




Research Article - (2025) Volume 4, Issue 4
We Must Dismantle the Breast Cancer Tower of Babel Brick by Brick
Received Date: Sep 29, 2025 / Accepted Date: Oct 31, 2025 / Published Date: Nov 12, 2025
Copyright: ©2025 Phil Bretz, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Bretz, P., Mantik, D., Lynch, R., David, L., Stiles, A., et al. (2025). We Must Dismantle the Breast Cancer Tower of Babel Brick by Brick. J Surg Care, 4(4), 01-12.
Abstract
In our previous publications, we have elucidated the Lavender Way, a positive changing of the guard with respect to the diag- nosis and treatment of breast cancer. While our first publication was a clarion call for radical change, it did not specify, except for Lavender, how that could be accomplished. This paper will be a blueprint on how to eliminate the suffering wrought by breast cancer based on our experience of providing care to over 14,000 women. Forty years ago, we all thought that having huge cancer centers and a mammogram machine on every corner would end the devastation wrought by breast cancer. We were wrong. Now as AI overtakes many of the tasks normally done by humans, there will be much publicity from a mammogram center that has AI driven results women should flock to. They will also be wrong. One can’t dabble in just tweaking the outer edges, cleverly camouflaging the fact that if all this new technology finds something that patient will suffer mightily physically, psychologically, and financially. Why? Because as Dr. Raza says, “Cancer crushes hope, leaving a wasteland of grief, depres- sion, despair, and an unending sense of futility.” If doctors don’t see that or refuse to acknowledge it and refuse any change in the for-profit system 75% of doctors labor under, that’s the problem, coupled with a government blind to the true path needed to eliminate the suffering. What needs to be done?
Keywords
Breast Cancer, Cryoablation, Genetics, Infrared
Background
In the Bible man’s attempt to reach heaven constructing the Tower of Babel ended in disaster. So too is our modern version of that tower concerning breast cancer, placing one ‘breakthrough’ on top of another hasn’t budged the number of breast cancer yearly deaths in forty years except to continually go up now surpassing 43,000 yearly. That’s just the death toll, not the “Wasteland of grief, de- pression, despair, and the sense of unending futility, breast cancer leaves in its wake,” [1]. Not to mention in many cases total fi- nancial ruin. Not to mention fear of the cancer returning, fear of husbands leaving, fear of loss of femininity so there is no chance of getting a husband, and ultimately death, leaving behind their family. And not to mention the increased rate of suicide associated with breast cancer surgery [2].
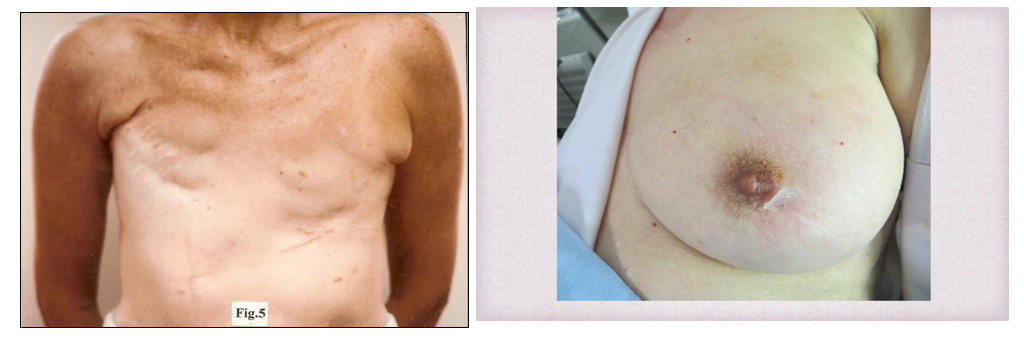
Choose any touted ‘breakthrough’ from the first mammograms called MAMMOMAT by Siemens in 1972, later using a selenium plate, to then file screen, to then digital mammography, to com- puter-assisted detection (CAD), and on the surgical side, from mastectomy to then lumpectomy, to then anti-estrogens, to then accelerated partial breast radiation, to then intraoperative radiation therapy (IORT), to then creating huge cancer centers and mammo- gram machines on every corner, and in the last forty years you’ll see escalation in the number of yearly deaths from breast cancer. You’ll also see an ever-increasing number of women fed up with the ‘fallow promises’ of ‘breakthroughs’ that don’t keep them out of harm’s way. Worse is now they are touting bilateral prophylac- tic mastectomy and the so-called drive-by mastectomy, (HRAM). The mounting disdain for the latest offering of AI assisted every- thing has produced a burgeoning number of women refusing mam- mography and breakthroughs the medical-industrial complex touts out of fear if something is found, disaster will ensue. If this wasn’t true, then we should have no images like these in our country, but apparently, we do

