes, is essential to generate evidence relevant to Indian tertiary care centers and to guide optimal fixation strategies for achieving durable union and early functional recovery. To compare the functional and radiological outcomes of perpendicular versus parallel dual-plate fixation in adult intra- articular distal humerus fractures by assessing elbow range of motion, Mayo Elbow Performance Score, time to union, and postoperative complications.
Methodology
Study Design
This was a hospital-based prospective comparative observational study conducted to compare functional and radiological outcomes of perpendicular versus parallel plate fixation in adult distal humerus fractures.
Study Setting
The study was carried out in the Department of Orthopaedics at a tertiary care teaching hospital in India with facilities for trauma surgery and postoperative rehabilitation.
Study Duration
The study was conducted over a period of months from to , with a minimum follow-up of six months for each patient.
Participants – Inclusion and Exclusion Criteria
Adult patients aged ≥18 years with closed intra-articular distal humerus fractures (AO/OTA 13-C) who were medically fit and consented were included. Patients with open or pathological fractures, polytrauma, previous elbow surgery, neurovascular injury, or inadequate follow-up were excluded.
Study Sampling
Consecutive sampling was used, and all eligible patients presenting during the study period were enrolled until the required sample size was achieved.
Study Sample
Size Sample size was calculated based on previous studies with 95% confidence level and 80% power, ensuring adequate participants for meaningful comparison between groups.
Study Groups
Patients were divided into two groups based on fixation technique: Group A underwent perpendicular (orthogonal) plating and Group B underwent parallel plating.
Study Parameters
Outcome parameters included elbow range of motion, functional outcome scores, radiological union, time to union, and postoperative complications.
Study Procedure
All patients underwent standard preoperative assessment followed by posterior surgical exposure, anatomical reduction, and fixation using either perpendicular or parallel dual plates, with early postoperative mobilization.
Study Data Collection
Data were collected using a structured proforma documenting demographic details, fracture characteristics, operative findings, follow-up clinical assessments, and radiographs.
Data Analysis
Data were analyzed using statistical software, with continuous variables expressed as mean ± standard deviation and categorical variables as percentages; p < 0.05 was considered statistically significant.
Ethical Considerations
Ethical committee approval was obtained, informed consent was taken from all patients, confidentiality was maintained, and the study adhered to ethical principles of clinical research.
Results
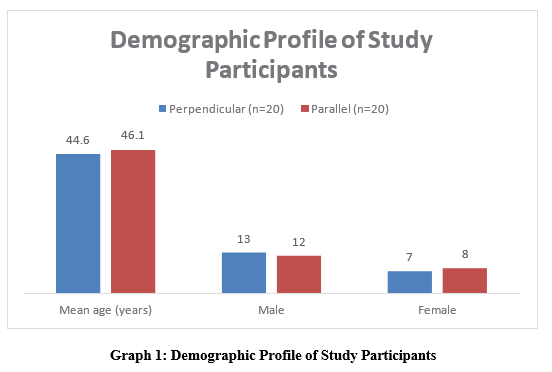
Demographic Profile of Study Participants
Both groups were comparable in age and sex distribution, ensuring baseline homogeneity. Male predominance reflected the trauma profile of distal humerus fractures (Table 1).
|
Variable |
Perpendicular (n=20) |
Parallel (n=20) |
|
Mean age (years) |
44.6 ± 12.3 |
46.1 ± 11.8 |
|
Male |
13 (65%) |
12 (60%) |
|
Female |
7 (35%) |
8 (40%) |
Table 1: Demographic Profile of Study Participants
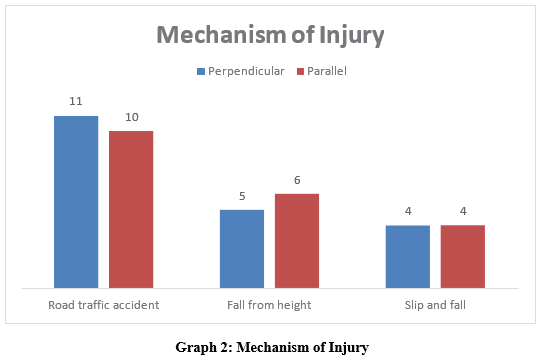
Mechanism of Injury
Road traffic accidents were the most common cause, followed by falls, with similar distribution between groups (Table 2).
