
Advances in Hematology and Oncology Research(AHOR)
ISSN: 2692-5516 | DOI: 10.33140/AHOR
Impact Factor: 1.2


Case Report - (2025) Volume 8, Issue 2
Unusual Presentation of a Rare Case of Breast Dermatofibrosarcoma Protuberans in a Young Male: A Case Report and Literature Review
2Department of Surgery, King Abdulaziz Hospital, Saudi Arabia
3Department of Pathology and Laboratory Medicine, King Faisal Specialist Hospital and Research Centre, Saudi Arabia
Received Date: Jun 13, 2025 / Accepted Date: Jul 28, 2025 / Published Date: Aug 05, 2025
Copyright: ©Â©2025 Wadha Almohamdi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Almohamdi, W., Alghamdi, R., Mandili, A., Rafi, R., Almutawa, A., et, al. (2025). Unusual Presentation of a Rare Case of Breast Dermatofibrosarcoma Protuberans in a Young Male: A Case Report and Literature Review. Adv Hema Onco Res, 8(2), 01-06.
Abstract
Introduction: Dermatofibrosarcoma protuberans is an extremely rare subtype of soft tissue neoplasm. Although DFSP typically manifests in the trunk and extremities, it rarely occurs in the breast, and is often misdiagnosed as benign or malignant breast lesions. Data regarding DFSP in the breast is scarce in existing literature. Only 13 cases in men have been documented. Here, we present a case diagnosed with breast DFSP in a young male patient who underwent surgical excision at our facility.
Case Report: A 24 years old male patient presented to the surgical clinic complaining of painless right breast lump for 8 months. The patient denied any nipple discharge. No history of hormonal or steroids medications use. Upon examination there was non-tender 1cm mass felt at lower outer quadrant of the right breast, with no changes in the overlying skin. At the contralateral side, the left breast was normal. Bilateral axilla was unremarkable.
Discussion: Dermatofibrosarcoma was first described as progressive recurrent dermatofibroma in 1924 by Darier and Ferrand. Subsequently, in 1925 Hoffmann referred to the disease as dermatofibrosarcoma protuberans DFSP.
Conclusion: Dermato Fibrosarcoma Protuberans (DFSP) of the breast is extremely rare. We reported a rare case of breast DFSP in a male patient discovered after 8 months with unusual presentation as a breast lump and not a skin lesion, with nonspecific radiological features. Due to the rarity of breast DFSP cases, surgeons need to be aware of breast DFSP to avoid misdiagnosis with a benign breast lesion and keep a high index of suspicion in male breast lesions.
Keywords
Dermatofibrosarcoma Protuberans, Breast Sarcoma, Breast Tumors, Spindle Cell Tumors, Male Breast, Case Report
Introduction
Dermatofibrosarcoma protuberans is an extremely rare subtype of soft tissue neoplasm. Although DFSP typically manifests in the trunk and extremities, it rarely occurs in the breast, and is often misdiagnosed as benign or malignant breast lesions. Data regarding DFSP in the breast is scarce in existing literature. Only 13 cases in men have been documented. Here, we present a case diagnosed with breast DFSP in a young male patient who underwent surgical excision at our facility. In addition to presenting this unique case, we also conducted a literature review to draw attention to breast DFSP. Currently, there is a lack of reported studies exploring the cause of breast DSFP, the clinical, and radiological features, and the response to surgical treatment.
Case Report
A 24 years old male patient presented to the surgical clinic complaining of painless right breast lump for 8 months. The patient denied any nipple discharge. No history of hormonal or steroids medications use. Upon examination there was non-tender 1cm mass felt at lower outer quadrant of the right breast, with no changes in the overlying skin. At the contralateral side, the left breast was normal. Bilateral axilla was unremarkable. The patienthad right breast ultrasound that showed a 1.7cm well-defined oval shaped heterogenous soft tissue solid mass with internal vascularity. BIRADS 4. US-guided biopsy showed features of DFSP, and tumor cells were positive for CD34 marker and negative for epithelial markers (Cytokeratins Cam 5.2 and Pankeratin). The patient had Magnetic Resonance Imaging (MRI) which revealed a well-defined oval mass, showing early homogenous persistent enhancement, and measuring 1.6 x 1.2 x 1.7 cm. The case was discussed in the breast tumor board, and the plan was to proceed with wide local excision. The patient underwent right breast lumpectomy. Preoperative image of the tumor with 2 cm margins marked (Figure 1). Intraoperative image showed nodular appearance of the lesion (Figure 2).