Figure 1: This Took Seven Years, the Size of your Fist She was Putting Horse Urine on it to Heal it

Figure 2: Hid this from her Husband for Three Years
In less dramatic fashion we have forgotten women like well- known African-American journalist, Ananda Lewis, who died of metastatic breast cancer on June 11, 2025, probably because she was afraid of having a mammogram and the threat it portends [3]. So, while the rate of deaths from breast cancer is declining, the absolute number of deaths is increasing. Further, according to a report by MedStar Health found that, “A new survey from Med- Star Health finds that most American women over age 40 are not screening for breast cancer through annual mammogram. Accord- ing to the results, 59% of respondents say they forgo the recom- mended routine exam on a yearly basis. Almost a quarter (23%) say they’ve never had a mammogram. This in light of the fact that there is nearly a 3% increase in younger women under age 40 de- veloping breast cancer [4].”
Of course, in typical governmental fashion, the United States Preventative Task Force has now lowered the guidelines to start mammography at age 40. It was at 50 for many years. Then we have research findings by such a prestigious group as the American College of Surgeons Oncology Group in 2009 that African-Amer- ican women were developing a much more lethal breast cancer, so-called triple negative in their 30s What good is all this research then? In summary then, we apparently have (in MedStar survey) almost 60% of women over 40 refusing mammography guidelines, and 23% never had a mammogram [5]. African American wom- en develop an aggressive form of breast cancer in their 30s and the USPSTF is now lowering the guidelines to start at 40, where they had ratcheted it up to 50 for years. With increasing numbers of deaths, especially for African-American girls, what the hell is going on here, and who is in charge? Of course, no one is really in charge, we don’t have a true national focus charged to eliminate the suffering wrought by breast cancer.
What is going on is blatant disregard for women’s future by the medical-industrial complex. Fully 75% of America’s doctors are now ‘owned’ by either hospitals or HMOs, or worse, private equity firm’s hell bent on profit ahead of actual caring for our people. The new owners of our doctors tell them when they will see patients, how many they will see, and what type of treatment will be of- fered. Every decision that involves some expenditure of money is at the mercy of a ‘gatekeeper’ who decides if a request, for ex- ample, an MRI, will be done or refused. Forget what your doctor wants. And for-profit HMOs can divide the left-over money at the end of the year if there is a surplus. So, it seems like there is conflict of interest. If they don’t let you have that MRI or certain new ‘cancer’ treatment or that ‘miracle’ drug you see on TV, they potentially pocket that money.
They ignore the mounting disdain for those ‘fallow promises’ and the increasing yearly deaths from breast cancer, most of which could be avoided with The Lavender Way.
When doctors are essentially hourly employees and don’t have any say in how you are treated, this leads to a doctor who really doesn’t give a damn about you, especially since you’ll probably end up seeing multiple different doctors. That is, if you are lucky you’ll see a real doctor, otherwise you’ll see a PA (physician assistant) or NP (nurse practitioner). While the list of shameful intrusions into our being cared for the right way is endless, we will focus now on how we can reverse things. Usually going back in time is viewed as noncontributory. We remember the days when all physicians (after hours) had an answering service. The patient never got an answering machine that said we’re closed, please call back during regular business hours and ask for scheduling. Then you are lucky if it will only take a week to see your doctor, meanwhile your ap- pendix bursts and you need emergency surgery.
In my day even if a patient called at 2 am in some distress, the an- swering service would patch them through to me. Then a lasting disdain at your appointment is the doctor staring into the computer screen making sure they have the right codes for billing. Here’s how we fix things. And don’t say we don’t have the funding when we, via US AID, give a country like Guatemala $16,031,739 to develop a Sesame St. Workshop. That amount is small potatoes compared to the newly arrived 152 billion in tariffs enacted by President Trump. We just have to decide how important women are, and someone has to have the huevos to say enough is enough.
Methods
In order to totally revamp what we offer to America’s women in terms of diagnosis and treatment of breast cancer, we need to look past just treatment or what type of surgery they will incur. The ‘P” word will be paramount. In this case the ‘P” stands for PREVEN- TION. As a side bar and something not known to the public be- fore, when then, Dr. Bretz, authored the first largescale breast can- cer prevention clinical trial using the drug Tamoxifen, FDA IND 34,223, ICI (Imperial Chemical Industries now Astra-Zeneca’s) attorney told me there was a little saying going around the compa- ny since they had created a 7.5 mg ‘P’ pill and the ‘P’ ostensibly stood for Prevention. The joke was it stood for Phil. Then they could extend their patent but that never happened, 10 mg was the pill used for the first FDA approved breast cancer prevention pill.
To elucidate the anxiety and fear created just by picking up the phone to make an appointment for a mammogram, that causes the new term “Time Toxicity” developed by Arjun Gupta, MD [6]. At the outset of this paper we said we would have to dismantle the breast cancer Tower of Babel brick by brick, and that starts with the environment we create for women. That is before any diagno- sis, they should find themselves entering the facility, not out of fear but to embrace it. Further, they must know that the primary pur- pose and credo would be to preserve their mind, body, and spirit. We would advocate that the appearance of the waiting room, for instance, would be akin to entering a well-furnished home. Look book, Ashley Stiles In fact, a huge aquarium that they would walk under (in our flagship center) to get to the registration desk would have multiple inlets with tables to allow for solitude and contem- plation, or just hanging out [7]. Yes, this place will be so cool with a library and Lavender Bistro East women will want to hang out.

