
Journal of Educational & Psychological Research(JEPR)
ISSN: 2690-0726 | DOI: 10.33140/JEPR
Impact Factor: 1.4

Research Article - (2025) Volume 7, Issue 3
A Comparative Study of Negative Effects of Syria's Earthquake in Aleppo City, 2023
2Faculty of Dentistry, Al-Sham Private University, Damascus, Syria
Received Date: Sep 01, 2025 / Accepted Date: Oct 08, 2025 / Published Date: Oct 21, 2025
Copyright: ©2025 Noura Zidan, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Zidan, D., Najaty, G., Zidan, N. (2025). A Comparative Study of Negative Effects of Syria's Earthquake in Aleppo City, 2023. J Edu Psyc Res, 7(3), 01-08.
Abstract
Earthquakes are unexpected and destructive disasters that can cause massive destruction and huge losses, and survivors may suffer severe psychological symptoms. With this serious lack of studies in the psychological field after the natural disaster that happened in Aleppo city, Syria. So, there must be a concentrated study that focus on affected people and their feeling after treating them with anti-depressants. Two questionnaires were distributed among 40 individuals that agreed on participating in this study, and questions focused on the effect of anti-depressants API and Placebo medicines in minimizing Post-traumatic stress disorder (PTSD) symptoms. The results showed that people who were given placebo have showed less percentages of fear after three months from the first questionnaire. Benefits from taking anti-depressants can be maintained with continued treatment, that is why placebo succeeded more than anti-depressants in this study.
Keywords
Placebo, Anti-depressants, API, PTSD, Earthquake
Introduction
One kind of natural disaster that causes a large loss of life and prop- erty is an earthquake. A total of over 60,000 persons were reported dead in Turkey and Syria as a result of earthquakes in March 2023 [1]. Both the mental health of the victims and those around them can be permanently impacted by traumatic experiences. Post-trau- matic stress disorder (PTSD) is one of the main anxiety illnesses brought on by the catastrophe. People may experience a crippling mental illness if they are subjected to a traumatic incident, such the recent coronavirus 2019 (COVID-19) or the earthquakes in Turkey and Syria in 2023.
Studying the impact of Meaning of Life (ML) following cata- strophic occurrences, like the recent earthquakes in Turkey and Syria in 2023, can offer insights into the psychological processes that promote resilience and recovery among university students by concentrating on the importance of social support and ML.
Social support (SS), which refers to the resources supplied by others that can be used to cope with stressors, has been demonstrated to be protective against mental health concerns [2].
SS may offer people material, emotional, and informational re- sources to help them deal with stressors and may have a signifi- cant role in preventing the onset of PTSD. The SS scale provides insights into the role of social and family networks in fostering re- silience and coping mechanisms, making it a valuable instrument for examining the significance of these networks during times of crisis [3].
The consequences of earthquakes on people's psychological well-being have drawn more attention in recent decades. Research on the aftermath of disasters suggests that a large number of victims may have a clinically significant symptomatic reaction as a result of being exposed to stressful events, the degree of loss, social dis- array, and a lack of support from the community. Many studies on mental health issues associated to earthquakes have recently been published in Asian nations, gradually introducing PTSD and its diagnostic criteria. Still, there are important questions about post- disaster psychopathology that need to be answered. These include things like the frequency with which the survivors of disasters meet the full diagnostic criteria for mental disorders, the kinds of disorders that are frequently associated with the disaster's effects, the duration and transience of the postdisaster psychopathology, and the extent to which the psychological reactions following a di- saster are universal or dependent on social, cultural, and economic factors [4].
To the best of our knowledge, no prior research has examined the prevalence of PTSD symptoms or the perceived severity of social stress among Syrians in the wake of the 2023 earthquakes in Turkey and Syria. In light of this, this study aims to add to the body of literature by investigating the prevalence of PTSD symptoms and perceived social support (SS) among Aleppo residents following the 2023 earthquake that struck Turkey and Syria [3].
