
International Journal of Orthopaedics Research(IJOR)
ISSN: 2690-9189 | DOI: 10.33140/IJOR
Impact Factor: 1.6

Research Article - (2025) Volume 8, Issue 2
Unilateral Cementless Total Knee Arthroplasty: Approach and Clinical Outcomes
2Bacharel em Medicina, Clinica Arthron - Rua Treze de Maio, Brazil
Received Date: Feb 26, 2025 / Accepted Date: Mar 26, 2025 / Published Date: Apr 04, 2025
Copyright: ©2025 Marcelo Horikawa, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Horikawa, M., Barbieri Horikawa, P. H. (2025). Unilateral Cementless Total Knee Arthroplasty: Approach and Clinical Outcomes. Int J Ortho Res, 8(2), 01-09.
Abstract
Objective: This study aims to analyze the clinical and functional outcomes of unilateral cementless total knee arthroplasty (TKA), evaluating its efficacy, safety, and impact on patient recovery. Additionally, this research compares cementless TKA with the conventional cemented approach, highlighting advantages, disadvantages, and potential complications associated with each technique.
Methods: A retrospective cohort study was conducted on 280 patients who underwent unilateral cementless TKA. Demographic data, comorbidities, and biomechanical parameters were analyzed. Femoral and tibial movements were assessed through radiographic measurements, and functional outcomes were evaluated using clinical scores. Statistical analysis included the Shapiro-Wilk test for normality, the Kruskal-Wallis test for intergroup comparisons, and Dunn’s post-hoc test for pairwise differences. Statistical significance was set at p < 0.05.
Results: Statistically significant differences were found in key biomechanical parameters, particularly in femoral slope (2.10° ± 1.35, p = 0.007), tibial flexion (4.40° ± 2.20, p = 0.009), and tibial extension (2.30° ± 1.60, p = 0.038). These results suggest that cementless TKA requires precise implant positioning to optimize sagittal alignment and post- operative function. Gender distribution showed a predominance of female patients (60.71%), and hypertension was the most prevalent comorbidity (68.93%), reinforcing the need for perioperative cardiovascular risk management. No statistically significant differences were found in tibial varus, tibial valgus, or rotational movements.
Conclusion: The findings support the efficacy and safety of cementless TKA, particularly in younger and active patients with good bone quality. Precise implant positioning is essential to minimize post-operative complications and ensure long-term survivorship. Compared to cemented TKA, cementless fixation presents advantages such as improved osseointegration and reduced cement-related complications but also requires careful patient selection to mitigate the risk of early implant loosening. Future studies should focus on long-term implant survival, functional recovery, and cost- effectiveness to further refine the indications for cementless TKA.
Keywords
Cementless Total Knee Arthroplasty, Knee Osteoarthritis, Biomechanics, Implant Fixation, Surgical Outcomes
Introduction
Total knee arthroplasty (TKA) is one of the most commonly performed surgical procedures for patients suffering from end- stage knee osteoarthritis (OA). It is a highly effective intervention aimed at relieving pain, improving function, and restoring joint stability [1,2]. Over the past few decades, advancements in implant materials, fixation techniques, and surgical precision have significantly improved the clinical outcomes of TKA. However, the debate regarding the optimal fixation method—cemented versus cementless—remains ongoing, as both approaches present distinct advantages and challenges [3, 4].
standard, with long-term studies demonstrating excellent implant survivorship and predictable outcomes [5,6]. By utilizing polymethylmethacrylate (PMMA) cement to anchor the implant to the bone, cemented fixation provides immediate stability and reliable long-term performance [7,8]. Despite these advantages, cemented implants are associated with complications such as aseptic loosening, periprosthetic fractures, and bone cement implantation syndrome, leading some surgeons to explore alternative fixation methods [9,10].
In contrast, cementless TKA has gained popularity due to its potential for biological fixation and long-term durability [11,12]. Unlike cemented implants, cementless components rely on bone ingrowth to achieve stability, reducing concerns related to cement wear debris, osteolysis, and late-stage loosening [13,14]. Advances in implant coatings, such as porous titanium and hydroxyapatite, have improved bone-implant integration, making cementless TKA a promising option for younger, active patients [15,16].
Despite its advantages, cementless fixation presents specific challenges. One of the primary concerns is early aseptic loosening, particularly in patients with osteoporosis or poor bone stock [17,18]. Additionally, subsidence of tibial components has been reported in certain patient populations, potentially leading to malalignment and compromised functional outcomes [19,20]. Given these risks, proper patient selection is crucial to maximize the benefits of cementless TKA while minimizing complications [21,22].
Beyond fixation techniques, several patient-specific factors influence surgical outcomes. Age, activity level, bone quality, and the presence of comorbidities all play essential roles in determining the most appropriate approach for each individual [23,24]. Recent studies indicate that hypertension, diabetes, and rheumatoid arthritis are among the most frequently observed comorbidities in TKA patients, impacting perioperative risks, rehabilitation efficiency, and long-term implant survivorship [25,26]. Given the increasing prevalence of multimorbidity in aging populations, optimizing perioperative care is essential for reducing complications and enhancing recovery [5,27].