Figure 1: Preoperative Image of the Tumor with 2 cm Margins Marked
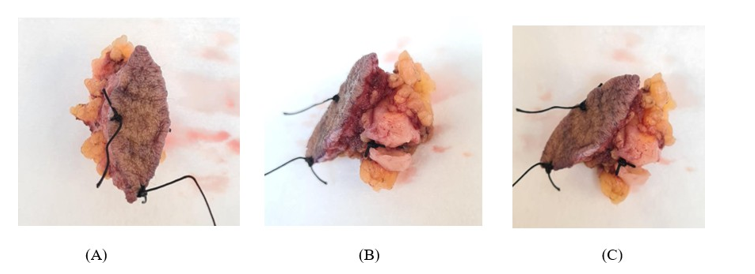
Figure 2: (A) Intraoperative Image of the Tumor after WLE, (B) Nodular Appearance of the Lesion and the Cut Surface (C) With Infiltrating Growth at the Periphery
Pathologic examination of the excised mass revealed a relatively well-defined tumor nodule within the subcutaneous fat (Figure 3A and 3B). The proliferating tumor cells exhibited a uniform spindle cell morphology, with a prominent storiform growth pattern (Figure 4). There was no significant mitotic activity or necrosis. The tumor involved the fat (adipocytes) in a honeycomb-like pattern (Figure 4). Immunohistochemistry study revealed strong and diffuse positivity for CD34 marker in the tumor cells (Figure 5 and 6). S-100 marker was negative (which would argue against the potential histologic differential diagnosis of the rare and recently defined NTRK-rearranged spindle cell neoplasm (some cases of which can have a DFSP-like histologic features). No fibro sarcomatous transformation was noted.


Figure 3 (A, B): Low-Magnification Photomicrograph, Illustrating the Upper Edge of the Lesion (Left Lower Field in A and Right Lower Filed in B) Within the Subcutaneous Fat. Part of Epidermis is seen in the Right Upper Corner (A) while Skin Adnexa (A Hair Follicle and Sweat Glands) are seen in the Left Upper Filed (B). (H&E Stain; Original Magnification 20x)
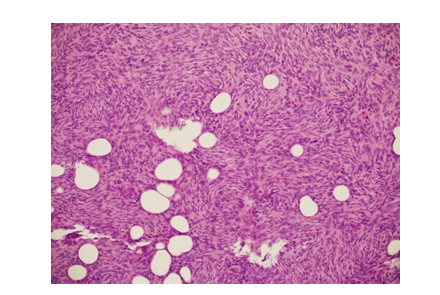
Figure 4: The Proliferating Tumor Cells, Exhibiting a Uniform Spindle Cell Morphology, with a Storiform Growth Pattern, and Entrapment of Adipocytes in a Honeycomb-Like Pattern. (H&E Stain; Original Magnification 200x)
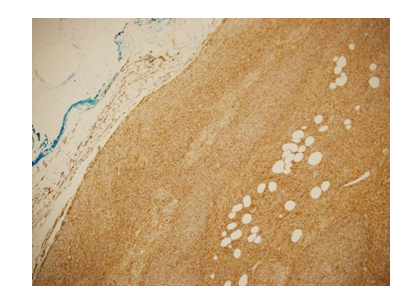
Figure 5: Immunohistochemistry for CD34 Marker, showing Strong and Diffuse Positivity (Brown Color) in the Tumor Cells (Central and Right Field). (Original Magnification 100x)

Figure 6: Low-Magnification Photomicrograph Showing the Smooth and Well-Define Border of the Lesion within the Subcutaneous Fat. Fatty Tissue is Noted involved by the Tumor. (H&E Stain; Original Magnification 50x)
As the peripheral and deep margins were focally involved, and in order to minimize the chance of local recurrence, the case was referred to plastic surgery service for considering a wide re-excision and immediate breast reconstruction. Plastic surgery assessment revealed scar only, with no evidence of local palpable residual mass, so their plan was observation only and follow up. During follow-up, wound has healed completely with no locoregional recurrence or distant metastasis after 2 years.