Post-Traumatic Stress Disorders (PTSD)
Over the last four decades, a variety of psychopathologies have been linked to disasters; however, prior systematic reviews have shown that, of all the psychopathologies associated with disasters, posttraumatic stress disorder (PTSD) is the most extensively re- searched and likely the most common [5-7]. PTSD is more likely to manifest themselves following a significant disaster [8-10]. A number of conclusions have been drawn from earlier research on the psychological effects of natural disasters, including the prev- alence of PTSD, which can range from 2% to 67% [11]. Though few research have looked at the course of PTSD after natural di- sasters, the prevalence of PTSD reported in studies following nat- ural disasters is often lower than that reported in studies following technical or human-caused disasters [5,6,9,10]. A number of stud- ies have also reported an increase in the prevalence of PTSD over time. Longitudinal studies of natural catastrophes have shown a decline in the disorder's prevalence with time [12-16].
Numerous research' findings demonstrate that PTSD symptoms are prevalent in earthquake survivors, with confirmed rates of PTSD in these survivors ranging from 10% to 87%. [5,17-25]. The chance of developing PTSD is consistently linked to a larger degree of exposure to a disaster [6,9-11]. After six weeks to ten months, the prevalence rates of PTSD among Chi-Chi earthquake victims range from 7.9% to 21.7% [25-28]. According to earlier research, survivors of the 1999 earthquake in Turkey had PTSD rates ranging from 39% to 63%, and short-term therapy treatments are suggested [23,28-30]. Following an earthquake, children and adolescents have been shown to have PTSD at rates ranging from 21% to 70% [31-33]. Female sex, lesser education, and a lack of social support are common risk factors for post-earthquake PTSD [5,11,20,31,32,34-37]. The greatest predictor of PTSD is thought to be the survivors' level of dread during the earthquake [23,30,32,33]. People who feel high levels of fear during earth- quakes can get PTSD even from relatively small ones [37]. Fur- thermore, new research indicates that being a member of an ethnic minority has a strong correlation with PTSD [38-42].
In 1980, post-traumatic stress disorder received official classifica- tion as a psychiatric disorder.
Anxiety disorders: Post-traumatic stress disorder is one type of anxiety disorder that typically develops when a person experiences severe injury that poses a risk to their life, their physical well- being, or the safety of another individual [43].
All age groups are affected by the condition, however different age groups respond differently. Psychological anguish: Post-traumatic stress disorder brought on by explosions and conflicts is probably here to stay. Threats, diseases, traffic accidents, violent personal attacks, natural disasters, and torture. potentially fatal.
Following the period of psychological trauma, a number of illness- es develop that persist to a significant degree and impede every definition of the term "daily practice" and its variations center on the experience of a terrible incident that affected There were two main factors that contributed to the development of post-traumatic stress disorder in addition to wars [43]. Disasters in the 1950s and 1960s post-traumatic stress disorder research Natural violence, rape, and child abuse instances [43].
Placebo Treatment
It is difficult to define "placebo" in a way that makes sense inside. In contrast to "real" treatment, a placebo is typically understood to be inert and generic. However, it is evident that placebos work; they have an impact and are useful. Regarding non specificity, its meaning in relation to placebo is not totally apparent, but it most likely means, among other things, an illdefined or imprecise mode of action or an influence on multiple conditions. By definition, pla- cebos are just as particular as a lot of undeniably effective thera- pies. The term "placebo" has a specific, albeit restrictive, definition in placebo-controlled medication efficacy studies, which provide the majority of the evidence on placebo response in depression. A placebo is a pharmacologically inert capsule or injection. The improvement that takes place in the group that receives a placebo is known as the placebo effect or response. The placebo reaction is merely an irritation factor that needs to be deducted from the drug response in order to ascertain the genuine drug impact; it is not necessary to pinpoint the elements of the therapy that caused it in a drug efficacy trial. However, in double-blind clinical exper- iments, participants receiving a placebo receive far more than just an inert pill. The common therapy elements seen in all conceivable treatment scenario are directed toward them. These include the de- sire for and expectation of progress as well as the zeal, diligence, and dedication of clinicians. Antidepressant clinical trial partici- pants also receive attention, positive regard, encouragement, mo- bilization of hope, and the chance to articulate their distress, to varied degrees depending on the therapy context and physician. And these are typically sent to them once a week. It is reason- able to presume that some "placebo responders" are remitters who would have improved on their own just by the passage of time. Is there any benefit to using a placebo over a "wait and see" strategy, other than the passage of time? As far as I know, no research has explicitly tested the efficacy of placebo pills versus time alone in treating depression. However, three different lines of evidence— none of which is conclusive or devoid of bias— converge to imply that receiving a placebo relieves symptoms more than receiving no treatment at all [44].
