
International Journal of Preventive Medicine and Care(IJPMC)
ISSN: 2994-032X | DOI: 10.33140/IJPMC

Research Article - (2024) Volume 2, Issue 2
Trends in Sudden Cardiac Death in Pilots: A Post COVID-19 Challenging Crisis of Global Perspectives (2011-2023) - A Systematic Review and Meta-Analysis
Received Date: Jul 23, 2024 / Accepted Date: Aug 17, 2024 / Published Date: Aug 28, 2024
Copyright: ©Â©2024 Julian Yin Vieira Borges. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Borges, J. Y. V. (2024). Trends in Sudden Cardiac Death in Pilots: A Post COVID-19 Challenging Crisis of Global Perspectives (2011-2023) - A Systematic Review and Meta-Analysis. Int J Prev Med Care, 2(2), 01-12.
Abstract
Background: Sudden cardiac death (SCD) remains a significant threat to pilots and is a leading cause of death worldwide, jeopardizing flight safety and causing devastating consequences. This review examines trends in SCD among pilots from a global perspective, analyzing evidence from 2011 to 2023, with a focus on its growing impact as a global crisis and recent findings pointing to a potential rise in incidence, particularly after 2019.
Objectives: To analyze the prevalence, risk factors and prevention strategies for SCD in pilots, particularly post-COVID-19.
Methods: The PRISMA guidelines for systematic meta-analysis was used, a search of peer-reviewed literature for international aviation databases, and pilot associations was conducted to identify relevant data. The analysis focused on trends in SCD prevalence, risk factors, prevention strategies, and recent findings, including the potential impact of COVID-19, the role of vaccination, and important biomarkers to screen for predisposition. Eligibility criteria included studies reporting SCD incidence, risk factors, or prevention strategies in pilots. Data were extracted, and meta-analyses conducted.
Results: Recent studies suggest a potential increase in SCD incidence among pilots following the COVID-19 pandemic. Cardiovascular complications, increased stress, disruptions in healthcare, and changes in lifestyle may contribute to this potential rise. Identified risk factors include age, male gender, and cardiovascular comorbidities. Biomarkers such as troponin, N-terminal pro-B-type natriuretic peptide (NT-proBNP), and high-sensitivity C-reactive protein (hs-CRP) have been identified as potential indicators of increased SCD risk in pilots. Preventive measures include regular cardiovascular assessments and lifestyle modifications.
Conclusion: SCD remains a significant and rising threat to pilots, posing a global crisis that requires immediate attention. Through a comprehensive approach that includes risk assessment, preventive measures, emergency response, and preventive protocols, the aviation industry can mitigate this risk and safeguard the lives of pilots and passengers.
This review also suggests standardized examination protocol for pilots includes regular cardiovascular risk assessment, biomarker screening, monitoring of COVID-19 and vaccination status, lifestyle modifications, and a standardized reporting system. The adoption of a standardized protocol by aviation regulatory bodies and airlines worldwide is crucial to address the growing threat of SCD among pilots and ensure the highest standards of aviation safety.
Keywords
Sudden Cardiac Death (SCD), Pilots, Aviation Safety, Global Crisis, Rising Threat, Covid-19, Biomarkers, Prevention Strategies
Introduction
Sudden cardiac death (SCD) is a leading cause of death worldwide, claiming an estimated 17 million lives annually [1]. In the United States alone, SCD accounts for over 350,000 deaths each year, with a significant proportion occurring in seemingly healthy individuals [2]. The global burden of SCD is substantial, and its impact on society, families, and healthcare systems cannot be overstated.
The airline industry has experienced unprecedented challenges in recent years, with the COVID-19 pandemic exacerbating existing concerns and introducing new ones. One such emerging issue is the rise in sudden cardiac death (SCD) among pilots, which has become a significant global concern [3].
In the aviation industry, SCD poses a unique and particularly devastating threat due to its potential to compromise flight safety, making it a critical global concern [4]. Unlike other industries where an individual's sudden incapacitation may have limited consequences, a pilot's sudden incapacitation due to SCD can lead to catastrophic accidents, endangering the lives of passengers, crew, and people on the ground. The high-stakes nature of aviation, coupled with the responsibility pilots bear for the safety of others, magnifies the significance of SCD in this context.
Pilots are at an increased risk of SCD due to a combination of factors, including underlying heart conditions, age, and lifestyle factors [5]. The demanding nature of the profession, irregular work schedules, and exposure to various stressors such as altitude changes, jet lag, and long working hours can take a toll on pilots' cardiovascular health [6]. Additionally, the sedentary nature of the job, limited opportunities for regular exercise, and disrupted sleep patterns can contribute to the development of risk factors for SCD, such as obesity, hypertension, and diabetes [7].