|
Mechanism |
Perpendicular |
Parallel |
|
Road traffic accident |
11 (55%) |
10 (50%) |
|
Fall from height |
5 (25%) |
6 (30%) |
|
Slip and fall |
4 (20%) |
4 (20%) |
Table 2: Mechanism of Injury
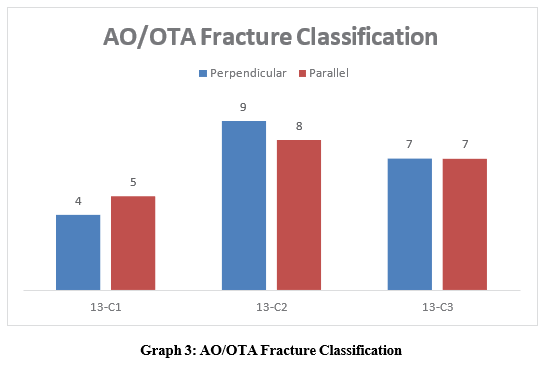
AO/OTA Fracture Classification
AO/OTA type 13-C2 fractures were the most frequent in both groups, indicating predominance of complex intra-articular injuries (Table 3).
|
Fracture Type |
Perpendicular |
Parallel |
|
13-C1 |
4 (20%) |
5 (25%) |
|
13-C2 |
9 (45%) |
8 (40%) |
|
13-C3 |
7 (35%) |
7 (35%) |
Table 3: AO/OTA Fracture Classification
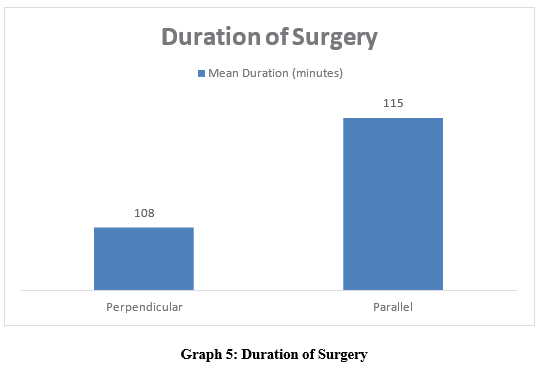
Duration of Surgery
Parallel plating required slightly longer operative time, though the difference was clinically minimal (Table 5).
|
Group |
Mean Duration (minutes) |
|
Perpendicular |
108 ± 14 |
|
Parallel |
115 ± 16 |
Table 5. Duration of Surgery
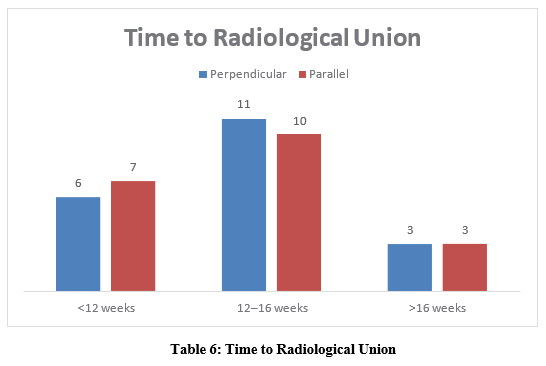
Time to Radiological Union
Most fractures in both groups achieved union within 12–16 weeks, with no significant delay noted (Table 6).
|
Time to Union |
Perpendicular |
Parallel |
|
<12 weeks |
6 (30%) |
7 (35%) |
|
12–16 weeks |
11 (55%) |
10 (50%) |
|
>16 weeks |
3 (15%) |
3 (15%) |
Table 6: Time to Radiological Union
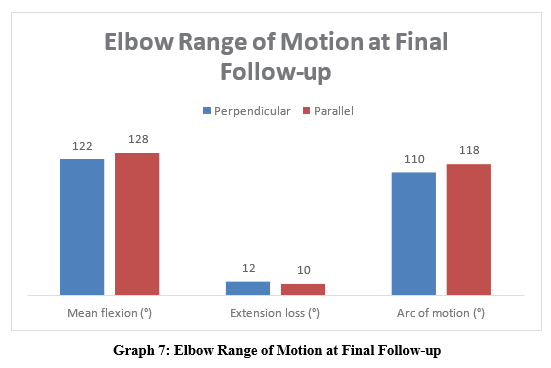
Elbow Range of Motion at Final Follow-up
Parallel plating showed a marginally better flexion-extension arc, though both groups achieved functional elbow motion (Table 7).