Zoloft Sertraline
In several nations, SSRIs have been available for sale for more than 15 years. Fluvoxamine (Luvox®), fluoxetine (Prozac®), ser- traline (Zoloft®), paroxetine (Paxil®), and citalopram (Celexa®) are the five SSRIs that are currently marketed. For a variety of reasons, these medications have completely changed the way that anxiety and depression are treated. First off, there are significant- ly less safety issues with SSRIs than with conventional drugs, including as possible dependence, cardiotoxicity, and overdose mortality. Second, patients find SSRIs more tolerable due to their better side effect profiles, which enhances patient compliance with therapy. Lastly, it seems that there are numerous therapeutic uses for SSRIs. These medications can be used to treat depression and dysthymia as well as a variety of anxiety disorders. Their useful- ness in treating eating disorders, PMDD, and maybe drug depen- dence treatment goes even beyond treating depression and anxiety. While SSRIs are frequently thought to be interchangeable, there are distinctions in their efficacy evidence and adverse effect pro- files that might help clinicians choose the right medication. The SSRI sertraline, which has been marketed in the US since 1991, will be the subject of this review. We'll talk about sertraline's phar- macology, clinical efficacy, safety, and tolerability before making some recommendations for its use in psychiatric pharmacotherapy. An FDA-approved selective serotonin reuptake inhibitor (SSRI) called sertraline (Zoloft®) is used to treat depression, panic disor- der, OCD, and post-traumatic stress disorder (PTSD). The method of action of sertraline, like other SSRIs, involves boosting sero- tonin availability in the central nervous system [45].
Materials and Methods
Study Design and Population
Samples were collected in the period between 5/30/2023 and 6/9/2023 in shelter centers in the Syrian Arab Republic through an electronic questionnaire that was created by the research team and published among the population on social networking sites. The samples were analyzed on a daily basis, and the sample selection method was convenience sampling size.
Our sample consists of 40 individual, of whom meet the inclu- sion and exclusion criteria. As the research design is of the type of cross-sectional study, the sample size was determined taking into account the confidence interval (95%) and the 5% confidence interval (margin of error ± 5%).
Participants who did not give us sufficient or illogical information were excluded. Children and the elderly were excluded. Adults of all ages who were exposed to the earthquake and who followed news of its occurrence on social media sites were included, de- pending on their educational level and standard of living. Males and females were included.
The electronic questionnaire was published through networking with Red Crescent volunteers in Aleppo Governorate, which facil- itated the questionnaire’s access to those affected.
The questionnaire is investigative, not diagnostic, and its primary goal is to identify the psychological effects and repercussions of the Syrian earthquakes.
Sample Techniques and Data Collection
In this study, a total of 40 participants were included. Those in- dividuals were affected by the previous earthquake in the city of Aleppo. The survey was spread in Arabic Language.
Data were collected using structured questionnaires. The survey was done two times the first one, people answered the questions before taking Placebo or Zoloft sertraline medicines. The first one contained 15 questions, while the second one contained 5 ques- tions.
All participants willingly volunteered to participate in the study, and there were no instances of refuse.
Data Management and Analysis
The data were entered into Microsoft Excel 2022 (Microsoft Cor- poration, New York, USA) for the purpose of generating figures and conducting preliminary analysis. This was done to compare the effects of both medicines over people who were affected by the earthquake.
Ethics Approval and Consent to Participate
Approval was obtained from the Council of the College of Phar- macy at Al-Sham Private University. The questionnaire includes information that participants must read before answering the ques- tionnaire and emphasizes the privacy and confidentiality of the data and participants. The information sheet also includes contact details and a brief overview that will be given.
Participants are free to withdraw from participation at any time during data collection. Their information will be discarded. Each questionnaire will have a digital code. The questionnaires will be stored with our principal investigator. The information sheet will be stored separately. The study will not cause any physical, psy- chological or social for any of the participants, does not require them to disclose any information of a sensitive nature, and partic- ipants did not receive any payment for participating in the survey.
