

Research Article - (2026) Volume 9, Issue 1
A Clinical Governance Intervention Framework: Empowering Nurse and Clinical Managers to Improve Patient Flow and Reduce Distress in Public Sector Emergency Units in Gauteng
Received Date: Feb 02, 2026 / Accepted Date: Feb 27, 2026 / Published Date: Mar 09, 2026
Copyright: ©2026 Thizwilondi Ananias Magadze. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Magadze, T. A. (2026). A Clinical Governance Intervention Framework: Empowering Nurse and Clinical Managers to Improve Patient Flow and Reduce Distress in Public Sector Emergency Units in Gauteng. Adv Neur Neur Sci, 9(1), 01-06.
Abstract
Chronic overcrowding and access block in public sector Emergency Centres (ECs) in South Africa, particularly in academic hospitals like Dr. George Mukhari Academic Hospital (DGMAH), significantly compromise patient safety and staff well-being. This study aimed to develop a practical and workable Clinical Governance Intervention Framework (CGIF) to empower Nurse and Clinical Managers in improving patient flow and reducing distress within the DGMAH EC. Employing a mixed-methods design, the study first quantitatively assessed the correlation between managerial clinical leadership practices and patient flow metrics (e.g., Length of Stay). Subsequently, qualitative interviews explored the barriers, enablers, and effective strategies utilized by managers. Findings confirmed that strong managerial leadership in clinical governance specifically in risk management and inter-departmental liaison was inversely correlated with patient waiting times. The resulting CGIF provides a structured, three-tiered approach focusing on Real-time Data Utilization, Inter-Departmental Escalation Protocols, and UnitSpecific Quality Improvement Cycles. This framework offers practical, low-cost solutions for managerial intervention, which is critical for transforming the quality of care in highly distressed public EC environments.
Keywords
Emergency Centre Overcrowding, Clinical Governance, Patient Flow, Managerial Leadership, Access Block
Introduction
Background and Context
The Emergency Centre (EC) serves as a vital access point to the healthcare system, yet in many public academic hospitals in South Africa, it operates under conditions of extreme strain [1]. Dr. George Mukhari Academic Hospital (DGMAH), located in the Gauteng province, is a tertiary-level institution experiencing persistent overcrowding, often termed “access block” [2]. Access block occurs when admitted patients cannot be moved to inpatient wards due to a lack of bed capacity, causing a cascade of delays throughout the EC [3]. The consequence is detrimental: increased patient mortality and morbidity, compromised staff morale, delayed initiation of critical care, and heightened distress for both patients and healthcare providers [4].
The Role of Clinical Governance
Clinical Governance is defined as a framework through which National Health Service organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care, by creating an environment in which excellence in clinical care will flourish [5]. In the context of EC overcrowding, the effectiveness of clinical governance hinges on local operational leadership— specifically that provided by Nurse and Clinical Managers [6]. These managers are uniquely positioned to translate high-level quality mandates into daily operational improvements concerning triage, patient flow, and inter-departmental communication. However, a structured framework to empower these managers with specific, evidence-based tools to address overcrowding in the local DGMAH context remains absent.
Problem Statement
Despite the clear mandate for continuous quality improvement, the persistent overcrowding at DGMAH EC demonstrates a gap in the effective operationalization of clinical governance principles by unit-level Nurse and Clinical Managers. The lack of a tailored, practical intervention framework limits their ability to: a) Proactively manage the flow of patients; b) Effectively escalate bed block issues; and c) Sustain a culture of quality improvement that targets the root causes of distress. This study addresses this gap by developing a practical, context-specific Clinical Governance Intervention Framework (CGIF) for DGMAH EC managers.
Research Aim and Objectives
Overall Aim: To develop a practical Clinical Governance Intervention Framework (CGIF) to empower Nurse and Clinical Managers to improve patient flow and reduce distress within the Dr. George Mukhari Academic Hospital Emergency Centre.
Specific Objectives:
• To quantitatively assess the correlation between managerial clinical leadership practices (e.g., risk monitoring, audit frequency) and key patient flow metrics (e.g., average waiting time to bed allocation) at the DGMAH EC.
• To qualitatively explore the perceived barriers and effective strategies employed by Nurse and Clinical Managers in implementing clinical governance standards to manage access block at DGMAH EC.
• To develop an evidence-based, practical Clinical Governance Intervention Framework (CGIF) tailored to the resource-constrained environment of the DGMAH EC.