Another critical factor influencing TKA outcomes is gender differences. Studies have shown that women undergo TKA at higher rates than men, often presenting with greater preoperative pain and functional limitations [14,28]. Anatomical and hormonal differences, including variations in knee kinematics, joint laxity, and bone density, may contribute to distinct surgical considerations for female versus male patients [10,13]. Understanding these differences is vital for tailoring surgical techniques, implant selection, and rehabilitation protocols to ensure optimal outcomes for all patient demographics [15,21].
In addition to biological and demographic factors, technological advancements in knee arthroplasty have the potential to improve alignment precision and implant positioning, thereby enhancing patient outcomes [8,26]. Robotic-assisted TKA and patient- specific instrumentation (PSI) have gained popularity for their ability to optimize component alignment and reduce surgical variability [9,23]. However, while these technologies have demonstrated promising short-term benefits, their long-term cost- effectiveness and superiority over conventional techniques remain under investigation [14,20].
As the field of knee arthroplasty continues to evolve, surgeons must weigh the benefits and drawbacks of each fixation method to provide the best possible outcomes for patients. While cemented TKA remains the preferred choice for older, lower-demand patients, cementless TKA is emerging as a viable alternative, particularly for younger and more active individuals [16,24]. The decision should be highly individualized, considering patient- specific characteristics, surgical expertise, and implant innovations [13,21].
This study aims to analyze the clinical and functional outcomes of unilateral cementless total knee arthroplasty (TKA), evaluating its efficacy, safety, and impact on patient recovery. Additionally, this research seeks to compare cementless TKA with the conventional cemented approach, highlighting advantages, disadvantages, and potential complications associated with each technique. By assessing biomechanical parameters, patient-reported outcomes, and implant survivorship, this study contributes to the ongoing discussion regarding the optimal fixation method in modern knee arthroplasty.
Methodology
Participants
A total of 280 elderly patients of both sexes, with a mean age of 75.52 years, participated in this study. These individuals did not respond to conservative treatment for knee osteoarthritis and consequently underwent total knee arthroplasty.
Ethical Aspects
This study was conducted in accordance with ethical guidelines and regulations for research involving human subjects. The research protocol was approved by the Ethics Committee on the Brazil Platform under approval number 24845019.2.0000.5083.
All participants provided their informed consent by signing the Free and Informed Consent Form (TCLE), ensuring their voluntary participation and understanding of the study objectives, risks, and benefits. The study adhered strictly to the National Health Council (Conselho Nacional de Saúde - CNS) Resolution No. 466/2012, which establishes ethical principles for human research, including respect for dignity, autonomy, and confidentiality of participants.
Furthermore, the study complied with Brazil’s General Data Protection Law (Lei Geral de Proteção de Dados - LGPD, Law No. 13.709/2018), ensuring the protection of personal and sensitive data collected during the research. Data confidentiality, anonymity, and security were strictly maintained throughout the study, following national and international standards for ethical research involving human participants.
Inclusion and Exclusion Criteria
This study included elderly patients of both sexes, aged 60 years or older, diagnosed with advanced knee osteoarthritis who had not responded to conservative treatment. Additionally, participants had to meet the surgical indication for total knee arthroplasty and be able to provide informed consent by signing the Free and Informed Consent Form (TCLE).
Patients were excluded if they had a history of active infections in the knee joint, systemic inflammatory diseases such as severe rheumatoid arthritis or spondyloarthropathies, or severe deformities that would prevent the surgical procedure. Individuals with medical contraindications to surgery, including decompensated cardiopulmonary conditions posing a high surgical risk, were also excluded. Additionally, patients who were unable to provide informed consent were not included in the study.
Surgical Procedure – Total Knee Arthroplasty
The surgical procedure was performed using the Amplivision Navigation System, developed by Amplitude Surgical (France), with the aim of optimizing implant positioning and enhancing intraoperative precision. All patients included in the study underwent total knee arthroplasty performed by the same orthopedic surgeon, ensuring technical standardization and reproducibility of procedures.
The implants used were Score prostheses, manufactured by Amplitude Surgical (France), recognized for their advanced technology and biomechanical performance, making them suitable for uncemented knee arthroplasty.
The surgeon responsible for the procedures is a specialist in orthopedics and traumatology and a member of the Brazilian Society of Orthopedics and Traumatology (SBOT), a leading institution for the certification and professional development of specialists in the field. This expertise contributed to the consistency of surgical techniques and the rigorous application of technical and safety protocols during both the intraoperative and postoperative periods.
Analyzed Variables
This study analyzed a set of clinical, functional, radiographic, and qualitative variables to assess the outcomes of uncemented total knee arthroplasty (TKA). The selection of these variables aimed to measure the procedure’s effectiveness, safety, and impact on patients' quality of life.
Demographic variables included biological gender, date of birth, and the operated knee (right or left). Additionally, pre-existing diseases and comorbidities, such as systemic arterial hypertension, were considered to assess their influence on postoperative prognosis.