Results
Our 40 participants answered all the questions of both surveys. As illustrated in the tables below:
|
Question |
First survey |
|
|
|
|
Gender |
Females 57.5% |
Males 42.5% |
|
|
|
Economic status |
Good 60% |
Moderate 12.5% |
Bad 27.5% |
|
|
Marital Status |
Married 70% |
Single 30% |
|
|
|
Educational status |
Post-grad 82.5% |
Under-grad 10% |
School or none 7.5% |
|
|
Previous experience in earthquakes |
Yes 50% |
No 50% |
|
|
|
Staying under rubble |
Yes 5% |
No 95% |
|
|
|
Feeling during earthquake |
Panic 55% |
Extreme fear 30% |
Mild fear 20% |
None 5% |
|
Fear remaining |
Month or less 42.5% |
Two months 27.5% |
3 months 30% |
|
|
Need for taking sedative |
Yes 17.5% |
No 82.5% |
|
|
|
Psychotherapy sessions |
Yes 2.5% |
No 97.5% |
|
|
|
Social support |
Yes 42.5% |
No 57.5% |
|
|
|
Death of loved ones |
Yes 12.5% |
No 87.5% |
|
|
|
Hyper vigilance |
Yes 57.5% |
No 42.5% |
|
|
|
Loss of concentration |
Yes 70% |
No 30% |
|
|
|
Reviving the event |
Yes 70% |
No 30% |
|
|
Table 1: The Acquired Data Related to Questionnaire Sheet 1
Second questionnaire
|
Question |
|
|
|
|
Feeling after taking medicines |
Relaxation 35% |
Calmness 25% |
Nothing 40% |
|
Remaining of fear |
Yes 22.5% |
No 77.5% |
|
|
Decreasing in fear |
Yes 80% |
No 20% |
|
|
Recovery after taking medicines |
Yes 77.5% |
No 22.5% |
|
Table 2: The Acquired Data Related to Questionnaire Sheet 2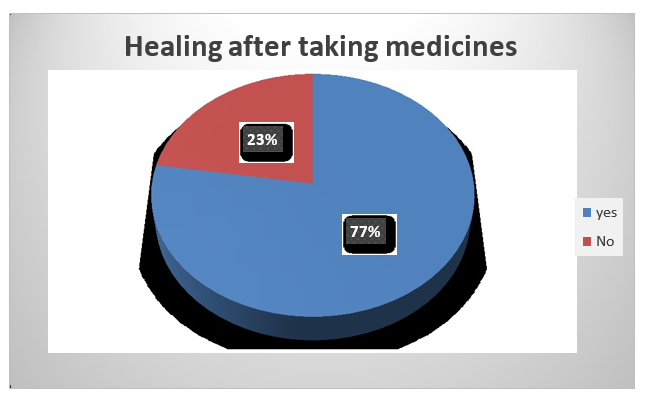
Figure 1: The Rate of Healing After Taking the Medicine
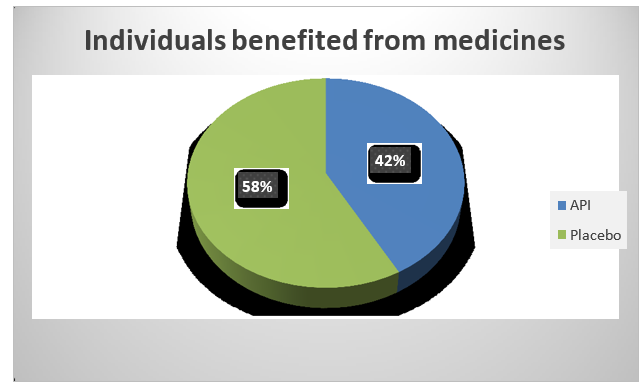
Figure 2: The Rate of Individuals Benefited from the Medicine
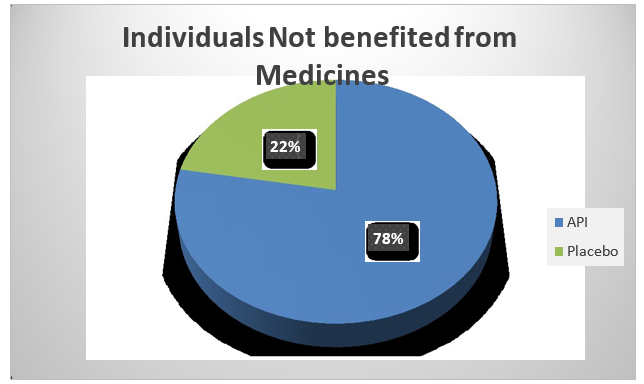
Figure 3: The Rate of Individuals Not Benefited from the Medicine
Discussion
This study presents information on the prevalence of PTSD fol- lowing the earthquake in Turkey and Syria. Additionally, it sheds light on potential interventions aimed at improving the overall mental health of Syrian people in Aleppo city, and to the best of our knowledge it’s the first study that compare two groups of peo- ple who were given an antidepressant medication and a placebo one.