Literature Review
The Global Crisis of Emergency Centre Crowding
EC crowding is a global phenomenon, but the drivers and impact are amplified in low- and middle-income countries, where resource limitations are severe [7]. Studies consistently link EC crowding to negative outcomes, including increased inhospital mortality and adverse events [8,9]. The primary cause is often identified as Access Block the inability to transfer admitted patients to inpatient units which is an institutional, rather than EC-specific, failure [3].
Clinical Governance and Managerial Accountability
Clinical governance requires a system of accountability where managers are responsible for the quality of care delivered within their sphere [5]. In the EC, this translates to the manager’s oversight of four key domains: Risk Management (e.g., maintaining a risk register of flow failures), Clinical Audit (e.g., auditing compliance with triage policies), Staff Development, and Effective Communication [6]. Effective clinical leadership, particularly in the form of inter-departmental liaison and proactive problem-solving, is crucial for mitigating the systemic failures that cause EC overcrowding [4].
The Gap in Practical Frameworks
While the importance of managerial leadership in quality improvement is well-established, many clinical governance models are theoretical and lack the specific, actionable steps necessary for resource-constrained public hospitals in Gauteng [2]. The literature suggests that successful interventions often involve low-cost, high-impact managerial actions such as implementing structured communication and escalation plans [10]. This study aims to synthesise these principles into a practical framework specifically for DGMAH.
Methodology
Study Design
A Sequential Explanatory Mixed-Methods Design (QUAN & QUAL) was utilised [11]. This design involved an initial quantitative phase to identify correlations, followed by a qualitative phase to explain and elaborate upon the findings, ensuring the resulting framework is both statistically supported and contextually rich.
Study Setting and Population
The study was conducted at the Emergency Centre of Dr. George Mukhari Academic Hospital (DGMAH) in Pretoria, Gauteng.
• Quantitative Sample: Retrospective data on patient flow and managerial activity data were collected from 30 operational weeks (spanning 6 months) to capture cyclical variations in the EC.
• Qualitative Sample: A purposive sample of 8 key managerial personnel directly involved in the DGMAH EC operations was selected, including the Unit Nurse Manager, two Charge Nurses, the Clinical Manager (Head of Department), and two managers from key liaison departments (e.g., Internal Medicine, Hospital Management).
Data Collection
Phase 1: Quantitative Data (QUAN)
• Managerial Clinical Leadership (Independent Variable): Weekly records were audited to track the frequency of specific managerial actions indicative of governance: o Frequency of documented EC risk register reviews (Focusing on flow risks). Frequency of inter-departmental (EC-Inpatient) meetings focused on access block. Frequency of clinical audit completion (e.g., triage compliance audit).
• Patient Flow Metrics (Dependent Variable): Retrospective EC operational data were collected weekly: Average Waiting Time (AWT) to Inpatient Bed Allocation (Primary measure of access block). o Total EC Length of Stay (LOS) for admitted patients.
Phase 2: Qualitative Data (QUAL)
Semi-structured interviews were conducted with the purposive sample of 8 managers. The interview guide focused on:
• “Describe the biggest recurrent barrier to moving admitted patients out of the EC.”
• “What proactive steps do you currently take to manage periods of anticipated crowding?”
• “What support or tools would significantly enhance your ability to manage flow and reduce staff distress?”
Data Analysis
• QUAN Analysis: Pearson correlation analysis (r) was used to assess the linear relationship between the weekly frequency of managerial governance actions and the AWT to Bed Allocation. Statistical significance was set at p < 0.05$. Regression analysis was used to model the predictive relationship.
• QUAL Analysis: Interview transcripts were analysed using thematic analysis [12]. This involved coding the data to identify recurrent themes related to barriers, effective strategies, and unmet needs, which would directly inform the framework development.
Ethical Considerations
Ethical approval was obtained from the Research Ethics Committee of the institution and permission was granted by the hospital CEO (DGMAH, 2023). Confidentiality was ensured by anonymising all data and reporting findings only in aggregate. Participation was voluntary, and informed consent was obtained from all interviewees.
Findings
Quantitative Findings
The analysis of the 30 weeks of operational data revealed significant correlations between managerial governance practices and patient flow metrics:
|
Managerial Governance Action (Independent Variable) |
AWT to Bed Allocation (r) |
Total EC pvalue LOS (r) |
|
Frequency of Risk Register Review |
-0.52 |
-0.39 <0.01 |
|
Frequency of Inter-departmental Meetings |
of |
-0.48 <0.001 |
|
Frequency of Clinical Audit Completion |
-0.15 |
-0.10 0.40 |
The results show a statistically significant negative correlation between the frequency of documented Risk Register Reviews (r = -0.45, p < 0.01) and Inter-departmental Meetings (r = -0.52, p < 0.001) and the Average Waiting Time (AWT) to Inpatient Bed Allocation. This suggests that the more frequently managers engage in structured risk monitoring and collaborative meetings with other departments, the faster patients are transferred out of the EC. The frequency of routine Clinical Audit Completion showed no significant correlation with the flow metrics.