Functional and clinical variables were analyzed based on physical and functional examination findings, including the presence of persistent and intense pain, visible deformities, and chronic swelling. Moreover, the physical activity level of patients was recorded, classifying them into different categories according to the intensity of daily activities performed before surgery.
Biomechanical variables related to femoral and tibial movement were assessed using intraoperative navigation and imaging exams. Femoral movement variables included varus angle, valgus angle, tibial slope, and femoral rotation, while tibial movement variables included varus angle, valgus angle, flexion, extension, and tibial rotation. These measurements were crucial for determining the accuracy of component alignment and implant stability.
Subjective variables related to patient satisfaction were also included. Individual perceptions regarding pain relief, mobility improvement, ability to perform daily activities without difficulty, and sense of security while walking and engaging in physical activities were assessed. Additionally, an overall evaluation of satisfaction with surgical outcomes was considered, allowing for a comprehensive analysis of the intervention’s impact on the patient’s quality of life.
Finally, surgical procedure-related variables were recorded, including total surgical time, use of the intraoperative navigation system Amplivision (Amplitude Surgical, France), as well as the prosthetic model used (Score – Amplitude Surgical, France) and the surgical techniques applied by the responsible orthopedic surgeon.
Statistical Analysis
The statistical analysis was conducted using Python and MATLAB 2025, ensuring precision and reproducibility of statistical calculations. Initially, descriptive statistics were performed, including the calculation of mean, median, standard deviation, and interquartile range, to characterize the clinical, functional, and biomechanical variables of the study.
For inferential statistics, the Shapiro-Wilk normality test was applied to verify the distribution of the data. Since some variables did not follow normal distribution, non-parametric tests were adopted, including the Kruskal-Wallis test for comparisons between multiple groups. When statistical significance was detected (p < 0.05), Dunn’s post hoc test was performed to identify specific differences between groups.
Results
Table 1 presents the descriptive statistics and the respective p-values for the intragroup analysis of femoral and tibial movements. The variables analyzed include femoral varus, femoral valgus, femoral slope, and femoral rotation, as well as tibial varus, tibial valgus, tibial flexion, tibial extension, and tibial rotation. The results are expressed as mean values accompanied by standard deviations, which reflect the variability within the sample. Statistical significance was assessed using the Kruskal-Wallis test, with p-values below 0.05 considered significant. The purpose of this analysis is to determine whether these movements exhibit relevant variations within the studied group.
|
VARIABLE |
MEAN (± STANDARD DEVIATION) |
P-VALUE |
|
Femoral Varus (Degrees) |
0.82 (±0.04) |
<0.001* |
|
Femoral Valgus (Degrees) |
0.59 (±0.05) |
<0.001* |
|
Femoral Slope (Degrees) |
2.10 (±1.35) |
0.007 |
|
Femoral Rotation (Degrees) |
7.25 (±0.60) |
0.15 |
|
Tibial Varus (Degrees) |
0.55 (±0.07) |
0.51 |
|
Tibial Valgus (Degrees) |
0.54 (±0.08) |
0.87 |
|
Tibial Flexion (Degrees) |
4.40 (±2.20) |
0.009* |
|
Tibial Extension (Degrees) |
2.30 (±1.60) |
0.038* |
|
Tibial Rotation (Degrees) |
2.10 (±1.30) |
0.17 |
|
Legend: P-values indicate the statistical significance of intra-group differences, considered significant when p < 0.05 (*). Statistical tests applied: Shapiro-Wilk for normality, Kruskal-Wallis for non-parametric comparisons, Dunn's post hoc test for pairwise comparisons. |
||
Table 1: Statistical Summary of Femoral and Tibial Movements
Figure 1 illustrates the distribution of femoral and tibial movements through boxplots, allowing for a visual assessment of data dispersion and variability. Subfigure (a) represents femoral movement patterns, specifically femoral varus, femoral valgus, femoral slope, and femoral rotation, whereas subfigure (b) depicts tibial movement patterns, including tibial varus, tibial valgus, tibial flexion, tibial extension, and tibial rotation. The use of boxplots enables a detailed examination of central tendency, range, interquartile variability, and the presence of potential outliers, thus facilitating the identification of movement patterns that may be more pronounced or exhibit greater dispersion within the analyzed group.
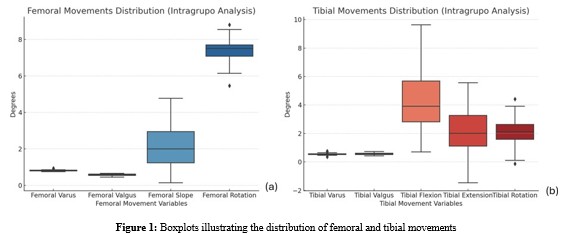
Legend: (a): The boxplot shows the range of femoral varus, valgus, slope, and rotation. Femoral rotation has the highest range of motion, while femoral varus and valgus show minimal variation; (b): The boxplot illustrates tibial varus, valgus, flexion, extension, and rotation. Tibial flexion and extension display the greatest variability, while tibial varus and valgus exhibit minimal dispersion.
