
Archives of Case Reports: Open Access(ACROA)
ISSN: 3065-7598 | DOI: 10.33140/ACROA


Short Communication - (2025) Volume 2, Issue 2
Young Man was Admitted to the Poisoning Emergency Room with Decreased Level of Consciousness
2Faeze Abbasloo, Board-Certified Internal Medicine Specialist, Tehran, University of Medical Sciences (TUMS), Tehran, Iran
3Associate professor of Emergency Medicine, Tehran University of Medical Sciences, Iran
Received Date: Sep 04, 2025 / Accepted Date: Oct 09, 2025 / Published Date: Oct 28, 2025
Copyright: ©2025 Faeze Abbasloo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kiaei. S. Z. F., Abbasloo, F., Talebian, T. M. (2025). Young Man was Admitted to the Poisoning Emergency Room with Decreased Level of Consciousness. Arch of case Rep: Open, 2(2), 01-03.
Abstract
Methadone (MTD) is a synthetic long-acting opioid receptor ag- onist that has potent analgesic effects. It is commonly used for detoxification or as a substitute in treating opium addiction. ARDS is a rare MTD-related condition causing acute respiratory distress, documented in the medical literature [1]. However, in most cases, methadone was consumed orally in the formation of tablets in high or unknown doses [2].
Keywords
ARDS, methadone, cannabis
Introduction
Methadone (MTD) is a synthetic long-acting opioid receptor agonist that has potent analgesic effects. It is commonly used for detoxification or as a substitute in treating opium addiction. ARDS is a rare MTD-related condition causing acute respiratory distress, documented in the medical literature [1]. However, in most cases, methadone was consumed orally in the formation of tablets in high or unknown doses [2].
The use of synthetic cannabinoids (SCs) as a substitute for marijuana and other similar substances that induce euphoria has rapidly increased in many countries. The prevalence of cannabis use in Iran is relatively low compared to many other countries. However, there is decisive evidence of a growth in cannabis use among youth, as well as some evidence of an increase in cannabis use disorder [3]. Cannabis use in juveniles has been related to negative physical health effects such as impaired cognitive performance, respiratory distress, lung injury, myocardial ischemia, seizures, oral health issues, weight loss, and cannabinoid hyperemesis syndrome [4].
In this article we present a case, who used methadone and cannabis and developed ARDS. The patient has clearly given written informed consent before this report was prepared. Patient anonymity was preserved wherever possible.
The patient a 22-year-old male, who was urgently transported to Baharloo Hospital due to a decrease in his level of consciousness. His family found him that morning, unconscious and making gurgling sounds, prompting them to call the EMS immediately. EMS personnel administered three ampoules (a total dose of 1.2 mg) of naloxone, which resulted in him becoming alert and oriented to person, time, and place when we assessed him in the Baharloo Hospital emergency department.
Initially, oxygen via a reservoir bag mask was administered due to hypoxemia. However, as his oxygen saturation was around 70% and failed to increase more, intubation was performed in the emergency department. Early intubation was necessary due to severe dyspnea, persistent hypoxemia, and excessive pulmonary secretions, which compromised his ability to protect his airway.
Following intubation, a lung CT scan (Figure. 1-A) revealed severe alveolar infiltration, and the patient was transferred to the Poisoning ICU ward. Despite receiving 100% oxygen (FiO2), oxygen saturation remained around 75% in SIMV mode with a PEEP of 5 cmH2O, Ti of 1.2 s ,TV of 500 ml, and airway secretion suctioning, which included significant pinkish fluid. His blood pressure and pulse rate were as follows: BP 93/40 mmHg, PR 112 bpm.
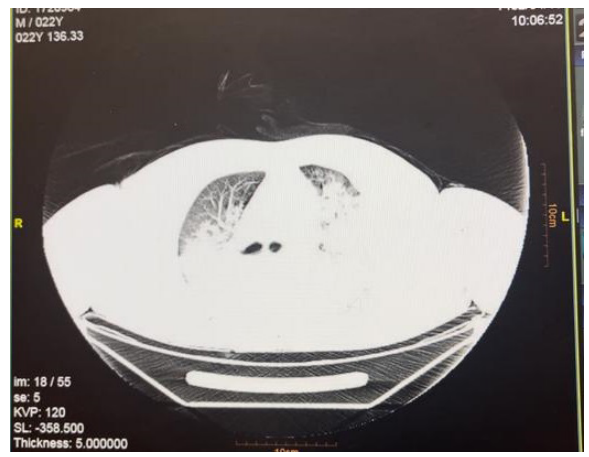
Figure 1-A: Chest CT Scan at Admission Day
A pulmonary CT scan revealed severe alveolar infiltration on both sides, while lab tests showed leukocytosis, high CRP levels, respiratory acidosis in VBG, and positive results for tetrahydrocannabinol and methadone in his screening test. Consequently, we initiated broad-spectrum antibiotics such as meropenem and vancomycin, suspecting massive aspiration pneumonia. Due to a PaO2/FiO2 ratio under 200, ventilator settings were adjusted following an ARDS diagnosis: PEEP 14 cmH2O, TV under 420 ml, Ti 1.7 s, which improved his oxygenation to an oxygen saturation of 90%. Gradually over the first 24 hours, his oxygen saturation increased to 100%, allowing a reduction in FiO2, Ti, and PEEP to 50%, 0.9, and 6, respectively.