Discussion
Dermatofibrosarcoma was first described as progressive recurrent dermatofibroma in 1924 by Darier and Ferrand. Subsequently, in 1925 Hoffmann referred to the disease as dermatofibrosarcoma protuberans DFSP [1]. DFSP of the breast is an exceedingly rare condition with an unknown cause. It is characterized by a slow- growing mesenchymal tumor that usually originates in the dermis [2-3]. It is most commonly encountered between the ages of 30 and 50 [4]. In one study by Bouhani M et al, reported only 11 cases of breast DFSP in men from 1994 until 2019 [5]. We continued the review based on the PubMed and Google Scholar database to search for similar cases, and we found two more cases reported as DFSP of the breast in the last 4 years from 2020 until 2023 (Table). Our literature review revealed the median age of presentation is 41 years, youngest was 9 years and oldest was 66 years.
|
Case |
Author |
Years |
Age |
|
1 |
Chen et al [6] |
2009 |
41 |
|
2 |
Park et al [7] |
2011 |
36 |
|
3 |
Akhtar et al [8] |
2012 |
22 |
|
4 |
Prabhu et al [9] |
2014 |
55 |
|
5 |
Al Tarakji et al [10] |
2015 |
27 |
|
6 |
Saikia et al [11] |
2016 |
40 |
|
7 |
Ezejiofor et al [12] |
2017 |
13 |
|
8 |
Diwakar et al [13] |
2018 |
35 |
|
9 |
Dhakal et al [14] |
2018 |
48 |
|
10 |
Bouhani et al [5] |
2019 |
44 |
|
11 |
Murase et al [15] |
2020 |
9 |
|
12 |
Wang et al [16] |
2020 |
27 |
|
13 |
VuÄaj et al [17] |
2021 |
66 |
|
14 |
Current case |
2024 |
24 |
Table: Case Reported of breast DFSP in Male Patients on PubMed and Google Scholar
Incidence of DFSP is around 1% of all soft tissue tumors and less than 0.1% of all malignancies [18]. It most commonly occurs in the trunk and extremities, and is extremely rare to affect the breast [19]. There are two major types of DFSP have been described: the classic DFSP “low-grade” type, and the fibro sarcomatous “high- grade” type FS-DFSP. Classic type represents around 85% of cases, and is considered a tumor of intermediate grade (borderline malignancy), with a substantial risk of local recurrence (20-50%), particularly if not completely excised, and generally lack metastatic potential. Approximately 10% of cases represent the high-grade (Fibro sarcomatous) type, which is more aggressive and associated with higher rates of recurrence and metastasis, with up to 10-15% risk of metastasis (most often to the lung) [20].
Radiological investigations of breast DFSP still has no specific features and can be misdiagnosed for other benign and malignant breast lesions. On breast ultrasound the major characteristic of the DFSP is probably the hyperechoic rim in the periphery which reflects the components of the tumor cells and fibrous tissue invading the fat in the subcutaneous layer. For better evaluation for the DFSP margins, infiltrating into surrounding tissue and invading the adjacent structures, MRI is the preferred modality [21]. As radiological modalities still lack diagnostic features for breast DFSP, core needle biopsy or even an excisional biopsy is required to establish the diagnosis. Histopathologically, the tumor is composed of monomorphic population of spindle cells arranged in a storiform pattern. The intense staining for CD34 marker differentiates DFSP from myxoid liposarcoma [10]. The vast majority of DFSP contain fusion genes of COL1A1-PDGFB, but rare ones (around 2%), particularly those occurring the breast/ chest wall, do have PDGFD fusion gene.
Due to common presentation and lack of diagnostic radiological features; breast DFSP has wide differential diagnosis, including benign and malignant breast diseases which includes primary breast tumors with spindle cell differentiation like phyllodes tumor, fibromatosis-like areas of metaplastic carcinoma, fibromatosis, nodular fasciitis, and inflammatory myofibroblastic tumor [8]. In our case, initially our provisional diagnosis was breast fibroadenoma as it presented as a breast lump and not as skin lesion, but histopathological examination showed DFSP. The etiology is not completely clear. Multiple factors have been suggested including previous trauma in around 10-20% of the cases, scars, burns, tattoos, and vaccination scar [5]. In our case, the patient had no previous scar or trauma history. Radiological investigations of breast DFSP still has no specific features and can be misdiagnosed for other benign and malignant breast lesions. On breast ultrasound the major characteristic of the DFSP is probably the hyperechoic rim in the periphery which reflects the components of the tumor cells and fibrous tissue invading the fat in the subcutaneous layer. For better evaluation for the DFSP margins, infiltrating into surrounding tissue and invading the adjacent structures, MRI is the preferred modality [21]. As radiological modalities still lack diagnostic features for breast DFSP, core needle biopsy or even an excisional biopsy is required to establish the diagnosis. Histopathologically, the tumor is composed of monomorphic population of spindle cells arranged in a storiform pattern. The intense staining for CD34 marker differentiates DFSP from myxoid liposarcoma [10]. The vast majority of DFSP contain fusion genes of COL1A1-PDGFB, but rare ones (around 2%), particularly those occurring the breast/chest wall, do have PDGFD fusion gene.