The intragroup analysis of femoral movements revealed that femoral varus and femoral valgus exhibited relatively low mean values (0.82° and 0.59°, respectively), with minimal dispersion, as indicated by their small standard deviations. Both movements demonstrated statistically significant p-values (<0.001), suggesting a systematic pattern of variation in the sample, despite their limited magnitude. Femoral slope, on the other hand, presented a higher mean value (2.10°) with greater variability (SD = 1.35°), indicating more substantial movement differences among individuals. The statistical significance of this variable (p = 0.007) further supports its relevance in the biomechanical assessment of femoral motion. Conversely, femoral rotation exhibited the highest mean value (7.25°), reflecting a larger range of motion within the femoral kinematic parameters. However, its p-value (0.15) indicates that this variation was not statistically significant, suggesting that this movement may not be a key distinguishing factor in the sample.
Regarding tibial movements, tibial varus and tibial valgus demonstrated minimal mean values (0.55° and 0.54°, respectively) and exhibited no statistically significant differences (p-values of 0.51 and 0.87). This finding suggests that these movements remain relatively stable within the analyzed group, with limited inter-individual variation. In contrast, tibial flexion and tibial extension displayed broader movement ranges (4.40° and 2.30°, respectively) and achieved statistical significance (p = 0.009 and p = 0.038). These results highlight the dynamic nature of these movements, indicating that tibial flexion and extension may be critical factors influencing lower limb kinematics. Finally, tibial rotation, with a mean of 2.10° and a standard deviation of 1.30°, did not reach statistical significance (p = 0.17), suggesting that, despite its relatively higher magnitude compared to valgus movements, its variability does not present a significant distinguishing factor within the group.
Table 2 presents the distribution of categorical variables, including biological gender, the operated knee, and the presence of comorbidities, with values adjusted to a total of 280 participants. The table provides both absolute and relative frequencies, allowing a clearer understanding of the sample composition. The most prevalent categories, particularly regarding gender and comorbidities, highlight key aspects of the studied population.
|
CATEGORY |
COUNT |
PERCENTAGE (%) |
|
Biological Gender - Male |
110 |
39.29% |
|
Biological Gender - Female |
170 |
60.71% |
|
Operated Knee - Left |
163 |
58.21% |
|
Operated Knee - Right |
116 |
41.43% |
|
Comorbidities - Hypertension |
193 |
68.93% |
|
Comorbidities - Rheumatic Diseases |
43 |
15.36% |
|
Comorbidities - Hypertension & Diabetes |
21 |
7.5% |
|
Comorbidities - Renal Disease & Hypertension |
21 |
7.5% |
Table 2: Distribution of Categorical Variables
Most of the sample consists of female participants (60.71%), whereas male participants represent 39.29% of the total. This predominance of females is consistent with epidemiological data in studies on osteoarthritis and total knee arthroplasty, where women tend to have a higher prevalence of joint degenerative conditions.
Regarding the operated knee, the left knee was more frequently operated (58.21%) compared to the right knee (41.43%). This difference, although not highly pronounced, may indicate biomechanical factors or habitual preferences that lead to a greater incidence of left knee impairments requiring surgical intervention. Comorbidities were highly prevalent in the sample, particularly hypertension, which affected 68.93% of participants. This finding aligns with existing literature, as hypertension is commonly associated with degenerative joint diseases due to its links with systemic inflammation and vascular dysfunction.
Rheumatic diseases were present in 15.36% of participants, highlighting a considerable portion of patients with inflammatory conditions that may have contributed to joint degeneration. Additionally, 7.5% of participants had both hypertension and diabetes, while another 7.5% had renal disease associated with hypertension. These combined conditions reinforce the complexity of the clinical profiles observed in patients undergoing knee arthroplasty.
Discussion
Table 1 presents the statistical summary of femoral and tibial movements, emphasizing the biomechanical parameters observed in patients undergoing cementless total knee arthroplasty (TKA).
The analysis highlights key angular deviations, their statistical significance, and their potential implications for post-operative outcomes. Understanding these results is crucial for optimizing surgical techniques and ensuring implant longevity.
The analysis of femoral varus and femoral valgus revealed minimal mean deviations (0.82° ± 0.04 and 0.59° ± 0.05, respectively), both of which were statistically significant (p < 0.001). Although these values appear small, their significance suggests that even minor alterations in femoral alignment could have substantial biomechanical consequences. Previous research has indicated that excessive femoral varus or valgus may contribute to uneven load distribution across the knee joint, increasing the risk of early implant wear and loosening [1,2]. Therefore, precise alignment remains a critical factor in ensuring optimal post-operative function and long-term survivorship.