In addition, it would house a grand conference hall to be used not only for medical conferences the community could attend but con- certs or plays. Like everything there, the community could em- brace it. Below are images of the library and conference center.


Above is the entrance to the conference center and below the library and registration


Results
In our prior publications (listed in the Reference section), we have presented our 10 years out results. We have made it clear that with our genetics test it is possible to predict within ten years the onset of a patient’s breast cancer. This coupled with employing multiple non-radiation diagnostic modalities, thus being able to image a pa- tient accurately multiple times a year, we can find nascent cancers before they have attained the capacity to metastasize. Then using liquid nitrogen (aka The Lavender Procedure), we can kill the can- cer in-office in 20 minutes, totally outside the system for about $2,500.00 vs. around $200k for standard of care, including multi- ple surgeries usually for retained cancer at the margins, prolonged chemotherapy, and radiation.
Lavender would level the playing field overnight, especially the underserved. Briefly, we divided the patients into three groups. Group I were ideal patients, that is, ultrasmall cancers not likely to have metastasized and clear axillary lymph nodes on physical exam and ultrasound. Any lymph node over 1cm in size was sub- mitted to ultrasound guided core biopsy. Group 2 were patients with less-than-ideal cancers, for instance DCIS. Group 3 were pa- tients who had refused ANY standard-of-care. They generally had larger tumors that were done just to prevent the tumor from erod- ing through the skin. All patients in Group 1 at ten years out are cancer -free except two. One who had developed Alzheimer’s fell getting out of bed, hit her head and died as a consequence. The oth- er lived a great distance away and unbeknownst to us developed an aggressive primary lung cancer five years out, but no evidence of breast cancer. Our other papers have more details. We have shown the technology used in Lavender should be put to a definitive clin- ical trial against current standard-of-care.
Discussion
In addition to this thoughtfully designed National Flagship Breast facility, it would house three operating rooms, imaging center, a boutique hotel, training center, infusion center, pathology, radia- tion center, and research. Yes, if you haven’t guessed by now our country would dedicate this facility as the FLAGSHIP. Obviously, satellite facilities around the country (at least three in each state) would not be duplicated but as close as possible on a smaller scale. Since this is America, we would not advocate closing down the many breast facilities including those in the major cancer centers. Instead, we would just present an alternative and its entire struc- ture of what we feel women deserve. PROMISES MADE, PROM- ISES KEPT.
Other parameters of Lavender Breast Centers would include the following:
1. Same day appointments no matter what, even on weekends and after hours if need be.
2. All patients would undergo our genetics risk test that not only tells lifetime risk but when that risk will likely manifest within ten years of a patient’s life. Recommended.
3. Patients get to see the same doctor ideally for decades.
4. The doctor they see is the same doctor that can perform, for example, aspiration of a cyst or ultrasound guided core biopsy, or if needed, The Lavender Procedure (cryoablation).
5. No procedure (except definitive needle biopsy) will be carried out without full consultation and ample time for reflection with the other cancer doctors, oncologists and radiation therapists.
6. All centers would use state-of-the-art mammography with AI but, in addition, multiple non-radiation diagnostic modalities, in- cluding modified military infrared. We can use IR to enact acceler- ated imaging, something other centers just offering mammography can’t do because radiation is cumulative. That is, they can’t do accelerated mammography indefinitely because that may very well cause breast cancer. That’s why using multiple non-radiation diag- nostic modalities is so important.
7. Family members would be invited to observe the Lavender pro- cedure, thereby humanizing the entire experience.
8. No time limits on any visit. Bruce Carlson, the former Direc- tor of the Office of Reconnaissance, once said at a conference, “If you do things the same way, the results will always be the same.” In this paper we have presented something completely different than women being frightened just to make an appointment for mammography. It is our hope the President of the United States would one day tell America’s women his administration is going after breast cancer to end the suffering, whatever it takes, period. Lastly, it is not our intention to shove Lavender down everyone’s throat. We would expect that current Secretary of HHS RFK Jr. would impel a major definitive clinical trial between the technolo- gy of Lavender vs. standard-of-care. Let the best man win.
For completeness’ sake, for those who have not seen the infrared printout, below are a couple of examples. Our other papers explain it in detail.