The period from 2011 to 2023 has witnessed a significant shift in the landscape of aviation safety, particularly with regard to the threat of sudden cardiac death (SCD) among pilots. Recent studies suggest a potential increase in SCD incidence among pilots following the COVID-19 pandemic [8]. Cardiovascular complications, increased stress, disruptions in healthcare, and changes in lifestyle may contribute to this potential rise [9]. Additionally, concerns have been raised about the potential role of COVID-19 vaccination in increasing the risk of myocarditis, a condition that can lead to SCD [10]. However, further research is needed to fully understand the relationship between vaccination and SCD risk [11].
The International Civil Aviation Organization (ICAO) has recognized SCD as a significant threat to aviation safety and has called for a global effort to address this issue [12]. The ICAO has emphasized the need for robust medical screening, regular health assessments, and the implementation of preventive strategies to mitigate the risk of SCD among pilots [12]. However, despite these efforts, SCD remains a persistent concern in the aviation industry. Current guidelines and protocols for cardiovascular risk assessment in pilots vary across countries and airlines. The International Civil Aviation Organization (ICAO) provides general recommendations for medical examination of pilots, including cardiovascular evaluation [13].
However, these recommendations are not universally adopted, and there is a lack of standardization in the scope and frequency of cardiovascular risk assessment [14]. This highlights the need for a comprehensive and evidence-based protocol to mitigate the risk of SCD in pilots. Given the growing burden of SCD in pilots post-COVID-19 and the potential global aviation crisis impact, there is a pressing need to conduct a systematic review and meta-analysis to examine the current trends in SCD prevalence, determine risk factors, and outline potential preventive measures.
This Review Aims to Address the Following Key Questions
1. Has the incidence of SCD among pilots increased following the COVID-19 pandemic, and if so, to what extent?
2. Is there an association between COVID-19 vaccination and an increased risk of SCD in pilots, particularly through the development of myocarditis?
3. What are the most effective protocols and preventive measures that can be implemented to standardize the medical examination and screening procedures for pilots to mitigate the risk of SCD?
This review aims to provide a comprehensive analysis of the current state of knowledge on SCD in pilots and identify gaps in the literature that require further research. The findings have great importance for aviation regulatory bodies, airlines, and healthcare providers involved in the care of pilots, informing the development of evidence-based strategies to enhance aviation safety and safeguard the lives of those who navigate the skies.
A comprehensive trend analysis of SCD incidence among pilots during this period was conducted, paying close attention to any potential changes associated with the COVID- 19 pandemic. This included examining the potential impact of COVID-19 on cardiovascular complications, the potential impact of COVID-19 and vaccination on SCD prevalence, and risk factors such as stress levels, healthcare access, and lifestyle factors that, if increased, have the potential to contribute to an increase in SCD risk.
Furthermore, an investigation concerning the direct association between certain types of COVID-19 vaccines and the development of myocarditis, a condition linked to SCD, was conducted. While concerns have been raised about this potential link, further research is necessary to fully understand the relationship between vaccination and SCD risk.
To mitigate the risk of SCD in pilots, the review aims to identify biomarkers that can effectively predict individuals at increased risk. These biomarkers will serve as valuable tools for early detection and intervention, potentially saving lives. The identification of reliable biomarkers for SCD risk in pilots could lead to the development of targeted screening programs and personalized prevention strategies [15].
This critical examination of SCD in pilots during a time of significant change will provide invaluable insights into this complex issue. By focusing on updated trends, potential risk factors, and preventive measures, we aim to enhance aviation safety and safeguard the lives of those who navigate the skies. The findings of this review will have important implications for aviation regulatory bodies, airlines, and healthcare providers involved in the care of pilots [16].
Methods
Data Sources and Search Strategy
A comprehensive search was conducted in multiple databases, including PubMed, Embase, Scopus, Web of Science, and Cochrane Library. The search strategy combined keywords related to sudden cardiac death, pilots, aviation safety, COVID-19, vaccination, biomarkers, and risk factors.
The search terms were adapted for each database and included both free text and controlled vocabulary terms (e.g., MeSH terms in PubMed) to ensure a comprehensive search. The exact search terms used for each database are provided in the supplementary materials to enable reproducibility. This systematic review was conducted following the PRISMA guidelines.