The femoral slope, with a mean of 2.10° ± 1.35 (p = 0.007), exhibited greater variability compared to other femoral parameters. The posterior tibial slope has been extensively studied for its influence on knee kinematics, particularly in posterior cruciate-retaining implants. Excessive posterior slope can increase flexion instability and posterior translation of the tibia, whereas inadequate slope may lead to anterior impingement and restricted range of motion [3,26]. This variability suggests that intraoperative techniques should focus on achieving an optimal femoral slope to minimize complications.
Interestingly, femoral rotation demonstrated the highest mean value (7.25° ± 0.60), but its p-value (0.15) indicated a lack of statistical significance. Femoral rotation plays a crucial role in patellofemoral tracking, and excessive external or internal rotation has been associated with anterior knee pain and patellar maltracking [5,6]. Although the present study did not find significant intra-group differences in this parameter, previous studies suggest that rotational alignment errors, even within this range, could contribute to functional impairments over time [11].
Tibial alignment parameters, including tibial varus (0.55° ± 0.07, p = 0.51) and tibial valgus (0.54° ± 0.08, p = 0.87), did not reach statistical significance. These results suggest that small variations in tibial coronal alignment may not significantly impact early post- operative outcomes. However, literature has shown that excessive tibial varus can lead to increased medial compartment loading, which may contribute to accelerated polyethylene wear and implant loosening in the long term [23,28]. Conversely, excessive valgus alignment may predispose patients to lateral instability, underscoring the importance of careful intraoperative adjustments to maintain neutral alignment.
In contrast, tibial flexion (4.40° ± 2.20, p = 0.009) and tibial extension (2.30° ± 1.60, p = 0.038) were both statistically significant. These findings align with existing literature, which highlights the impact of sagittal tibial alignment on knee stability and implant kinematics [14,11]. Specifically, an increased tibial flexion angle may affect quadriceps efficiency and contribute to flexion contractures, while excessive tibial extension may result in hyperextension instability. These results reinforce the importance of individualized surgical planning to achieve proper sagittal tibial alignment.
Lastly, tibial rotation (2.10° ± 1.30, p = 0.17) did not demonstrate statistical significance. While rotational alignment is critical for optimal knee function, particularly in terms of tibiofemoral congruence, the present findings suggest that within this range, rotational deviations may not substantially impact post-operative outcomes. However, studies indicate that excessive internal tibial rotation can lead to patellar maltracking and anterior knee pain, while excessive external rotation can compromise flexion stability [15,16]. Thus, while this study did not find significant differences, clinical judgment remains essential in ensuring appropriate tibial rotational alignment.
The findings of this study align with previous research emphasizing the importance of precise implant positioning in cementless TKA. The statistical significance of femoral slope, tibial flexion, and tibial extension suggests that these parameters play a crucial role in optimizing knee biomechanics. These results are consistent with studies that advocate for meticulous alignment strategies to minimize complications such as early aseptic loosening and excessive wear [19,20].
Moreover, the lack of statistical significance in femoral rotation and tibial rotation aligns with previous meta-analyses, which suggest that rotational alignment, while essential, may have less immediate impact on functional outcomes than sagittal and coronal alignment parameters [12,18]. This is further supported by findings from Forlenza et al. (2023) and Goh et al. (2022), who noted that while rotational errors can contribute to complications, their effects may be more pronounced in specific patient subgroups, such as those with pre-existing malalignment or high-demand activities [6,29].
Table 2 provides an overview of key categorical variables within the study population, including biological gender distribution, laterality of the operated knee, and the presence of comorbidities. Understanding these demographic and clinical characteristics is essential for evaluating trends in total knee arthroplasty (TKA) and identifying factors that may influence surgical outcomes and long-term prognosis.
The results indicate a predominance of female patients (60.71%) compared to male patients (39.29%) undergoing cementless TKA. This gender disparity aligns with existing literature, which consistently reports a higher prevalence of knee osteoarthritis (OA) among women [1,26]. The increased susceptibility of females to knee OA has been attributed to several factors, including hormonal influences, anatomical differences, and biomechanical variations [2,11]. Postmenopausal estrogen decline, for example, has been linked to cartilage degeneration and increased joint laxity, predisposing women to a higher incidence of OA and a greater need for surgical intervention.
Furthermore, women often experience more severe functional impairment and pain before opting for surgery, possibly due to differences in pain perception and healthcare-seeking behaviors [8,12]. These findings emphasize the need for gender-specific approaches in preoperative assessment and rehabilitation protocols to ensure optimal patient outcomes.
The distribution of the operated knee reveals that the left knee was more frequently operated (58.21%) than the right knee (41.43%). While this difference may seem subtle, it raises interesting biomechanical considerations. Studies suggest that the dominant leg tends to be less affected by OA, as it is more actively engaged in dynamic activities, such as balance control and load absorption, which may help preserve joint integrity over time [23,28]. Conversely, the non-dominant leg is often subjected to compensatory loading, increasing the risk of degenerative changes and ultimately leading to a higher rate of surgical intervention.