This patient’s mother died of breast cancer at age 57 and the pa- tient is now 51. She said she went to bed every night wondering if today was the day she would develop breast cancer. Our genetics risk test said she was at high risk within ten years. We then imaged her twice yearly with our non-radiation diagnostic modalities, including our modified military infrared. As indicated above, it picked up the cancer in the right breast UOQ. The neural network with AI indicated positive. Our neural network compares the pa- tient’s heat signature with known heat signatures of various can- cers. As we enrolled various patients with cancer, the AI became more sensitive and thus more accurate in differentiating benign from malignant disease. In fact, our infrared picked up the cancer three years before mammography or MRI called it. Currently in- frared can’t localize within a couple of millimeters precisely where the cancer is, thus the need for mammography. Even so, this tumor was 4mm, our smallest found. Our first 500 patients we recorded a false negative rate of 0.4%.

This patient came in crying holding her mammogram report that identified suspicious calcifications for malignancy in the left breast at 6 0’clock. As can be seen all the heat signals are in the green, (except the threshold which is picking up the calcifications), and the comment section is clear. In the top left image, you can see the rose-colored circle at just the spot where the calcifications are. This case illustrates that infrared doesn’t need developed blood vessels (although that helps), but it can pick up cancers or not without neo-angiogenesis. It will register any metabolic activity irrespective of blood flow. This is a benign read. She left relieved and the biopsy showed dystrophic calcifications, non-malignant. A surgery was avoided.
This case was very interesting. As can be seen, all indications are cancer in the RUOQ, a very positive exam, except the images at the top did not show any flash point. The patient had a normal physi- cal exam, normal mammogram and normal ultrasound. Therefore, an MRI was ordered, and it picked up a cancer in the apex of the right lung. This cancer was asymptomatic and undiagnosed. Suc- cessful surgery saved her. This patient is one of four patients diag- nosed with other cancers besides breast that we have found. That is, one basal cell carcinoma, two patients with lymphoma (axillary lymph adenopathy), and this patient.
Conclusion
However, that isn’t enough to treat women in a totally different and non-threatening manner they deserve. They have put up with enough devastation, enough is enough. This country needs to demonstrate to ALL of America’s women that it is serious about ending the suffering wrought by breast cancer. To that end a signif- icant National Breast Cancer Center should be created akin to the one proposed herein. Its primary function would be to fine -tune diagnosis and treatment with the credo to preserve mind, body, and spirit. Breast cancer would be its primary focus. We learned certain things caring for over 14,000 women, not everything, but enough to know Lavender breast centers are the key they respond to. Without that center and satellites in each state, we’ll see the same scenario of slash-poison-burn. Saying again, women need to see something concrete. It is our hope this is brought to the attention of the President of the United States, and that he makes the announcement that would mean so much to so many and future generations [8-10].
Brick by Brick
Below is an image taken of a patient about two minutes after her Lavender procedure and normal activity is resumed immediately with one patient playing 18 holes of golf. This patient is now more than ten years out from her Lavender Procedure cancer-free, no surgery, no chemotherapy, and no radiation on a HER 2 positive cancer. The other patient’s surgery is obvious. A different out- come, you bet.