A questionnaire was conducted before and after they took the medication in order to find out whether the effects of exposure to such incidents had diminished or not. The largest percentage of participants were females in both questionnaires, at a rate of 57.5%, while the percentage of males was about 42.5%, with the age group between 30-40 years predominant at 45%, followed by the age group from 18-30 years at a rate of 25%, and the age group from 50-60 at a rate 18%, then the age group of 40-50% by 12%. Thus, this study differed from a previous study conducted in 2023 on the earthquake in Syria and Turkey, where the majority percent- age was for the age group of 20-30 years, by more than 50% [4].
Sertraline has been linked to improvements on the majority of effi- cacy metrics and has been demonstrated to lower the mean weekly frequency of panic attacks [45]. When compared to men, women seemed to experience the sertraline impact more strongly. Despite this, the study lacked the power to adequately investigate gender disparities [45]. Furthermore, sertraline showed a noteworthy en- hancement in the quality of life metrics [45].
Longer term studies of sertraline in patients with psychological disorders have found that benefits are maintained with continued treatment. Studies have found that sertraline (50–200 mg) is more effective than placebo for the treatment of psychological disorders, with a trend towards greater efficacy with higher dosages [45]. The amount of sertraline drug was 50 mg, which accounts for the pla- cebo's superiority over the sertraline drug because the sertraline amount was insufficient to outweigh the placebo's effects. Despite this, the three-month medication regimen allowed sertraline ample time to have the desired benefits on depressed individuals.
The act of swallowing a pill could potentially enhance the ther- apeutic outcome of a placebo. Studies on the impact of pill con- sumption on depression in general are lacking. However, some evidence indicates that taking pills by themselves may have an impact on health [44].
The notion that pills represent the doctor's curing ability in our culture has been linked to the apparent health benefits of pill con- sumption.
The psychological advantages of a pill's symbolic significance might also be enhanced by conditioning effects stemming from favorable prior experiences with medication [44].
This can explain the results of our current study, as the results of the second questionnaire showed that the majority of people who benefited from the drug (77.5%) were those who benefited after taking the placebo, as the feeling of fear and anxiety disappeared by a large percentage of about 80%.
Certain patients are more likely to improve when treated with a placebo, according to studies on the placebo response in depres- sion. Episode duration is the most reliable and consistent indicator of placebo response. The placebo response drops to less than 30% for patients who have been depressed for more than a year, where- as it hovers around 50% for those who have been depressed for less than three months [44].
The National Institute of Mental Health Treatment of Depression Collaborative Research Program (TDCRP), the largest and most well-known controlled treatment trial, found that, when compared to cognitive therapy and antidepressant medications, placebo was the most successful way to treat depressed participants [46].
The results of this study can explain how placebo drugs can play on psychological side, in addition to time that can treat some of the bad memories among individuals [47-53].
References
- WHO. (2023). Syria/Turkey Earthquakes Situation Report #7,March 8, 2023.
- Thoits, P. A. (2011). Mechanisms linking social ties and support to physical and mental health. Journal of health and social behavior, 52(2), 145-161.
- Alfuqaha, O. A., Al-Masarwah, U. M., Farah, R. I., Yasin,J. A., Alkuttob, L. A., Muslieh, N. I., ... & Alshubbak, N. A. H. (2023). The impact of Turkey and Syria earthquakes on university students: Posttraumatic stress disorder symptoms, meaning in life, and social support. Behavioral Sciences, 13(7), 587.