Additionally, cultural and occupational factors may contribute to this discrepancy. In right-leg dominant individuals, which constitute the majority of the population, the left leg is more exposed to weight-bearing asymmetries, potentially leading to earlier cartilage deterioration [13,14]. However, further research is needed to determine whether laterality significantly affects post- operative functional outcomes and recovery rates.
Among the reported comorbidities, hypertension was the most common condition, affecting 68.93% of the patients. This high prevalence is consistent with previous studies that identify hypertension as a major comorbidity in TKA patients [6,19]. Hypertension has been linked to systemic inflammation, endothelial dysfunction, and impaired microcirculation, all of which can negatively impact joint health and surgical recovery [15,20].
Additionally, hypertension is associated with a higher risk of perioperative complications, including increased intraoperative bleeding, delayed wound healing, and postoperative cardiovascular events [4,27]. Given these risks, optimizing blood pressure management before and after surgery is crucial in improving patient outcomes.
A significant proportion of patients (15.36%) were diagnosed with rheumatic diseases, including conditions such as rheumatoid arthritis (RA) and other inflammatory arthropathies. Unlike primary OA, which is primarily mechanical in origin, rheumatic conditions involve systemic inflammation, which accelerates joint degradation and often necessitates earlier surgical intervention [18,25].
Patients with inflammatory arthritis present unique challenges in TKA due to bone quality concerns, increased risk of infection, and altered healing responses [5,9]. The presence of active inflammation may also impact prosthesis survival, emphasizing the importance of preoperative immunosuppressive therapy adjustments to optimize outcomes [16,22].
A smaller, yet clinically significant portion of the cohort (7.5% each) had both hypertension and diabetes or hypertension and renal disease. These multimorbid conditions suggest an increased cardiovascular and metabolic burden, which has been linked to poorer surgical outcomes and higher complication rates in TKA patients [8,21].
Diabetes, for instance, negatively impacts wound healing and increases the risk of periprosthetic joint infection (PJI) [24,17]. Patients with renal disease, on the other hand, often exhibit bone metabolism alterations, which can affect implant osseointegration in cementless TKA, potentially leading to early loosening or implant failure [23,26].
The presence of multiple comorbidities necessitates a multidisciplinary approach, with preoperative screening and postoperative monitoring playing key roles in mitigating complications and optimizing patient recovery [10,22].
The findings from Table 2 provide valuable insights into the demographic and clinical characteristics of patients undergoing cementless TKA. The predominance of female patients is consistent with broader epidemiological trends, emphasizing the need for gender-specific surgical considerations, such as implant selection and rehabilitation strategies tailored to differences in knee kinematics and bone quality
[2,11].
The higher prevalence of left knee surgeries raises interesting biomechanical and functional implications that warrant further investigation. Future studies should explore whether laterality influences implant survivorship, functional recovery, and patient- reported outcomes in cementless TKA.
Lastly, the high prevalence of hypertension and multimorbidity underscores the importance of preoperative risk stratification and individualized perioperative management. Given the well- documented association between systemic conditions and surgical complications, addressing cardiovascular and metabolic risk factors is essential to enhancing surgical outcomes and improving long-term implant performance [9,14].
Future research should focus on long-term follow-up studies to assess how these demographic and comorbidity factors influence implant longevity and functional outcomes. Additionally, advancements in surgical techniques, patient optimization protocols, and postoperative care will be crucial in mitigating risks and ensuring successful outcomes in cementless TKA.
Conclusion
This study aimed to analyze the clinical and functional outcomes of unilateral cementless total knee arthroplasty (TKA), assessing its efficacy, safety, and impact on patient recovery. The findings provide valuable insights into the biomechanical characteristics, demographic distribution, and comorbidities of patients undergoing this procedure, contributing to a more comprehensive understanding of its benefits and potential limitations.
The results indicate that cementless TKA is a viable and effective surgical approach, with statistically significant improvements in key femoral and tibial alignment parameters, particularly in sagittal alignment (femoral slope, tibial flexion, and tibial extension). These findings reinforce previous studies that highlight the importance of precise implant positioning in ensuring long-term stability and functional outcomes. Additionally, the predominance of female patients and the higher prevalence of left knee surgeries reflect broader epidemiological trends in knee osteoarthritis, warranting further investigation into gender- and laterality-specific surgical considerations.
From a clinical perspective, hypertension emerged as the most prevalent comorbidity (68.93%), emphasizing the need for optimized perioperative management to reduce cardiovascular risks and enhance surgical success. Moreover, the presence of multimorbidities, such as hypertension combined with diabetes or renal disease, highlights the complex health profiles of many patients undergoing TKA, necessitating a multidisciplinary approach for preoperative optimization and postoperative care.
When comparing cementless TKA to the conventional cemented technique, several advantages were noted. Cementless implants have been associated with improved osseointegration, reduced bone cement-related complications, and potential long-term survivorship benefits. However, they also present challenges such as increased risk of early aseptic loosening, particularly in patients with osteoporosis or metabolic disorders. These findings align with recent studies that suggest patient selection criteria should be carefully considered when opting for a cementless approach.