Below are two images. If it was you, which would you prefer?
Please refer to the reference section for our previously published papers. A couple more quotes from Dr. Raza’s book, The First Cell,’ are in order. “With minor variations, a protocol of surgery, chemotherapy, and radiation -- the slashpoison-burn approach to treating cancer – re- mains unchanged, it is an embarrassment. Equally embarrassing is the arrogant denial of that embarrassment.” Page 6 “Stay positive is the refrain, as if it were a sin to voice the intense pain and suffering of cancer patients. Why are we so afraid to tell the stories of the majority who die. “Page 7” The gaping discon- nect between knowledge about cancer biology and the capacity to use this knowledge to benefit patients is staggering.” Page 6 “How good are the solutions we offer if we constantly have to ask ourselves whether the cancer or the treatment will kill the patient.” Page 13 No one, however, willingly surrenders their pet projects, no matter how far they have drifted from the original intent, as long as they can maintain their grip on grants and power.” Page 46 Brick by Brick In closing, it’s really what the women say and not us. The letters below are a small sample but an important encapsulation of how we have affected women and learned from them in our 33 years as dedicated breast doctors. Our portfolio is almost 3” thick of mostly handwritten letters, not just a Hallmark card with a signature at the end. If you’re a fellow breast doctor, ask yourself how many let- ters you have received over the years because the patients were so grateful to be in your care. If your portfolio of letters is bigger than ours, we’d like to hear from you to make ourselves better. To really impact people, we found it more advantageous to be their friend than write papers about ‘significant P values’ and Kaplan-Meier Survival Curves. Check out these letters. If this isn’t what is star- ing you in the face every day, then perhaps you should stand a post and reconsider.

Brick by Brick

Brick by Brick
Brick by Brick
References
- Raza Azra, “The First Cell”, page 35.
- Shi, J., Yang, Y., Guo, Y., & Ren, W. (2022). Suicide risk among female breast cancer survivors: A population–based study. Frontiers in oncology, 12, 986822.
- Wikipedia under her name
- Most Women Skipping Annual Mammograms, According to New MedStar Health Survey, October 2, 2023, Media Inqui- ries.
- Sally, G. (2009). African American women still have poorer breast cancer outcomes. Journal of the Americn College of Surgeons.
- Gupta, A., Eisenhauer, E. A., & Booth, C. M. (2022). The time toxicity of cancer treatment. Journal of Clinical Oncology, 40(15), 1611-1615.
- Stiles, & Ashley. (2024). Lookbook for Lavender Breast Cen- ters.
- Bretz, et al, RAS Publishers, (2021). The Lavender Way – Lavender Procedure, a Way to Defeat Breast Cancer without Surgery, Chemotherapy, or Radiation. A Clarion Call for Rad- ical Change. Oncology and Therapy Journal, 2(2)
- Bretz, P., Mantik, D., & Lynch, R. (2024). The Lavender Way/ Procedure, How to Diagnose and Treat Early Breast Cancer without Surgery, Chemotherapy, or Radiation a Global Solu- tion-10 Year out Results. Gynecol Reprod Health. 2024; 8 (4): 1-8. Correspondence: Phillip Bretz, the Visionary Breast Cen- ter, La Quinta, California, USA, E-mail: phil. bretz@ gmail. com. Received, 16.
- Bretz, P., Mantik, D., Lynch, R., & Djordjevic, B. (2025). Treating Breast Cancer with the Breast Intact and the Patient Fully Awake, has a Lasting Positive Psychological Impact aka The Lavender Way – Lavender Procedure, Journal of Surgery, 13(3), 60-68.