Due to common presentation and lack of diagnostic radiological features; breast DFSP has wide differential diagnosis, including benign and malignant breast diseases which includes primary breast tumors with spindle cell differentiation like phyllodes tumor, fibromatosis-like areas of metaplastic carcinoma, fibromatosis, nodular fasciitis, and inflammatory myofibroblastic tumor [8]. In our case, initially our provisional diagnosis was breast fibroadenoma as it presented as a breast lump and not as skin lesion, but histopathological examination showed DFSP. The etiology is not completely clear. Multiple factors have been suggested including previous trauma in around 10-20% of the cases, scars, burns, tattoos, and vaccination scar [5]. In our case, the patient had no previous scar or trauma history. Surgical wide local excision with free margin is the cornerstone management. DFSPs are resistant to chemoradiotherapy. The exact margin of resection is still unknown because DFSP has a high propensity for local infiltration as well as a high local recurrence rate. an excision with 2-3 cm margin with skin, subcutaneous tissue, and fascia included is widely accepted [5]. Mohs Micrographic Surgery MMS is another option; it allows the extent of excision to be customized to the microscopic extent of tumor and results in better margin control [13]. Because of the overexpression of PDGFB leads to activation of the PDGF receptors, tyrosine kinase inhibitors (Imatinib) can be used as an immunotherapy when clinically appropriate. Post operatively, patients need be seen regularly every 6-12 months to detect early recurrence. Radiological investigation, including ultrasound, and tissue biopsy are only indicated in cases of suspected recurrence. The 10-year survival rate is >99% [22].
Conclusion
Dermato Fibrosarcoma Protuberans (DFSP) of the breast is extremely rare. We reported a rare case of breast DFSP in a male patient discovered after 8 months with unusual presentation as a breast lump and not a skin lesion, with nonspecific radiological features. Due to the rarity of breast DFSP cases, surgeons need to be aware of breast DFSP to avoid misdiagnosis with a benign breast lesion and keep a high index of suspicion in male breast lesions.
Data Availability Statement
The data that support the fndings of this study are available and included in the article/supporting material/referenced article.
Ethics statement
There is no identifable information on the patient.
Consent
The data for the patient were obtained from the hospital’s electronic system.
References
- Cottier, O., Fiche, M., Meuwly, J. Y., & Delaloye¹, J. F. (2011). Dermatofibrosarcoma presenting as a nodule in the breast of a 75-year-old woman: a case report. Journal of medical case reports, 5(1), 503.
- Maji, S., Paul, M. J., & Sen, S. (2018). Dermatofibrosarcomaprotuberans of the breast—a rare entity. Indian Journal ofSurgical Oncology, 9(3), 351-354.
- Bague, S., & Folpe, A. L. (2008). Dermatofibrosarcoma protuberans presenting as a subcutaneous mass: a clinicopathological study of 15 cases with exclusive or near- exclusive subcutaneous involvement. The American journal of dermatopathology, 30(4), 327-332.
- Boukovalas, S., Castillo, A. C., Andry, D., Lombana, N., Qiu, S., & Murphy, K. D. (2017). Dermatofibrosarcoma protuberans: trauma and genetics. Ann Plast Reconstr Surg, 1(1), 1001.
- Bouhani, M., Fertani, Y., Zemni, I., Adouni, O., Bouida, A., Chargui, R., & Khaled, R. (2019). Dermatofibrosarcoma protuberans of the breast in man: an extremely rare entity with a review of the literature. Journal of Investigative Medicine High Impact Case Reports, 7, 2324709619875634.