Despite its promising results, cementless TKA requires further long-term studies to confirm its superiority over cemented techniques in terms of implant longevity, functional recovery, and complication rates. The evolution of modern surgical technologies, including robotic-assisted TKA and advanced implant materials, may enhance precision in implant positioning and improve patient outcomes.
In conclusion, this study supports the efficacy and safety of cementless TKA, emphasizing its potential advantages in younger and active patients with good bone quality. However, individualized patient selection, meticulous surgical technique, and comprehensive postoperative care remain essential to maximize the benefits of this approach. As the trend towards cementless TKA continues to grow, future research should focus on comparing long- term clinical outcomes, refining surgical strategies, and optimizing patient recovery pathways to further establish its role in modern knee arthroplasty [29-32].
Financial Support
The company Amplitude Surgical Latam, sponsor of this publication, headquartered in Rio Claro, São Paulo, Brazil, reaffirms its commitment to technological innovation and scientific advancement in the orthopedic sector.
References
- Agarwal, A. R., Kuyl, E. V., Gu, A., Golladay, G. J., Thakkar,S. C., Siram, G., ... & Rao, S. (2024). Trend of using cementless total knee arthroplasty: a nationwide analysis from 2015 to 2021. Arthroplasty, 6(1), 24.
- Boontanapibul, K., Amanatullah, D. F., Huddleston III, J. I., Maloney, W. J., & Goodman, S. B. (2021). Outcomes of cemented total knee arthroplasty for secondary osteonecrosis of the knee. The Journal of Arthroplasty, 36(2), 550-559.
- Carlson, B. J., Gerry, A. S., Hassebrock, J. D., Christopher,Z. K., Spangehl, M. J., & Bingham, J. S. (2022). Clinical outcomes and survivorship of cementless triathlon total knee arthroplasties: a systematic review. Arthroplasty, 4(1), 25.
- Chen, C., Shi, Y., Wu, Z., Gao, Z., Chen, Y., Guo, C., & Bao,X. (2021). Long-term effects of cemented and cementless fixations of total knee arthroplasty: a meta-analysis and systematic review of randomized controlled trials. Journal of Orthopaedic Surgery and Research, 16, 1-14.
- Edgar, M., Harvey, J., Jiang, S., Walters, J., Kozina, E., Kaplan, N., ... & Chmell, S. (2023). Cemented total knee arthroplasty provides greater knee range of motion at 2 years than cementless technique. European Journal of Orthopaedic Surgery & Traumatology, 33(8), 3561-3568.
- Forlenza, E. M., Serino III, J., Terhune, E. B., Weintraub, M. T., Nam, D., & Della Valle, C. J. (2023). Cementless total knee arthroplasty is associated with early aseptic loosening ina large national database. The Journal of Arthroplasty, 38(7), S215-S220.
- Goh, G. S., Fillingham, Y. A., Sutton, R. M., Small, I., Courtney, P. M., & Hozack, W. J. (2022). Cemented versus cementless total knee arthroplasty in obese patients with body mass index≥ 35 kg/m2: a contemporary analysis of 812 patients. The Journal of Arthroplasty, 37(4), 688-693.
- Hannon, C. P., Salih, R., Barrack, R. L., & Nunley, R. M. (2023). Cementless versus cemented total knee arthroplasty: concise midterm results of a prospective randomized controlled trial. JBJS, 105(18), 1430-1434.
- Mercurio, M., Gasparini, G., Sanzo, V., Familiari, F., Castioni, D., & Galasso, O. (2022). Cemented total knee arthroplasty shows less blood loss but a higher rate of aseptic loosening compared with cementless fixation: an updated meta-analysis of comparative studies. The Journal of Arthroplasty, 37(9), 1879-1887.
- Mohammad, H. R., Judge, A., & Murray, D. W. (2024). A comparison of the periprosthetic fracture rate of cemented and cementless total knee arthroplasties: an analysis of data from the national joint registry. The Journal of Arthroplasty, 39(6), 1505-1511.
- Kim, Y. H., Park, J. W., & Jang, Y. S. (2021). The 22 to 25-year survival of cemented and cementless total knee arthroplasty in young patients. The Journal of arthroplasty, 36(2), 566-572.
- Liu, Y., Zeng, Y., Wu, Y., Li, M., Xie, H., & Shen, B. (2021). Acomprehensive comparison between cementless and cemented fixation in the total knee arthroplasty: an updated systematic review and meta-analysis. Journal of orthopaedic surgery and research, 16, 1-14.
- Rodriguez, S., & Ranawat, A. S. (2021). The future is non- cemented total knee arthroplasty: volume trends at the hospital for special surgery. Indian Journal of Orthopaedics, 55, 1096- 1100.
- Nam, D., Bhowmik-Stoker, M., Mahoney, O. M., Dunbar,M. J., & Barrack, R. L. (2023). Mid-term performance of the first mass-produced three-dimensional printed cementless tibia in the United States as reported in the American joint replacement registry. The Journal of Arthroplasty, 38(1), 85- 89.