In addition to the database searches, the grey literature was also searched, including conference proceedings, abstracts, and reports from relevant organizations such as the International Civil Aviation Organization (ICAO), the Federal Aviation Administration (FAA), and the European Union Aviation Safety Agency (EASA). The reference lists of included studies and relevant review articles were also hand-searched to identify any additional studies that may have been missed in the database searches
Study Selection
The Inclusion Criteria for This Review Were As Follows
1. Studies that reported on the incidence, prevalence, or risk factors for SCD in pilots.
2. Studies that investigated the potential impact of COVID-19 or COVID-19 vaccination on SCD risk in pilots.
3. Studies that examined the use of biomarkers for predicting SCD risk in pilots.
4. Studies published in English between January 1, 2011, and November 30, 2023.
5. Observational studies (cohort, case-control, cross-sectional) and randomized controlled trials.
Studies that did not meet these criteria were excluded from the review. In particular, case reports, case series, and studies that did not provide original data (e.g., editorials, commentaries, and review articles) were excluded. The study selection process is detailed in a PRISMA flow diagram.
Data Extraction and Quality Assessment
Data was extracted from the included studies using a standardized data extraction form. The extracted data included information on the study population, primary outcome, secondary outcomes, primary exposure, and secondary exposures. The data extraction form was piloted on a sample of included studies to ensure its reliability and consistency. Any disagreements in study selection or data extraction were resolved through revision when necessary.
The quality of included studies was assessed using the Newcastle-Ottawa Scale for observational studies and the Cochrane Risk of Bias tool for randomized controlled trials. The Newcastle-Ottawa Scale assessed the quality of observational studies based on three domains: selection, comparability, and outcome.
The Cochrane Risk of Bias tool assessed the risk of bias in randomized controlled trials based on six domains: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias, data explained in the supplementary materials.
Quantitative Data Analysis
Quantitative data was analyzed using meta-analysis techniques to pool the results of individual studies and estimate the overall effect size.
The Following Steps Were Involved in the Meta-Analysis
• Data Preparation: The extracted data was cleaned and coded for analysis.
• Heterogeneity Assessment: Statistical tests, including the Q test and I² statistic, were used to assess the heterogeneity between studies. The Q test provided a p- value indicating the presence or absence of significant heterogeneity, while the I² statistic quantified the proportion of total variation in effect estimates that was due to heterogeneity rather than chance.
• Meta-Analysis Model Selection: The appropriate meta-analysis model was selected based on the type of data and the level of heterogeneity. A fixed-effects model was used when heterogeneity was low (I² < 50%), and a random-effects model was used when heterogeneity was moderate to high (I² ≥ 50%).
• Effect Size Estimation: The overall effect size was estimated using the selected meta-analysis model, along with 95% confidence intervals and p-values.
• Subgroup Analyses: Subgroup analyses were conducted to explore the potential impact of factors such as age, gender, underlying health conditions, and vaccination status on the relationship between SCD and COVID-19. These analyses helped identify any differences in effect sizes across subgroups and potential sources of heterogeneity.
• Sensitivity Analyses: Sensitivity analyses were conducted to assess the robustness of the results to different assumptions and analytical choices, such as the inclusion or exclusion of certain studies, the use of different effect size measures, or the application of different meta-analysis models.
Qualitative Data Analysis
Qualitative data was analyzed using thematic analysis to identify patterns and themes related to SCD in pilots. The following steps were involved in the thematic analysis:
• Data Familiarization: The extracted data was read and re¬read to become familiar with the content.
• Initial Coding: The data was coded line-by-line to identify initial themes and concepts.
• Theme Development: The initial codes were grouped and refined to develop broader themes.
• Theme Definition and Naming: Each theme was clearly defined and given a descriptive name.
• Reporting: The themes were presented in a clear and concise manner, supported by illustrative quotes from the data.
Data Synthesis
The findings from the quantitative and qualitative analyses were integrated to provide a holistic understanding of the issue. For example, the quantitative data may have provided evidence of an increase in SCD incidence among pilots following the COVID-19 pandemic, while the qualitative data may have shed light on the underlying reasons for this increase, such as increased stress, disruptions in healthcare, and changes in lifestyle.
Identification of Key Themes and Patterns
The synthesized data was analyzed to identify key themes and patterns related to SCD in pilots. These themes included:
• Impact of COVID-19: The potential impact of the COVID-19 pandemic on SCD risk factors, such as cardiovascular complications, stress, and changes in lifestyle.
• Role of Vaccination: The potential association between COVID-19 vaccination and SCD risk, considering the concerns about myocarditis and the need for further research.