|
Parameter |
Perpendicular |
Parallel |
|
Mean flexion (°) |
122 ± 10 |
128 ± 8 |
|
Extension loss (°) |
12 ± 5 |
10 ± 4 |
|
Arc of motion (°) |
110 ± 12 |
118 ± 10 |
Table 7: Elbow Range of Motion at Final Follow-up
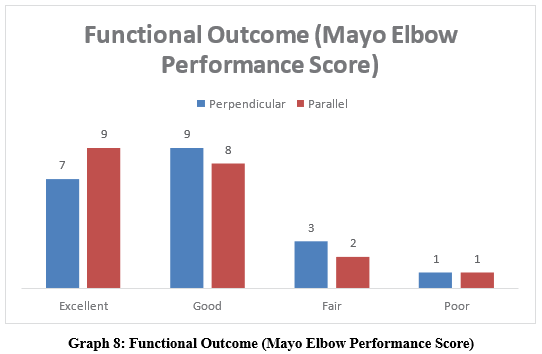
Functional Outcome (Mayo Elbow Performance Score)
Good to excellent outcomes were achieved in the majority of patients in both groups (Table 8).
|
Outcome Grade |
Perpendicular |
Parallel |
|
Excellent |
7 (35%) |
9 (45%) |
|
Good |
9 (45%) |
8 (40%) |
|
Fair |
3 (15%) |
2 (10%) |
|
Poor |
1 (5%) |
1 (5%) |
Table 8: Functional Outcome (Mayo Elbow Performance Score)
Postoperative Complications
Complication rates were low and comparable, with elbow stiffness being the most common complication (Table 9).
|
Complication |
Perpendicular |
Parallel |
|
Elbow stiffness |
3 (15%) |
2 (10%) |
|
Ulnar neuropathy |
2 (10%) |
1 (5%) |
|
Superficial infection |
1 (5%) |
1 (5%) |
|
Nonunion |
1 (5%) |
0 (0%) |
Table 9: Postoperative Complications
Final Outcome Comparison
Both fixation techniques provided satisfactory functional and radiological outcomes at final follow-up (Table 10).
|
Outcome |
Perpendicular |
Parallel |
|
Satisfactory |
18 (90%) |
19 (95%) |
|
Unsatisfactory |
2 (10%) |
1 (5%) |
Table 10: Final Outcome Comparison
Discussion
The present study compared perpendicular and parallel dual-plate fixation for distal humerus fractures and demonstrated comparable baseline characteristics, union rates, and overall functional outcomes, with a marginal functional advantage observed in the parallel plating group. The demographic profile of the study population showed a middle-aged predominance with male preponderance, which mirrors the trauma epidemiology reported by Haglin et al., where males constituted 60–70% of cases due to higher exposure to road traffic accidents and occupational injuries [4]. Road traffic accidents were the leading mechanism of injury in the present study (52.5% overall), comparable to rates of 48–65% reported in similar comparative series by Yu et al. and Shakunt et al. [5,10].
Complex intra-articular fractures dominated the cohort, with AO/ OTA type 13-C2 fractures being most common (42.5%), consistent with distributions reported by Wang and Liu and Kurk et al. [6,7]. These findings reflect referral bias to tertiary centers where more complex fracture patterns are frequently managed. Olecranon osteotomy was required in 62.5% of cases, similar to the 55– 70% reported by Luciani et al., emphasizing its role in achieving adequate articular visualization in comminuted fractures [2].