Qualitative Findings
Thematic analysis of the interviews yielded three key themes:
Theme 1: The Dominance of “The Output Problem” (Access Block)
All managers unequivocally identified the lack of inpatient bed capacity and slow patient discharge from wards as the single greatest driver of EC distress.
“We can manage the waiting room; we can do better triage. But when we have ten admitted patients in our beds who have nowhere to go for twelve hours, our flow collapses. That’s not an EC problem; that’s a hospital problem we have to absorb.”
(Participant 2, Nurse Manager)
Theme 2: The Need for Structured and Empowered Escalation
Managers reported that current escalation pathways were informal, reliant on personal relationships, and lacked clear accountability, making it difficult to force timely bed allocation.
“It’s often a shouting match, or I have to call the CEO’s ofice. There is no oficial ‘red alert’ that automatically triggers action from the ward managers or the hospital duty manager.
I need a tool that gives me the authority to declare an emergency status.” (Participant 5, Charge Nurse)
Theme 3: Demand for Real-Time, Simplified Data Tools
Managers acknowledged the importance of data but found the existing hospital information systems too complex or delayed. They desired simple, real-time visualizations for decision-making. “I can get a report from a week ago, but I need to know right now which ward has the most discharges pending and who is blocking the flow. I need a visible dashboard that I can use to show the medical teams the gravity of the situation in real-time.” (Participant 7, Clinical Manager)
Discussion
Validation of Managerial Clinical Leadership
The quantitative findings strongly validate the premise that managerial attention to clinical governance matters in high-acuity environments [6]. The significant negative correlation between AWT and the frequency of risk reviews and interdepartmental meetings (r -0.45) suggests that these proactive, systemic leadership activities are more effective in managing EC crowding than internal, unit-based compliance audits (which showed no significance). This reinforces the literature that EC overcrowding is an institutional flow problem requiring inter-departmental cooperation, not simply an EC efficiency problem [3]. Effective managers are those who consistently engage in boundary-spanning activities.
Practical Solutions from Qualitative Insights
The qualitative data highlighted that the most effective solutions must be practical, actionable, and address the “Output Problem” (Theme 1). The managers’ demand for a structured escalation protocol (Theme 2) and simplified data tools (Theme 3) forms the foundation of the proposed framework. Traditional governance focuses on paper compliance; the proposed framework focuses on operational empowerment giving managers the tools to enforce accountability and utilise real-time data for high-stakes decision-making.
Limitations
The study was confined to a single academic hospital (DGMAH) in Gauteng, which limits the direct generalisability of the quantitative correlations. However, the qualitative insights regarding the barriers (access block) and needs (escalation authority, real-time data) are highly likely to be representative of other public academic ECs in South Africa.
The Clinical Governance Intervention Framework (CGIF)
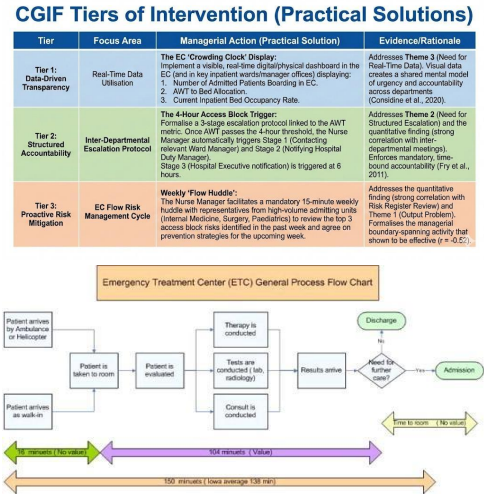
Based on the convergent findings, the following Clinical Governance Intervention Framework (CGIF) is proposed for implementation by Nurse and Clinical Managers at DGMAH. The framework focuses on low-cost, high-impact managerial actions.