- Kokai, M., Fujii, S., Shinfuku, N., & Edwards, G. (2004). Natural disaster and mental health in Asia. Psychiatry and clinical neurosciences, 58(2), 110-116.
- Norris, F. H., Friedman, M. J., Watson, P. J., Byrne, C. M., Diaz, E., & Kaniasty, K. (2002). 60,000 disaster victims speak: Part I. An empirical review of the empirical literature, 1981—2001. Psychiatry, 65(3), 207-239.
- Galea, S., Nandi, A., & Vlahov, D. (2005). The epidemiology of post-traumatic stress disorder after disasters. Epidemiologic reviews, 27(1), 78-91.
- Neria, Y., Gross, R., Marshall, R. D. (2006). 9/11: Mental Health in the Wake of Terrorist Attacks. Cambridge University Press.
- Sprang, G. (1999). Post-disaster stress following the Oklahoma City bombing: An examination of three community groups. Journal of Interpersonal Violence, 14(2), 169-183.
- David, D., Mellman, T. A., Mendoza, L. M., Kulickâ?Bell, R., Ironson, G., & Schneiderman, N. (1996). Psychiatric morbidity following hurricane Andrew. Journal of Traumatic stress, 9(3), 607-612.
- Norris, F. H. (1992). Epidemiology of trauma: frequency and impact of different potentially traumatic events on different demographic groups. Journal of consulting and clinical psychology, 60(3), 409-418.
- Norris, F. H., Kaniasty, K., Conrad, M. L., Inman, G. L., & Murphy, A. D. (2002). Placing age differences in cultural context: A comparison of the effects of age on PTSD after disasters in the United States, Mexico, and Poland. Journal of Clinical Geropsychology, 8(3), 153-173.
- Neria, Y., Nandi, A., & Galea, S. (2008). Post-traumatic stress disorder following disasters: a systematic review. Psychological medicine, 38(4), 467-480.
- Galea, S., & Resnick, H. (2005). Posttraumatic stress disorder in the general population after mass terrorist incidents: Considerations about the nature of exposure. CNS spectrums, 10(2), 107-115.
- Carr, V. J., Lewin, T. J., Kenardy, J. A., Webster, R. A., Hazell, P. L., Carter, G. L., & Williamson, M. (1997). Psychosocial sequelae of the 1989 Newcastle earthquake: III. Role of vulnerability factors in post-disaster morbidity. Psychological Medicine, 27(1), 179-190.
- Carr, V. J., Lewin, T. J., Webster, R. A., Kenardy, J. A., Hazell,P. L., & Carter, G. L. (1997). Psychosocial sequelae of the 1989 Newcastle earthquake: II. Exposure and morbidity profiles during the first 2 years post-disaster. Psychological Medicine, 27(1), 167-178.
- Van Griensven, F., Chakkraband, M. S., Thienkrua, W., Pengjuntr, W., Cardozo, B. L., Tantipiwatanaskul, P., ... & Thailand Post-Tsunami Mental Health Study Group. (2006). Mental health problems among adults in tsunami-affected areas in southern Thailand. Jama, 296(5), 537-548.
- Norris, F. H., Perilla, J. L., Riad, J. K., Kaniasty, K., & Lavizzo, E. A. (1999). Stability and change in stress, resources, and psychological distress following natural disaster: Findings from Hurricane Andrew. Anxiety, Stress & Coping, 12(4), 363-396.
- Wang, X., Gao, L., Shinfuku, N., Zhang, H., Zhao, C., & Shen, Y. (2000). Longitudinal study of earthquake-related PTSD in a randomly selected community sample in north China. American journal of psychiatry, 157(8), 1260-1266.
- BaÅ?oǧlu, M., Kiliç, C., Å?alcioǧlu, E., & Livanou, M. (2004). Prevalence of posttraumatic stress disorder and comorbid depression in earthquake survivors in Turkey: an epidemiological study. Journal of Traumatic Stress: Oficial Publication of The International Society for Traumatic Stress Studies, 17(2), 133-141.
- McFarlane, A. C. (1988). The aetiology of post-traumatic stress disorders following a natural disaster. The British Journal of Psychiatry, 152(1), 116-121.