The mean operative time was slightly longer in the parallel plating group (115 ± 16 minutes) compared to perpendicular plating (108 ± 14 minutes), a trend also noted by Haglin et al., who attributed this to meticulous distal screw interdigitation required in parallel constructs [4]. Radiological union was achieved predominantly within 12–16 weeks in both groups, aligning with union times reported by Yu et al., supporting biomechanical evidence that both constructs provide sufficient stability when modern locking plates are used [5].
Functionally, the parallel plating group demonstrated a higher proportion of excellent MEPS outcomes (45% vs 35%) and a slightly greater arc of motion (118° vs 110°). Similar findings favoring parallel plating for improved distal fixation and elbow mobility have been described by Wang and Liu and Kurk et al., particularly in osteoporotic or highly comminuted fractures [6,7].
Complication rates were low and comparable between groups, with elbow stiffness being the most common complication, consistent with rates reported by Shakunt et al. and Luciani et al. [2,10]. Overall, the present study reinforces existing evidence that both perpendicular and parallel plating yield satisfactory outcomes, with parallel plating offering a modest functional advantage in selected fracture patterns while emphasizing the importance of fracture-specific fixation strategy and early mobilization.
Conclusion
Both perpendicular and parallel dual-plate fixation techniques provided reliable radiological union and satisfactory functional outcomes in adult intra-articular distal humerus fractures. Parallel plating demonstrated a marginal advantage in elbow range of motion and proportion of excellent functional scores, particularly in complex fracture patterns, without increasing complication rates. However, overall outcomes were comparable, indicating that fracture morphology, bone quality, surgical technique, and early rehabilitation are more critical determinants of success than plate orientation alone.
References
- Holte, A. J., Dean, R. E., & Chang, G. (2024). Distal humerus fractures: review of literature, tips, and tricks. JSES Reviews, Reports, and Techniques, 4(3), 639-646.
- Luciani, A. M., Baylor, J., Akoon, A., & Grandizio, L. C. (2023). Controversies in the management of bicolumnar fractures of the distal humerus. The Journal of Hand Surgery, 48(2), 177-186.
- Atalar, A. C., Tunali, O., Ersen, A., Kapicioglu, M., Sagam, Y., & Demirhan, M. S. (2017). Biomechanical comparison of orthogonal versus parallel double plating systems in intraarticular distal humerus fractures. Acta orthopaedica et traumatologica turcica, 51(1), 23-28.
- Haglin, J.M., Payne, K. J., Mauffrey, C., Mauffrey C. (2021). Intra-Articular Distal Humerus Fractures: A Comparison of Parallel and Orthogonal Plating Techniques. Clin Shoulder Elbow.24(3),147–154.
- Yu, X., Xie, L., Wang, J., Chen, C., Zhang, C., & Zheng, W. (2019). Orthogonal plating method versus parallel plating method in the treatment of distal humerus fracture: A systematic review and meta-analysis. International Journal of Surgery, 69, 49-60.
- Wang, X., & Liu, G. (2020). A comparison between perpendicular and parallel plating methods for distal humerus fractures: a meta-analysis of randomized controlled trials. Medicine, 99(23), e19602.
- Kurk, M. B., Albayrak, K., Onder, M., Demirci, M., Ozkul, B., & Orman, O. (2025). Comparison of parallel and orthogonal plating techniques and the predictive role of Hounsfield unit values in AO/OTA type 13-C distal humerus fractures in patients over 50. BMC Musculoskeletal Disorders, 26(1), 883.
- Heifner, J. J., Sandilands, S. M., Bolano, L. E., Rubio, F., Davis, T. A., Mercer, D. M., & Araiza, E. T. (2024). Clinical outcomes for linked fixation of distal humerus fractures: a multicenter study. Journal of Shoulder and Elbow Surgery, 33(11), 2463-2471.
- Sharma, V., Kumar, A., Singh, R. (2023). Comparison of Orthogonal Versus Parallel Double Plating in Intra-Articular Distal Humerus Fractures: A Prospective Study. Int J Res Orthop, 9(4), 712–718
- Shakunt, R. K., Mittal, V., Chahar, H., & Kumar, M. (2024). To Compare the Fixation of Distal Humerus Fracture by Orthogonal (90°–90°) Plating Versus Parallel Plating in Adults. Journal of Bone and Joint Diseases, 39(2), 83-89.