On the third day, his chest X-ray showed significant improvement and a positive response to the treatment. Negative procalcitonin results, along with rapid lung recovery and reduced PEEP requirements, led to the decision to discontinue antibiotic administration. Extubation occurred on day 5, and the patient was discharged after a psychological consultation on the 10th day, during which he admitted to using a 10mg methadone tablet in combination with smoking a cannabinoid cigarette before losing consciousness.
A follow-up lung CT scan on the day of discharge revealed clear lung parenchyma with no visible remnants of previous opacities. (Figure. 1-B)
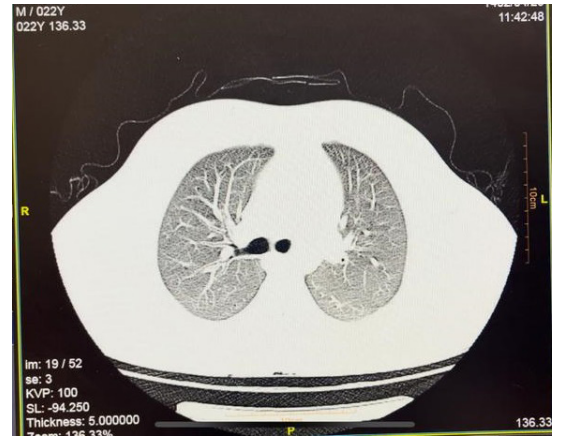
Figure 1-B: Chest CT Scan After Treatment
Acute respiratory distress syndrome is a complex disease that causes severe lung injury leading to respiratory distress. Acute Respiratory Distress Syndrome (ARDS) is a lung condition caused by inflammation triggered by both pulmonary and extrapulmonary factors. This inflammation causes damage to the alveolarcapillary membrane, resulting in increased permeability and the accumulation of fluid in the lungs. This condition is characterized by acute hypoxemic respiratory failure, reduced lung compliance, and bilateral infiltrates in chest radiographs, without any clinical evidence of cardiogenic pulmonary edema. ARDS typically occurs in patients without previous health issues. There are usually 18- 37 hours between the initial injury and the development of the clinical syndrome. After this period, symptoms of acute respiratory failure will appear. A precise assessment of abnormalities in lung mechanics and oxygenation is typically not performed until the patient is intubated and mechanically ventilated. Although this condition has been recognized for over a century, it was not until the landmark study by Ashbaugh et al. that it was fully understood [5].
Acknowledgement
The case was encountered during the author’s previous clinical practice at Tehran University of Medical Sciences.
References
- Drudi, F. M., Poggi, R., Trenta, F., Manganaro, F., & Iannicelli, E. (1997). A case of the adult respiratory distress syndrome induced by a methadone overdose. La Radiologia medica, 94(4), 393-396.
- Ridgway, Z. A., & Pountney, A. J. (2007). Acute respiratory distress syndrome induced by oral methadone managed with non-invasive ventilation. Emergency Medicine Journal, 24(9), 681-681.
- Rostam-Abadi, Y., Gholami, J., Amin-Esmaeili, M., Baheshmat, S., Hamzehzadeh, M., Rafiemanesh, H., ... & Rahimi-Movaghar, A. (2021). Evidence for an increase in cannabis use in Iran–A systematic review and trend analysis. PloS one, 16(8), e0256563.
- Harrell, M. B., Clendennen, S. L., Sumbe, A., Case, K. R., Mantey, D. S., & Swan, S. (2022). Cannabis vaping among youth and young adults: a scoping review. Current addiction reports, 9(3), 217-234.
- Ashbaugh, D., Bigelow, D. B., Petty, T., & Levine, B. (1967). A cute respiratory distress in adults. The Lancet, 290(7511), 319-323.