
International Journal of Clinical & Experimental Dermatology(IJCED)
ISSN: 2476-2415 | DOI: 10.33140/IJCED
Impact Factor: 1.9

Case Report - (2025) Volume 10, Issue 1
Trichotillomania in Childhood: A Sign of Emotional Distress
Received Date: Jan 02, 2025 / Accepted Date: Feb 03, 2025 / Published Date: Feb 20, 2025
Copyright: ©Â©2025 S Boujloud. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Boujloud, S., El Fatoiki, F. Z., Hali, F., Chiheb, S. (2025). Trichotillomania in Childhood: A Sign of Emotional Distress. Int J Clin Expl Dermatol, 10(1), 01-03.
Abstract
Trichotillomania is a psychodermatologic disorder characterized by repetitive hair pulling, resulting in hair loss and associated with significant social and psychological challenges. It is a relatively common cause of childhood alopecia that can be difficult to diagnose. Trichoscopy effectively supports differential diagnosis of various hair and scalp diseases by identifying key features indicative of trichotillomania. A multidisciplinary approach tailored to the child’s individual needs, along with family support, is essential for successful management and sustained remission.
Keywords
Trichotillomania, Trichoscopy, Hair Loss, Childhood Alopecia
Abbreviations
NAC = N-acetylcysteine
DSM-5 = Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
Introduction
Trichotillomania is characterized by the repetitive pulling out of hair leading to hair loss. Most people with trichotillomania commonly pull from the scalp, eyebrows, and eyelashes, but any bodily site with hair can be affected.
The disorder can be associated with serious social and psychologic dysfunction, as well as medical problems. Trichotillomania is a relatively common cause of childhood alopecia that can be sometimes difficult to diagnose. We are reporting a case of five children suffering from trichotillomania.
Case Report
A case reports of trichotillomania, identified in the pediatric dermatology consultation. We collected epidemiological data concerning age, sex and medical history of each patient. Diagnosis was based on anamnestic arguments, clinical examination data and trichoscopy. We report five pediatric cases, including three girls. The average age of the patients was 11 years (ranging from 7 to 14 years).
Diagnosis delay was between 6 months and 2 years of evolution. The precipitating factors and association reported in these cases were : changing school ; stress at school; anxious and nervous personality; attention-deficit and hyperactivity disorder.
The dermatological examination found incomplete circumscribed alopecia plates with hair of different length without damage to the eyebrows; no nail-biting or skin-picking. The sign of traction and the mycological examination were negative.
The trichoscopy showed signs of broken hair (Figure 2a, 2c), follicular microhemorrhage (Figure 2b), trichoptilosis, black spots and flame hairs. All children were referred to a child psychiatrist for specialized follow-up and management.



Figure 1: Clinical Presentations of Hair Loss Area/Patches Observed in Some of the Cases
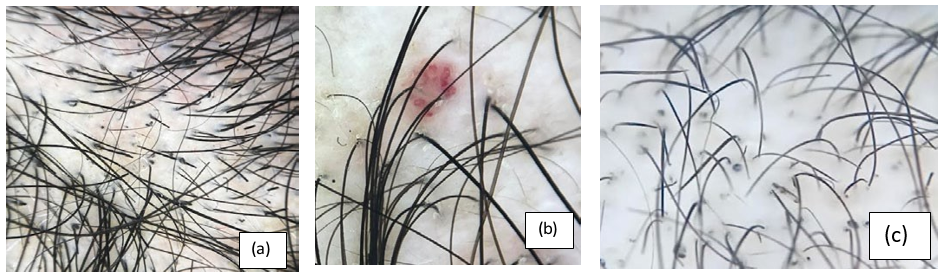
Figure 2: Dermoscopic Findings of Trichotillomania
Discussion
Trichotillomania, as defined by the Diagnostic and Statistical Manual of Mental Disorders, is an obsessive-compulsive or related disorder characterized by recurrent hair-pulling from any part of the body, resulting in hair loss [1,2].
The etiology of trichotillomania remains poorly understood. However, it is believed to result from the interplay of multiple factors, including genetic, social, psychological and neurobiological influences [3,4].
Although trichotillomania can be triggered by stress, the behavior often leads to significant emotional consequences, such as low self- esteem, distress, guilt and shame. Interestingly, most individuals describe hair-pulling as painless or even pleasurable [5].