Figure 1
|
Tier |
Focus Area |
Managerial Action (Practical Solution) |
Evidence/Rationale |
|
Tier 1: Data-Driven Transparency |
Real-Time Data Utilisation |
The EC “Crowding Clock” Display: Implement a visible, real-time digital/ physical dashboard in the EC (and in key inpatient wards/manager offices) displaying: 1. Number of Admitted Patients Boarding in EC. 2. AWT to Bed Allocation. 3. Current Inpatient Bed Occupancy Rate. |
Addresses Theme 3 (Need for Real-Time Data). Visual data creates a shared mental model of urgency and accountability across departments (Considine et al., 2020). |
|
Tier |
Focus Area |
Managerial Action (Practical Solution) |
Evidence/Rationale |
|
Tier 2: Structured Accountability |
Inter-Departmental Escalation Protocol |
The 4-Hour Access Block Trigger: Formalise a 3-stage escalation protocol linked to the AWT metric. Once AWT passes the 4-hour threshold, the Nurse Manager automatically triggers Stage 1 (Contacting relevant Ward Manager) and Stage 2 (Notifying Hospital Duty Manager). Stage 3 (Hospital Executive notification) is triggered at 6 hours. |
Addresses Theme 2 (Need for Structured Escalation) and the quantitative finding (strong correlation with interdepartmental meetings). Enforces mandatory, time-bound accountability [4]. |
|
Tier 3: Proactive Risk Mitigation |
EC Flow Risk Management Cycle |
Weekly “Flow Huddle”: The Nurse Manager facilitates a mandatory 15-minute weekly huddle with representatives from high-volume admitting units (Internal Medicine, Surgery, Paediatrics) to review the top 3 access block risks identified in the past week and agree on prevention strategies for the upcoming week. |
Addresses the quantitative finding (strong correlation with Risk Register Review) and Theme 1 (Output Problem). Formalises the managerial boundary-spanning activity that was shown to be effective (r = -0.52). |
Table 1: CGIF Tiers of Intervention (Practical Solutions)
Conclusion
This study successfully established a clear link between structured clinical governance practices, driven by Nurse and Clinical Managers, and improved patient flow metrics in the highly distressed environment of the Dr. George Mukhari Academic Hospital Emergency Centre. By moving beyond theoretical compliance to focusing on practical managerial interventions specifically, Real-time Data Utilization, Structured Escalation, and InterDepartmental Risk Huddles the proposed Clinical Governance Intervention Framework (CGIF) offers an immediate, actionable strategy to mitigate access block, reduce patient distress, and enhance the quality of care in this critical public health setting. The framework empowers local leadership with the tools necessary to enforce accountability and drive systemic, hospital-wide flow improvement.
References
- National Department of Health. (2020). National emergency medical services policy. Pretoria: National Department of Health.
- Booysen, E. L., Govender, S. and Van Wyk, B. (2021). Patient overcrowding and its impact on the quality of emergency care in a South African setting. African Journal of Emergency Medicine, 11(2), pp. 138-144.
- Richardson, D. B. (2018). The access block crisis: International solutions and their applicability to Australian emergency departments. Emergency Medicine Australasia, 30(5), pp. 741-748.
- Fry, M., D’Arcy, P. and Middleton, S. (2011). Organisational and clinical factors associated with extended length of stay in the emergency department. Journal of Advanced Nursing,67(6), pp. 1279-1286.
- Scally, G. and Donaldson, L. J. (1998). Clinical governance and the drive for quality improvement in the new NHS in England. BMJ, 317(7150), pp. 61-65.
- Sibiya, M. A., Luthuli, T. N. and Dlamini, D. V. (2019). Clinical governance and quality improvement in South African public hospitals: A scoping review. African Journal of Primary Health Care & Family Medicine, 11(1), a1983.
- Hwang, J., Wiler, J., Pines, J. M., et al. (2017). Emergency department crowding: Lessons learned from international models. Academic Emergency Medicine, 24(2), pp. 248-255.
- Sprivulis, P. C., Da Silva, J. A., Jacobs, I. G., et al. (2007). The association between emergency department overcrowding and mortality and adverse events in admitted patients. Medical Journal of Australia, 184(6), pp. 249-253.
- Pines, J. M., Zocchi, M. S. and Hugh, D. M. (2017). The emergency department crowding crisis: Challenges and opportunities for improvement. The Journal of Emergency Medicine, 53(6), pp. 883-891.
- Considine, J., Shaban, R. Z. and Curtis, K. (2020). Improving emergency department patient flow: A systematic review of system, organisational, and patient-level factors. Academic Emergency Medicine, 27(11), pp. 1133-1144.
- Creswell, J. W. and Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approaches. 5th ed. Thousand Oaks, CA: SAGE Publications.
- Braun, V. and Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), pp. 77-101.