
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Review Article - (2018) Volume 3, Issue 1
Wandering Spleen: A Rare Entity
Received Date: Nov 10, 2017 / Accepted Date: Nov 15, 2017 / Published Date: May 23, 2018
Copyright: ©Rita Mittal, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Wandering spleen is a rare differential diagnosis of an acute abdomen and must be suspected if a patient presents with abdominal pain along with a palpable lump and displacement of bowel to left upper quadrant and should be confirmed by CT scan.
As the condition is very rarely diagnosed pre-operatively, it requires a very high index of suspicion.
Introduction
As the condition is very rarely diagnosed pre-operatively, it requires a very high index of suspicion.
Case History
41 yrs old P2+0 admitted on 4th May, 2016 with chief complaints of - Heavy and frequent menstrual bleeding for 1year
-Awareness of lump per abdomen for 10-12days
-Pain lower abdomen & Burning micturation for 10-12days
• Her periods were dark red in colour with passage of clots. Cycles were repeated every 18-20days and there was no H/O dysmenorrhoea.
• Pain abdomen was dull aching, continuous, radiating to back and localised to lower abdomen and was relieved on lying down or after taking medication. There was burning micturation & increased frequency for 10-12days
• She also gave H/O awareness of lump per abdomen for 10-12 days which was painless, did not increase in size. She went to a private practitioner in Palampur and was referred to KNH as a case of fibroid uterus with adnexal mass after doing USG.
• No H/O altered bowel habits, evening rise of temperature, palpitations, loss of weight or appetite, inter menstrual bleeding or post coital bleeding
• There was nothing significant in past and family history. No abnormality was detected on GPE and Systemic Examination.
• On P/A Exam.- There was a well defined, firm, non tender mass of 16-18wks size arising from the pelvis, mainly in hypogastrium, mobile from side to side with no free fluid in the abdomen.
• Percussion note was dull and bowel sounds were normal
• L/E and P/S Exam. were normal
• P/V Exam. Mass of about 16 -18 wks size felt through anterior & Lt. fornix, firm, non tender, mobile from side to side. Uterus felt separately, parous size, firm, mobile, non tender, Right fornix clear
Clinical Impression
41yrs P 2+ O with Adnexal Mass ?
Ovarian Tumour
?? Subserous Fibroid
She was investigated for major surgery
Complete Haemogram
HB=9.8gm%
HCT=29.9%
TLC=13200/ml
DLC=N83 E2 L13
PLATLETS=4.10 Lac/ml
RFT
BUN=12.9mg/dl
S.UREA=1.0mg/dl
S. Creat- 0.8mg/dl
LFT: Normal
Electrolytes: Normal
CXR: WNL
ECG: WNL
CA125: 84.5U/L (normal range <35)
USG: ( 29/4/16) showed a mass of size 11.8x7.6cm, Slightly hyperechoic, appears to arise from fundal part of uterus, both ovaries normal
CT Scan: (30/4/16) Liver, GB, portal vein, CBD , pancreas, B/L kidneys: normal.Spleen – not visualized.Uterus - normal in size and shape, 4 x 4cm fibroid noted in the myometrium to the right of midline in the region of body of uterus. Adnexa : Large well defined soft tissue mass measuring 12 x 7x 8 cm noted in left side of pelvis extending superiorly upto umblical level.
Impression
? Subserosal fibroid
?? Solid ovarian mass
Management- Exploratory Laparotomy
Operative Findings
Evidence of dense adhesions. A reniform mass was lying anterior and to the left side of the uterus which was adherent to the surrounding structures i.e. Omentum, Bladder, Small and Large gut)
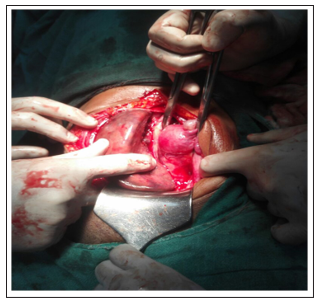
Figure 1: Finger showing adnexal mass with normal uterus,B/L tubes and ovaries.
Mass was reniform in shape, dull red in colour, firm in consistency, with a long vascular pedicle and showing e/o torsion. On following the pedicle it was found to be arising from the left hypochondrium.
A provisional diagnosis of Wandering Spleen was made.
Surgical opinion was sought. Meanwhile TAH with BSO was done
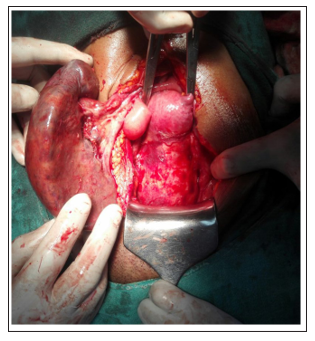
Figure 2: Arrow pointing towards long vascular pedicle of reniform mass
• On gross examination -Uterus normal in size, shape, outline. B/L fallopian tubes and ovaries were normal.