- Schwabe, M. T., & Hannon, C. P. (2022). The evolution, current indications and outcomes of cementless total knee arthroplasty. Journal of Clinical Medicine, 11(22), 6608.
- Tanariyakul, Y., Kanitnate, S., & Tammachote, N. (2024). Cementless and cemented total knee arthroplasties have similar outcomes but cementless patellar component migration was observed in a paired randomized control trial. The Journal of Arthroplasty, 39(5), 1266-1272.
- Sheridan, G. A., Cassidy, R. S., McKee, C., Hughes, I., Hill, J. C., & Beverland, D. E. (2023). Survivorship of 500 cementless total knee arthroplasties in patients under 55 years of age. The Journal of Arthroplasty, 38(5), 820-823.
- Uivaraseanu, B., Vesa, C. M., Tit, D. M., Maghiar, O., Maghiar,T. A., Hozan, C., ... & Bungau, S. (2022). Highlighting the advantages and benefits of cementless total knee arthroplasty. Experimental and Therapeutic Medicine, 23(1),58.
- Helvie, P. F., Deckard, E. R., & Meneghini, R. M. (2023). Cementless total knee arthroplasty over the past decade: excellent survivorship in contemporary designs. The Journal of Arthroplasty, 38(6), S145-S150.
- Monarrez, R., Dubin, J., Bains, S. S., Hameed, D., Moore, M. C., Chen, Z., ... & Nace, J. (2024). Cemented is not superior to cementless total knee arthroplasty for complications: a propensity score matched analysis. European Journal of Orthopaedic Surgery & Traumatology, 34(4), 1825-1830.
- WilczyÅ?ski, M., Bieniek, M., Krakowski, P., & KarpiÅ?ski, R. (2024). Cemented vs. cementless fixation in primary knee replacement: A narrative review. Materials, 17(5), 1136.
- Nam, D., Lawrie, C. M., Salih, R., Nahhas, C. R., Barrack, R. L., & Nunley, R. M. (2019). Cemented versus cementless total knee arthroplasty of the same modern design: a prospective, randomized trial. JBJS, 101(13), 1185-1192.
- Chen, A. G., Sogbein, O. A., McCalden, R. W., Bohm, E. R., & Lanting, B. A. (2025). Survivorship of modern cementless total knee arthroplasty: analysis from the Canadian Joint Replacement Registry. The Journal of Arthroplasty, 40(2), 380-385.
- Mosher, Z. A., Bolognesi, M. P., Malkani, A. L., Meneghini, R. M., Oni, J. K., & Fricka, K. B. (2024). Cementless total knee arthroplasty: a resurgence—who, when, where, and how?. The Journal of Arthroplasty, 39(9), S45-S53.
- Ailaney, N., Barra, M. F., Schloemann, D. T., Thirukumaran, C. P., & Kaplan, N. B. (2024). Short-term (6 months or less) pain in cemented versus cementless total knee arthroplasty: a systematic review and meta-analysis. The Journal of arthroplasty.
- Gibbons, J. P., Cassidy, R. S., Bryce, L., Napier, R. J., Bloch, B. V., & Beverland, D. E. (2023). Is cementless total knee arthroplasty safe in women over 75 Y of age?. The Journal of Arthroplasty, 38(4), 691-699.
- Gwam, C. U., George, N. E., Etcheson, J. I., Rosas, S., Plate, J. F., & Delanois, R. E. (2019). Cementless versus cemented fixation in total knee arthroplasty: usage, costs, and complications during the inpatient period. The journal of knee surgery, 32(11), 1081-1087.
- de Vries, E., Sánchez, E., Janssen, D., Matthews, D., & van der Heide, E. (2022). Predicting friction at the bone–Implant interface in cementless total knee arthroplasty. journal of the mechanical behavior of biomedical materials, 128, 105103.
- Goh, G. S., Fillingham, Y. A., Ong, C. B., Krueger, C. A., Courtney, P. M., & Hozack, W. J. (2022). Redefining indications for modern cementless total knee arthroplasty: clinical outcomes and survivorship in patients> 75 years old. The Journal of Arthroplasty, 37(3), 476-481.
- AbdioÄ?lu, A. A., & Peker, G. (2024). Comparison of bilateral cementless total knee arthroplasty results between patients in different BMI groups. Archives of Orthopaedic and Trauma Surgery, 144(5), 2317-2326.
- Asokan, A., Plastow, R., Kayani, B., Radhakrishnan, G. T., Magan, A. A., & Haddad, F. S. (2021). Cementless knee arthroplasty: a review of recent performance. Bone & Joint Open, 2(1), 48-57.
- Quispel, C. R., Duivenvoorden, T., Beekhuizen, S. R., Verburg, H., Spekenbrink-Spooren, A., Van Steenbergen, L. N., ... & De Ridder, R. (2021). Comparable mid-term revision rates of primary cemented and cementless total knee arthroplasties in 201,211 cases in the Dutch Arthroplasty Register (2007– 2017). Knee Surgery, Sports Traumatology, Arthroscopy, 29, 3400-3408.