- Chen, X., Chen, Y. H., Zhang, Y. L., Guo, Y. M., Bai,Z. L., & Zhao, X. (2009). Magnetic resonance imaging and mammographic appearance of dermatofibrosarcoma protuberans in a male breast: a case report and literature review. Journal of medical case reports, 3(1), 8246.
- PARK, J. Y., JANG, Y. H., & KIM, Y. C. (2011). Subcutaneousdermatofibrosarcoma protuberans on the breast. Korean Journal of Dermatology, 1025-1027.
- Akhtar, K., Sherwani, R. K., & Ray, P. S. (2012). Dermatofibrosarcoma protuberans of male breast: an unusual presentation. Oman medical journal, 27(4), e038.
- Prabhu, V. V., Shivani, A., Kulkarni, S. H., & Pawar,V. R. (2014). Dermatofibrosarcoma protuberans: male breast. Medical Journal of Dr. DY Patil Vidyapeeth, 7(1), 85- 87.
- Al Tarakji, M., Toro, A., Di Carlo, I., & Junejo, K. (2015). Unusual presentation of dermatofibrosarcoma protuberans in a male patient’s breast: a case report and review of the literature. World journal of surgical oncology, 13(1), 158.
- Saikia, B. K., Das, I., & Mandal, G. K. (2016). Fibrosarcomatous change in the background of dermatofibrosarcoma protuberans in male breast: study of a rare case and review of the entity. Journal of mid-life health, 7(1), 45-48.
- Ezejiofor, I. F., Onwukamuche, M. E., Anyiam, D. C. D., Ugwu, J. O., Ndukwe, C. O., Madubuike, K. C., ... & Ozor,N. S. (2017). Breast dermatofibrosarcoma protuberans in an adolescent male: a case report and extensive review of theliterature. Trop J Med Res, 20(2), 204-207.
- Diwakar, D. K., Wadhwani, N., & Paruthi, S. (2018). Recurrent dermatofibrosarcoma protuberans: challenging a surgeon’s dexterity for the ‘tricky’margins. Ecancermedicalscience, 12, 858.
- Dhakal, R., Makaju, R., Makaju, S., & Shrestha, G. (2018). Dermatofibrosarcoma protuberans of male breast: a case report. Int Clin Pathol J, 6(4), 154-156.
- Murase, Y., Takeichi, T., Matsumoto, T., Sakakibara, A., & Akiyama, M. (2020). A juvenile male case of dermatofibrosarcoma protuberans on the breast. Clinical & Experimental Dermatology, 45(1).
- Wang, Y., Wang, Y., Chen, R., Tang, Z., & Liu, S. (2020). A rare malignant disease, dermatofibrosarcoma protuberans of the breast: a retrospective analysis and review of literature. BioMed Research International, 2020(1), 8852182.
- Vucaj-cirilovic, V., Vukovic, M., Boban, J., Šolajic, N., Ranisavljevic, M., & Prvulovic-Bunovic, N. (2021). A male case of dermatofibrosarcoma protuberans in the breast presenting as gynecomastia. Vojnosanitetski pregled, 78(10), 1108-1112.
- Rouhani, P., Fletcher, C. D., Devesa, S. S., & Toro, J. R. (2008). Cutaneous soft tissue sarcoma incidence patterns in the US: an analysis of 12,114 cases. Cancer: Interdisciplinary International Journal of the American Cancer Society, 113(3), 616-627.
- Al Barwani, A. S., Taif, S., Al Mazrouai, R. A., Al Muzahmi,K. S., & Alrawi, A. (2016). Dermatofibrosarcoma protuberans: insights into a rare soft tissue tumor. Journal of Clinical Imaging Science, 6, 16.
- Bowne, W. B., Antonescu, C. R., Leung, D. H., Katz, S. C.,Hawkins, W. G., Woodruff, J. M., ... & Lewis, J. J. (2000). Dermatofibrosarcoma protuberans: a clinicopathologic analysis of patients treated and followed at a single institution. Cancer, 88(12), 2711-2720.
- Bae, S. H., & Lee, J. Y. (2016). Imaging features of breast dermatofibrosarcoma protuberans in various modalities including FDG-PET CT. Iranian Journal of Radiology, 13(2), e33916.
- Chan,T.C.,Wu,C.J.,&Jeng,S.F.(2015).Dermatofibrosarcoma protuberans: A 10-year experience. Formosan Journal of Surgery, 48(1), 10-16.