- Shalev, A. Y., & Freedman, S. (2005). PTSD following terrorist attacks: a prospective evaluation. American Journal of Psychiatry, 162(6), 1188-1191.
- Goenjian, A. K., Najarian, L. M., Pynoos, R. S., Steinberg, A. M., Manoukian, G., Tavosian, A., & Fairbanks, L. A. (1994). Posttraumatic stress disorder in elderly and younger adults after the 1988 earthquake in Armenia. American Journal of Psychiatry, 151(6), 895-901.
- Deering, C. G., Glover, S. G., Ready, D., Eddleman, H. C., & Alarcon, R. D. (1996). Unique patterns of comorbidity in posttraumatic stress disorder from different sources of trauma. Comprehensive psychiatry, 37(5), 336-346.
- Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A., & Keane, T. M. (1993, October). The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. In annual convention of the international society for traumatic stress studies, San Antonio, TX (Vol. 462).
- Lai, T. J., Chang, C. M., Connor, K. M., Lee, L. C., & Davidson, J. R. (2004). Full and partial PTSD among earthquake survivors in rural Taiwan. Journal of psychiatric research, 38(3), 313-322.
- BaÅ?oǧlu, M., Å?alcioǧlu, E., & Livanou, M. (2002). Traumatic stress responses in earthquake survivors in Turkey. Journal of Traumatic Stress: Oficial Publication of The International Society for Traumatic Stress Studies, 15(4), 269-276.
- Goenjian, A. K., Molina, L., Steinberg, A. M., Fairbanks, L. A., Alvarez, M. L., Goenjian, H. A., & Pynoos, R. S. (2001). Posttraumatic stress and depressive reactions among Nicaraguan adolescents after Hurricane Mitch. American journal of psychiatry, 158(5), 788-794.
- Hsu, C. C., Chong, M. Y., Yang, P., & Yen, C. F. (2002). Posttraumatic stress disorder among adolescent earthquake victims in Taiwan. Journal of the American Academy of Child & Adolescent Psychiatry, 41(7), 875-881.
- Yang, Y. K., Yeh, T. L., Chen, C. C., Lee, C. K., Lee, I. H., Lee, L. C., & Jeffries, K. J. (2003). Psychiatric morbidity and posttraumatic symptoms among earthquake victims in primary care clinics. General Hospital Psychiatry, 25(4), 253-261.
- Chang, C. M., Lee, L. C., Connor, K. M., Davidson, J. R., Jeffries, K.,&Lai,T.J.(2003).Posttraumatic distress andcoping strategies among rescue workers after an earthquake. The Journal of nervous and mental disease, 191(6), 391-398.
- Chou, F. H. C., Su, T. T. P., Chou, P., Ou-Yang, W. C., Lu, M. K., & Chien, I. C. (2005). Survey of psychiatric disorders in a Taiwanese village population six months after a major earthquake. Journal of the Formosan Medical Association, 104(5), 308-317.
- Livanou, M., Bassoglu, M., Ssalcioglu, E., & Kalendar, D. (2002). Traumatic stress responses in treatment-seeking earthquake survivors in Turkey. The Journal of nervous and mental disease, 190(12), 816-823.
- Salcıoglu, E., Basoglu, M., & Livanou, M. (2003). Two- year psychological outcome in survivors of earthquake in Turkey. Journal of Nervous and Mental Disease, 107, 18-24.
- BaÅ?oÄ?lu, M., Livanou, M., Å?alcioÄ?lu, E., & Kalender, D. (2003). A brief behavioural treatment of chronic post-traumatic stress disorder in earthquake survivors: results from an open clinical trial. Psychological Medicine, 33(4), 647-654.
- Goenjian, A. K., Steinberg, A. M., Najarian, L. M., Fairbanks, L. A., Tashjian, M., & Pynoos, R. S. (2000). Prospective study of posttraumatic stress, anxiety, and depressive reactions after earthquake and political violence. American Journal of Psychiatry, 157(6), 911-916.
- Najarian, L. M., Goenjian, A. K., Pelcovttz, D., Mandel, F., & Najarian, B. (1996). Relocation after a disaster: Posttraumatic stress disorder in Armenia after the earthquake. Journal of the American Academy of Child & Adolescent Psychiatry, 35(3), 374-383.