UCL 3 inches
On cut section
Uterus e/o polyp,2x2cm ,arising from fundus.
No e/o endometrial/ myometrial hyperplasia

Figure 3: Cut section of uterus showing myometrial polyp
• Spleen was enlarged, infarcted, with large pedicle 8-10 cm, containing thrombosed vessels and edematous tissue

Figure 4: Pancreatic tail extending into splenic pedicle identified,separated and divided.
Gut examined and found to be in satisfactory condition

Figure 5: Specimen of spleen after splenectomy
Recovery was uneventful and Pneumococcal vaccine given in addition to the routine treatment and she was discharged on 8th post op day.
HPE
Suggestive of splenic tissue with focal areas of infarction and thrombosis.Uterus, B/L tubes and ovaries: WNL with e/o myomatous polyp.
Introduction
Spleen is an important component of reticulo-endothelial system, which is involved in immunological defence and can serve as a storage site for red blood cells. Wandering spleen is a rare clinical entity with fewer than 500 cases reported and with an incidence of less than 0.2%.
Definition
Wandering spleen (WS) is defined as a mobile spleen that is attached only by an elongated vascular pedicle, allowing it to move to any part of the abdomen or pelvis.
Incidence
• More common in females with ratio of 7:1
• In children <10 years, ratio is 1:1
Usually presents between the ages of 20-40 years and in women of reproductive age group.
Review of Literature
Van Horn, a Dutch Physician, is credited with describing this condition in 1667 after performing an autopsy.
In 1875, Martin, a German Obstetrician, performed the first splenectomy for a wandering spleen.
Ten years later, splenopexy was described and was considered superior to splenectomy.
Embryology
Fetal splenic tissue develops from condensations of mesoderm in the dorsal mesogastrium. This peritoneal fold attaches the dorsal body wall to the fusiform swelling in the foregut that develops into the stomach. This condensation divides the mesogastrium into two parts, one between fetal splenic tissue and stomach to form gastrosplenic ligament and the other between it and the left kidney to form lienorenal ligament.
Anatomy
It lies in the left hypochondrium between the gastric fundus and the left hemidiaphragm, with its long axis lying along the tenth rib. The hilum sets in the angle between the stomach and the kidney and is in contact with the tail of the pancreas. The concave visceral surface lies in contact with these structures, and the lower pole extends upto the mid-axillary line.
Aetiology
Wandering spleen is a rare entity in which the spleen is attached by a long, vascular pedicle and is without its usual peritoneal attachments. The spleen can be found on any part of the abdomen or pelvis because of the length of its pedicle. The variable incidence of wandering spleen according to age and sex can be explained by two possible aetiologies, which are congenital and acquired.
• The acquired form occurs in multiparous women as a result of hormonal changes during pregnancy. This causes a slackening of the abdominal wall and laxity of the ligaments normally attached to the spleen.
• In the congenital form, there is failure of normal development of the dorsal mesogastrium when the lesser sac is formed. The attachment of the dorsal mesentery to the posterior peritoneum and diaphragm is faulty
Suspensory ligament of the spleen is either not formed or only partially formed. The length of its vascular pedicle determines mobility of the spleen in the absence of either some or all of these ligaments. Some reports suggest that wandering spleen is a result of progressive splenomegaly due to diseases such as typhoid fever, lymphoma and especially malaria. This is unlikely because some wandering spleens are found to be of normal size or only moderately enlarged. A more likely explanation is that splenomegaly is secondary to chronic or recurrent torsion and subsequent venous congestion, not the primary disease process.
Clinical Presentation
Varied and the diagnosis is often elusive. Wandering spleen usually presents as asymptomatic abdominal mass, intermittent abdominal pain or acute abdomen.
Sixty percent have a mass and pain. The nature of the pain reflects the degree of vascular occlusion and ischemia to the splenic pedicle. Acute torsion may precipitate fever, vomiting and acute abdominal pain, while recurrent, chronic torsion and detorsion may present as intermittent colicky pain or vague abdominal discomfort. Torsion can be precipitated by any movements of the body, changes in intra-abdominal pressure during respiration or peristalsis or distention of adjacent organs.
• Acute pancreatitis may be associated due to incorporation of the tail of the pancreas in the spleen’s vascular pedicle.
• Gastric compression or distention may also occur
• On physical examination, patients with wandering spleen may present with a pelvic or abdominal mass that may or may not be associated with pain or tenderness.