The clinical presentation is not typical, which is why it is important to eliminate other differential diagnoses such as telogen effluvium due to nutritional deficiencies, alopecia areata, tinea capitis, or a psychiatric disorder underlying the compulsive behavior.
The specific criteria for trichotillomania according to The American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-5), are as follows (5):
• Repeated attempts to decrease or stop the hair-pulling behavior
• The hair pulling causes clinically significant distress or impairment in social, occupational, or other important areas of functioning
• The hair pulling or hair loss cannot be attributed to another medical condition
• The hair pulling cannot be better explained by the symptoms of another mental disorder
Trichoscopy in this case is very important [6,7]. It is characterized by the presence of hairs broken at different length, black dots, trichoptilosis, coiled hairs, flame hairs, V-sign and tulip hairs. Yellow dots, upright regrowing hairs and exclamation mark hairs may be observed.
Managing pediatric trichotillomania remains challenging, requiring the identification of underlying psychopathological causes to propose tailored therapies for the child, while considering the family environment. Behavioral therapy has shown success in managing trichotillomania, but not all patients are able or willing to adhere to this approach.
Currently, no medications are specifically approved for the treatment of trichotillomania. However, certain drugs, such as selective serotonin reuptake inhibitors, tricyclic antidepressants, and glutamate-modulating agents may help control the symptoms. N-acetylcysteine is considered a first-line option due to significant benefits and low risk of side effects [4].
While NAC has shown significant effects in adults with trichotillomania at a dosage of 1,200 mg twice daily, pediatric trial data did not reveal any benefit. This may be because children tend to engage more in automatic hair-pulling behaviors, whereas NAC might be more effective for focused pulling by reducing the urge to pull hair [8].
In pediatric cases, a psychiatry-dermatology liaison is crucial, accompanied by comprehensive support services to meet the needs of both the patient and his parents. Social support plays a important role in habit reversal training, and physicians must emphasize the importance of family involvement in achieving successful outcomes and sustained remission
Pediatric trichotillomania is a multifaceted condition that necessitates a multidisciplinary team approach tailored to the individual needs of a child.
Conclusion
Trichotillomania is a complex psychodermatologic disorder with many aspects still requiring further exploration. It is a relatively frequent cause of childhood alopecia and can be challenging to diagnose and requires an interdisciplinary approach that addresses both the physiological and psychological aspects of the condition.
References
- Panza, K. E., Pittenger, C., & Bloch, M. H. (2013). Age and gender correlates of pulling in pediatric trichotillomania. Journal of the American Academy of Child & Adolescent Psychiatry, 52(3), 241-249.
- Fernandes, M. R. D. N., Melo, D. F., Vincenzi, C., Lima, C. D. S., & Tosti, A. (2021). Trichotillomania incognito: two case reports and literature review. Skin appendage disorders, 7(2), 131-134.
- França, K., Kumar, A., Castillo, D., Jafferany, M., Hyczy da Costa Neto, M., Damevska, K., ... & Lotti, T. (2019). Tricho- tillomania (hair pulling disorder): clinical characteristics, psy- chosocial aspects, treatment approaches, and ethical consider- ations. Dermatologic therapy, 32(4), e12622.
- Tostif, A. (2021). Trichotillomania: What Do We Know So Far?.
- Association., American Psychiatric. Diagnostic and Statistical Manual of Mental Disorders Fifth Edition Text Revision. Washington, 2013. 251-4.
- Abraham, L. S., Torres, F. N., & Azulay-Abulafia, L. (2010). Dermoscopic clues to distinguish trichotillomania from patchy alopecia areata. Anais brasileiros de dermatologia, 85, 723-726.
- Fernandes, M. R. D. N., Melo, D. F., Vincenzi, C., Lima, C. D. S., & Tosti, A. (2021). Trichotillomania incognito: two case reports and literature review. Skin appendage disorders, 7(2), 131-134.
- Bloch, M. H., Panza, K. E., Grant, J. E., Pittenger, C., & Leckman, J. F. (2013). N-Acetylcysteine in the treatment of pediatric trichotillomania: a randomized, double-blind, placebo-controlled add-on trial. Journal of the American Academy of Child & Adolescent Psychiatry, 52(3), 231-240.