
Journal of Clinical Review & Case Reports(JCRC)
ISSN: 2573-9565 | DOI: 10.33140/JCRC
Impact Factor: 1.823

Case Report - (2025) Volume 10, Issue 6
A Case Report of Panhypopituitarism with Refractory Shock
2Department of Pharmacy, Wenzhou Medical University, Wenzhou, PR, China
Received Date: May 02, 2025 / Accepted Date: Jun 20, 2025 / Published Date: Jun 30, 2025
Copyright: ©Copyright: ©2025 Mohammed Kassim Salah. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Citation: Salah, M. K., AL Mokdad, A. S., Aldailami, M. A., Hussein, T., & Al-Zaazaai, A. A. (2025). A Case Report of Panhypopituitarism with Refractory Shock. J Clin Rev Case Rep, 10(6), 01-03.
Abstract
Background: The panhypopituitarism is a rare endocrine system disease; the clinical presentation of a panhypopituitarism patient can vary from asymptomatic or subclinical cases to life-threatening myxedema coma.
Case report: Our patient is 55 years old woman whow as presented to emergency department with chief complains of acute watery diarrhea with AKI complicated by refractory shock. After necessary workup, panhypopituitarism was diagnosed.
Discussion: There are different diagnoses for shock. Inpatients with vague complaints such as refractory shock, we should take their history carefully and perform clinical examinations with all investigations to reach a definitive diagnosis.
Keywords
Panhypopituitarism, Shock, Endocrine system disease
Introduction
Refractory shock is a potentially fatal manifestation of cardiovascular failure with inadequate response to vasopressors characterized by poor tissue perfusion, hypotension, and organ failure [1]. Refractory shock in panhypopituitarism arises from severe hormonal deficiencies, particularly adrenocorticotropic hormone (ACTH) deficiency, leading to adrenal insufficiency and life-threatening hypotension [2]. Management of refractory shock involves treating the cause and restoring organ perfusion with fluid resuscitation and vasopressors, and hormone replacement therapy.
Case Report
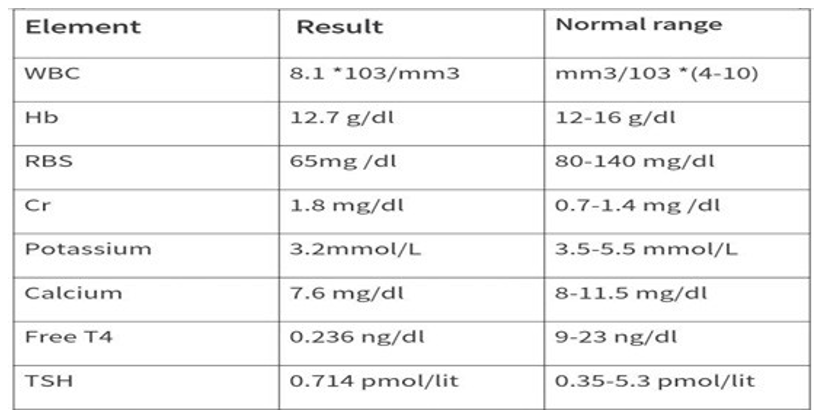
The patient was a 55 years old woman who complained of acute watery diarrhea and dehydration since 3 days ago. In the emergency department, the patient was hypotensive, with tachycardia. Signs of dehydration such as sunken eyes, delayed capillary refill time, and delayed skin turgor were observed in the general appearance. The patient was pale and there's mild pre-orbital edema. The lower extremities non-pitting edema was evident in both leg. Other examination findings were within normal limits. Primary lab test results were as the table. Then the patient was diagnosed as acute watery diarrhea follows in the due cholera complicated by AKI. Patient admitted to ICU and received adequate IV fluid and still hypotensive with no improvement and developed volume overload, then she was given dopamine with noradrenaline. Patient didn't respond to vasopressors and still hypotensive with confusion and AKI. Patient's TSH and free T4 were requested, and based in the results patient complains of hypothyroidism secondary to hypopituitarism. Finally, we prescribed her hydrocortisone 200 mg IV bolus followed by 100 mg every 8 hours and levothyroxine 0.1 mg daily. In subsequent follow-up the patient’s symptoms resolved and her life status had improve.
Discussion
In this case, we report a patient who was presented to the emergency department with complaints of acute watery diarrhea, dehydration, AKI, refractory shock, eventually panhypopituitarism was diagnosed. Patient did not respond to IV fluid therapy and vasopressors and still hypotensive. Septic shock first excluded. Thyroid function tests requested and results were low free T4 and TSH serum levels are suggested to secondary thyroid insufficiency in this patient. *the level of serum cortisol of the patient is done at 8 am, since the serum level is lower than 3 µg/dl, ACTH stimulation test is not needed. On the other hand, there is no evidence in the physical examination of patient for primary adrenal insufficiency (such as skin and mucosal pigmentation) and secondary adrenal insufficiency arises and at this situation we did not usually checked the ACTH hormone levels. MRI was not done to patient to evaluate the reasons of pituitary insufficiency that needs surgical intervention as the cause of pituitary apoplexy here is severe watery diarrhea that complicated by dehydration and AKI.