• Physical findings vary with the path physiologic state of the spleen.
The triad of
1. A firm ovoid mass with a notched edge
2. Painful movement of the mass except when the mass is moved toward the left upper quadrant
3. Resonance to percussion in the left upper quadrant has been described to suggest the diagnosis of a wandering spleen
Common differential diagnosis are
1. tubo-ovarian abscess
2. ovarian cyst with torsion
3. uterine fibroid
4. extrauterine pregnancy
• Laboratory values are often non-specific, however leucocytosis is generally present.
• Diagnosis of wandering spleen is very difficult with physical exam. alone and often requires radiologic confirmation.
Radiological Findings
Conventional radiographs of the abdomen may demonstrate distended bowel loops and suggest a soft-tissue mass. Small-bowel loops in the left upper quadrant can be suggestive of a wandering spleen.
The most reliable and least invasive method of making the diagnosis is with ultrasonography which can demonstrate the morphology and homogeneous echo texture of the spleen and its absence from its normal position in the left upper abdomen (as in this case). Excessive gas within the bowel may obscure this finding. If the spleen’s absence from the left upper quadrant has been confirmed, then evaluation of the vascular pedicle with Doppler studies may confirm decreased or absent blood flow to the ectopically located spleen that has undergone torsion.
• Radionuclide imaging complements ultrasonography and Liver-spleen scans utilizing technetium 99Tcm-sulphur colloid may demonstrate splenic displacement as well as the functional state of the spleen.
• 51 Cr-tagged red cells are more specific and can prevent confusion with the left lobe of the liver.
• CT contrast imaging is preferred mode of investigation with the contrast helping to elucidate the viability of spleen. If significant torsion of the splenic pedicle occurs, the torsed pedicle may mimic a bowel intussusceptions in appearance. The most specific sign of splenic torsion is a “whirl-like” (or ‘whorled’) appearance of splenic vessels and surrounding fat usually noted at the splenic hilum. Occasionally, ascites or necrosis of the pancreatic tail can be seen.
• If torsion is chronic, a thick pseudo capsule is evident. The spleen is not enhanced by intravenous contrast medium if torsion has occurred and blood supply is lost
• Arteriography allows definitive evaluation of the splenic vasculature and signs of left-sided portal hypertension, if present.
• Treatment: - Definitive treatment for wandering spleen is operative, since nonoperative treatment is associated with a complication rate as high as 65%.
Complications of wandering spleen include:
1. Infarction
2. Gangrene
3. Splenic abscess,
4. Variceal haemorrhage and
5. Pancreatic necrosis Historically, splenectomy has been used for wandering spleen, but with increased understanding of the spleen’s function, splenopexy with splenic salvage is now the procedure of choice in children. However, the decision to perform splenopexy versus splenectomy depends on both the timing of clinical presentation and the appearance and viability of the spleen intraoperatively
In the emergent setting, the diagnosis of wandering spleen is usually made at laparotomy because patients present with an acute abdomen.
The decision to perform splenopexy or splenectomy depends on the viability of the spleen after detorsion. If the spleen appears infarcted, a splenectomy should be performed. Splenopexy is a reasonable option when the spleen appears viable after detorsion and the splenic vein is not thrombosed. Results of splenopexy are considered better
References
- Sharma A, Salerno G.A (2014) torted wandering spleen: a case report. Journal of Medical Case Reports 8: 133.
- Lahiri S, Dasgupta N, Mondal A (2010) Journal of Surgical Case Reports 10: 4.
- Dahiya N, Karthikeyan D, Vijay S, Kumar T, Vaid M (2002) Wandering spleen:Unusual presentation and course of events. Abdominal Imaging 12: 359-362.
- Chi Long Ho (2014) Wandering spleen with chronic torsion in apatient with thalassaemia.Singapore Medical Journal 5: 198-200.
- Goyal RB, Gupta R, Prabhakar G, Mathur P, Mala T (2014) Salvage splenopexy for torsion of wandering spleen in a child. APSP J Case Rep 5: 4.
- Ahmadi H, Tehrani MM (2016) Arare caseofsplenic torsion with sigmoid volvulus in a 14 year old girl. Acta Med Iran 54: 72-75.
- Yoldas O, Karabusa T, Ozsan I, sahin E, Limon O et al (2015) Laparoscopic splenectomy for a wandering spleen causing chronic pelvic pain. Ulus Cerrahi Derg 32: 292-294.
- MOHAMMADI A, Mohammad GR (2015) Wandering Spleen: Whirlpool Appearance in Color Doppler Ultrasonography. A Case Report. MAEdiCA.a Journal of Clinical Medicine 10: 58-60.