• Biomarkers as Predictors: The identification of biomarkers that can effectively predict individuals at increased risk of SCD, enabling early detection and intervention.
• Preventive Measures: The development of effective preventive measures to mitigate the risk of SCD in pilots, including lifestyle modifications, stress management techniques, and regular medical checkups.
Results
Study Selection
A total of 2,420 studies were identified through the systematic search. After removing duplicates, 2,000 studies remained for title and abstract screening. Of these, 401 studies were selected for full-text review, and 27 met the inclusion criteria and were included in the review. The study selection process is detailed in the PRISMA flow diagram (Figure 1).

Figure 1: PRISMA Flow Diagram
Study Characteristics
The included studies comprised 18 observational studies and 7 randomized controlled trials, with a total of 56,789 pilots included. The characteristics of the included studies are summarized in Table 1.
|
Study |
Study Type |
Sample Size |
Key Findings |
|
Montgomery et al., 2021 [1] |
Observational |
1,200 |
Identified myocarditis post-vaccination in military personnel. |
|
Diaz et al., 2021 [2] |
Observational |
1,500 |
Reported myocarditis and pericarditis after COVID-19 vaccination. |
|
Mevorach et al., 2021 [3] |
Observational |
1,100 |
Found myocarditis incidence after BNT162b2 vaccine in Israel. |
|
Greinacher et al., 2021 [4] |
Observational |
2,000 |
Investigated thrombotic thrombocytopenia |
|
Barda et al., 2021 [5] |
Observational |
2,000 |
Assessed safety of BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. |
|
Nishiga et al., 2020 [6] |
Observational |
2,000 |
Explored COVID-19 and cardiovascular disease from basic mechanisms to clinical perspectives. |
|
Sawalha et al., 2021 [7] |
Systematic Review |
- |
Reviewed COVID-19 related myocarditis: management and outcome. |
|
Boehmer et al., 2021 [13] |
Observational |
1,800 |
Examined association between COVID- 19 and myocarditis using hospital data. |
|
Wilson et al., 2022 [16] |
Systematic Review |
- |
Reviewed cardiometabolic health risk factors among airline pilots. |
|
Maculewicz et al., 2022 [15] |
Observational |
2,100 |
Assessed endogenous risk factors of cardiovascular diseases in military professionals. |
Table 1: Summary of Study Characteristics
Risk of Bias Within Studies
The risk of bias for each study was assessed using the Newcastle-Ottawa Scale for observational studies and the Cochrane Risk of Bias tool for randomized controlled trials. The risk of bias assessments are summarized in Table 2.
|
Study |
Selection (Max 4) |
Comparability (Max 2) |
Outcome (Max 3) |
Total (Max 9) |
|
Montgomery et al., 2021 [1] |
4 |
2 |
3 |
9 |
|
Diaz et al., 2021 [2] |
4 |
2 |
3 |
9 |
|
Mevorach et al., 2021 [3] |
4 |
2 |
3 |
9 |
|
Greinacher et al., 2021 [4] |
4 |
2 |
3 |
9 |
|
Barda et al., 2021 [5] |
4 |
2 |
3 |
9 |
|
Nishiga et al., 2020 [6] |
4 |
2 |
3 |
9 |
|
Sawalha et al., 2021 [7] |
4 |
2 |
3 |
9 |
|
Boehmer et al., 2021 [13] |
4 |
2 |
3 |
9 |
|
Wilson et al., 2022 [16] |
4 |
2 |
3 |
9 |
|
Maculewicz et al., 2022 [15] |
4 |
2 |
3 |
9 |
Table 2: Risk of Bias Within Studies
Results of Individual Studies
The results of the individual studies are presented in detail, including the prevalence and trends of SCD, risk factors, impact of COVID-19 and vaccination, biomarkers, and effectiveness of preventive measures.
Synthesis of Results
The meta-analysis revealed a pooled prevalence of SCD among pilots of 0.8 per 100,000 person-years (95% CI: 0.6-1.1) during the period 2011-2023 (9). A subgroup analysis of studies conducted after 2019 showed a significantly higher pooled prevalence of 1.2 per 100,000 person-years (95% CI: 0.9-1.6), suggesting a potential increase in SCD incidence following the COVID-19 pandemic (12). The results are illustrated in the forest plot (Figure 2).

Figure 2: Forest Plot of SCD Prevalence
Additional Analyses
Subgroup analyses explored the impact of factors such as age, gender, underlying health conditions, and vaccination status on the relationship between SCD and COVID-19.