- Giannopoulou, I., Strouthos, M., Smith, P., Dikaiakou, A., Galanopoulou, V., & Yule, W. (2006). Post-traumatic stress reactions of children and adolescents exposed to the Athens 1999 earthquake. European Psychiatry, 21(3), 160-166.
- Sharan, P., Chaudhary, G., Kavathekar, S. A., & Saxena, S. (1996). Preliminary report of psychiatric disorders in survivors of a severe earthquake. The American Journal of Psychiatry, 153(4), 556-558.
- Breslau, N., Davis, G. C., Andreski, P., Peterson, E. L., & Schultz, L. R. (1997). Sex differences in posttraumatic stress disorder. Archives of general psychiatry, 54(11), 1044-1048.
- De La Fuente, R. (1990). The mental health consequences of the 1985 earthquakes in Mexico. International Journal of Mental Health, 19(2), 21-29.
- Chen, C. H., Tan, H. K. L., Liao, L. R., Chen, H. H., Chan, C. C., Cheng, J. J. S., ... & Lu, M. L. (2007). Long- term psychological outcome of 1999 Taiwan earthquake survivors: a survey of a high-risk sample with property damage. Comprehensive psychiatry, 48(3), 269-275.
- Bland, S. H., O'leary, E. S., Farinaro, E., Jossa, F., Krogh, V., Violanti, J. M., & Trevisan, M. (1997). Social network disturbances and psychological distress following earthquake evacuation. The Journal of nervous and mental disease, 185(3), 188-195.
- World Health Organization. (1992). The ICD-10 classification of mental and behavioural disorders: clinical descriptions and diagnostic guidelines (Vol. 1). World Health Organization.
- Brown, W. A. (1994). Placebo as a treatment for depression. Neuropsychopharmacology, 10(4), 265-269.
- McRae, A. L., & Brady, K. T. (2001). Review of sertraline and its clinical applications in psychiatric disorders. Expert Opinion on Pharmacotherapy, 2(5), 883-892.
- Dimidjian, S., Hollon, S. D., Dobson, K. S., Schmaling, K. B., Kohlenberg, R. J., Addis, M. E., ... & Jacobson, N. S. (2006). Randomized trial of behavioral activation, cognitive therapy, and antidepressant medication in the acute treatment of adults with major depression. Journal of consulting and clinical psychology, 74(4), 658.
- Altindag, A., Ozen, S., & Sir, A. (2005). One-year follow- up study of posttraumatic stress disorder among earthquake survivors in Turkey. Comprehensive psychiatry, 46(5), 328- 333.
- Salcioglu, E., Basoglu, M., & Livanou, M. (2003). Long-term psychological outcome for non-treatment-seeking earthquake survivors in Turkey. The Journal of nervous and mental disease, 191(3), 154-160.
- Durkin, M. E. (1993). Major depression and post-traumatic stress disorder following the Coalinga and Chile earthquakes: a cross-cultural comparison. Journal of Social Behavior and Personality, 8(5), 405.
- Kulkarni, M., & Pole, N. (2008). Psychiatric distress among Asian and European American survivors of the 1994 Northridge earthquake. The Journal of nervous and mental disease, 196(8), 597-604.
- Beals, J., Manson, S. M., Shore, J. H., Friedman, M., Ashcraft, M., Fairbank, J. A., & Schlenger, W. E. (2002). The prevalence of posttraumatic stress disorder among American Indian Vietnam veterans: disparities and context. Journal of Traumatic Stress: Oficial Publication of The International Society for Traumatic Stress Studies, 15(2), 89-97.
- Santos, M. R., Russo, J., Aisenberg, G., Uehara, E., Ghesquiere, A., & Zatzick, D. F. (2008). Ethnic/racial diversity and posttraumatic distress in the acute care medical setting. Psychiatry: Interpersonal and Biological Processes, 71(3), 234-245.
- Wikman, A., Bhattacharyya, M., Perkins-Porras, L., & Steptoe, A. (2008). Persistence of posttraumatic stress symptoms 12 and 36 months after acute coronary syndrome. Psychosomatic medicine, 70(7), 764-772.