Panhypopituitarism is a rare disease with a high mortality. It is characterized by complete or partial deficiency of hormones secreted by the pituitary gland [3,4]. Its Prevalence is 45 per 100,000 populations, and its incidence is 4 per 100,000 populations [5]. There is a variety of causes for Panhypopituitarism, such as cranial surgery, radiotherapy and tumors, hereditary causes, infiltrative disease, infectious diseases and head trauma. Due to the underlying pathology, clinical symptoms are related to severity and speed of onset [3]. This condition may be created in high-energy head trauma. Any symptoms associated with hormonal disorders after head trauma requires the studies of pituitary function [6,7].
The clinical presentation of the panhypopituitarism patient can vary from asymptomatic or subclinical cases to life-threatening myxedema coma. Patient’s symptoms are different, related to which hormone is involved (including hypothyroidism, hypoadrenalism, hypogonadism, growth hormone disorder and hypoprolactinemia) [3,4]. Some patients may be referred with hyponatremia due to adrenal glands dysfunction, in spite of the necessary studies for the evaluation of patients with hyponatremia, checking the serum cortisol level is needed to rule out hypoadrenalism [8,9]. Signs and symptoms of the disease may persist for several years without diagnosis [5]. Suspicion of this disease, clinical examination and biochemical tests may be helpful in early diagnosis of the disease [3,4]. In these patients, due to the impairment of cortisol and thyroid hormones, QT prolongation and heart rhythm disorders may be existed [10,11].
Treatment of panhypopituitarism includes therapies of underlying cause with hormone replacement. The main goal of Hormone Replacement Therapy (HRT) is to achieve to normal levels of circulating hormones to restore the body’s natural physiology and relief of symptoms with minimal side effects. Mineralocorticoid replacement is not necessary in most cases because the renin- angiotensin system and potassium are the key regulators for aldosterone secretion [3].
Considering the extent of clinical signs of panhypopituitarism, in confronting with vague complaints with resistant to treatments, we must keep in mind hormonal disorders such as panhypopituitarism.
References
- Saguil A. (2005). Evaluation of the patient with muscle weakness. American family physician, 71(7), 1327–1336.
- Morchi S (2013) Weakness. Rosen’s Emergency Medicine. (8th edn), Elsevier Saunders, China 2: 124-128.
- Prabhakar, V. K., & Shalet, S. M. (2006). Aetiology, diagnosis, and management of hypopituitarism in adult life. Postgraduate medical journal, 82(966), 259–266.
- Fernandez-Rodriguez, E., Bernabeu, I., Andujar-Plata, P., & Casanueva, F. F. (2012). Subclinical hypopituitarism. Best practice & research. Clinical endocrinology & metabolism, 26(4), 461–469.
- Toogood, A. A., & Stewart, P. M. (2008). Hypopituitarism: clinical features, diagnosis, and management. Endocrinology and metabolism clinics of North America, 37(1), 235–x.
- Charfi, N., Abid, M., Mnif, M., Kammoun, S., Ben Hmida, C., Bouaziz, M., & Rekik, N. (2001). Insuffisance antéhypophysaire post-traumatique [Post-traumatic hypopituitarism]. Presse medicale (Paris, France : 1983), 30(2), 59–61.
- Benvenga, S., Campenní, A., Ruggeri, R. M., & Trimarchi, F. (2000). Clinical review 113: Hypopituitarism secondary to head trauma. The Journal of clinical endocrinology and metabolism, 85(4), 1353–1361.
- Diederich, S., Franzen, N. F., Bähr, V., & Oelkers, W. (2003). Severe hyponatremia due to hypopituitarism with adrenal insufficiency: report on 28 cases. European journal of endocrinology, 148(6), 609–617.
- Diederich, S., Franzen, N. F., Bähr, V., & Oelkers, W. (2003). Severe hyponatremia due to hypopituitarism with adrenal insufficiency: report on 28 cases. European journal of endocrinology, 148(6), 609–617.
- Arpaci, D., Demir, M. V., Garip, T., & Tamer, A. (2013). A Case of QT Prolongation Associated with Panhypopituitarism. Case reports in endocrinology, 2013, 989745.
- Ghosh, R., León-Ruiz, M., Roy, D., Sardar, S. S., Bandyopadhyay, S., Bole, K., Dubey, S., & Benito-León, J. (2022). Panhypopituitarism and Central Diabetes Insipidus Almost Three Decades After Russell's Viper Envenomation: A Remarkable Case Report and Literature Review. Medical research archives, 10(10), 10.18103/mra.v10i10.3195.