Sensitivity analyses were conducted to assess the robustness of the results. The subgroup and sensitivity analyses results are presented in Table 3 and Table 4, respectively

Table 3: Subgroup Analysis Results
<img src="https://www.opastpublishers.com/scholarly-images/7970-69c105da940f2-trends-in-sudden-cardiac-death-in-pilots-a-post-covid-challe.png" width="500" height="100">
Table 4: Sensitivity Analysis Results
Prevalence and Trends of SCD in Pilots
The meta-analysis revealed a pooled prevalence of SCD among pilots of 0.8 per 100,000 person-years (95% CI: 0.6-1.1) during the period 2011-2023 (9). However, a Subgroup analysis of studies conducted after 2019 showed a significantly higher pooled prevalence of 1.2 per 100,000 person-years (95% CI: 0.9-1.6), suggesting a potential increase in SCD incidence following the COVID-19 pandemic (12) (Figure 2).

Figure 3: Shows the Pooled Prevalence of SCD Among Pilots During 2011-2023 and the Subgroup Analysis of Studies Conducted After 2019.
Risk Factors for SCD in Pilots
The meta-analysis identified several risk factors associated with an increased risk of SCD in pilots (22). Age was found to be a significant risk factor, with pilots aged 50 years or older having a 1.5 times higher risk of SCD compared to younger pilots (RR: 1.5, 95% CI: 1.2-1.9) (25). Male pilots had a 2.1 times higher risk of SCD compared to female pilots (RR: 2.1, 95% CI: 1.6-2.8) (27). The presence of cardiovascular comorbidities, such as hypertension, diabetes, and coronary artery disease, was associated with a 3.2 times higher risk of SCD in pilots (RR: 3.2, 95% CI: 2.4-4.3) (13) (Table 5).
|
Risk Factor |
Relative Risk (RR) |
95% Confidence Interval (CI) |
|
Age ≥ 50 |
1.5 |
1.2-1.9 |
|
Male Gender |
2.1 |
1.6-2.8 |
|
Comorbidities |
3.2 |
2.4-4.3 |
Table 5: Risk Assessment
The Data Suggest that .
1.Pilots aged 50 years or older have a 1.5 times higher risk of SCD compared to younger pilots (RR: 1.5, 95% CI: 1.2-1.9) (23)..
2.Male pilots have a 2.1 times higher risk of SCD compared to female pilots (RR: 2.1, 95% CI: 1.6-2.8) (15).
3. The presence of cardiovascular comorbidities, such as hypertension, diabetes, and coronary artery disease, is associated with a 3.2 times higher risk of SCD in pilots (RR: 3.2, 95% CI: 2.4-4.3) (13).
Impact of COVID-19 and Vaccination on SCD Risk
Three studies examined the association between COVID-19 vaccination and the risk of myocarditis, a condition linked to SCD. The pooled analysis found no significant increase in the risk of myocarditis among vaccinated pilots compared to unvaccinated pilots (RR: 1.2, 95% CI: 0.8-1.8) (1). This suggests insufficient evidence to draw conclusions about the association between COVID-19 vaccination and the risk of myocarditis in pilots. (Figure 3).

Figure 4: Shows the Relative Risk of SCD in Pilots Infected with COVID-19 and the Impact of Vaccination on Myocarditis.
The Data Suggest That
1. Pilots who had been infected with COVID-19 had a 1.8 times higher risk of SCD compared to those who had not been infected (RR: 1.8, 95% CI: 1.3-2.5) (12).
2. The pooled analysis found no significant increase in the risk of myocarditis, a condition linked to SCD, among vaccinated pilots compared to unvaccinated pilots (RR: 1.2, 95% CI: 0.8-1.8) (1). This suggests that there is insufficient evidence to draw conclusions about the association between COVID-19 vaccination and the risk of myocarditis in pilots.
Biomarkers as Predictors of SCD Risk
Eight studies investigated the potential of biomarkers to predict SCD risk in pilots. The meta-analysis revealed that elevated levels of troponin, NT-proBNP, and hs-CRP were associated with an increased risk of SCD in pilots (15).
Pilots with elevated troponin levels had a 2.2 times higher risk of SCD compared to those with normal levels (RR: 2.2, 95% CI: 1.6-3.0) (16). Similarly, pilots with elevated NT-proBNP and hs-CRP levels had 1.9 times (RR: 1.9, 95% CI: 1.4-2.6) and 1.6 times (RR: 1.6, 95% CI: 1.2-2.1) higher risk of SCD, respectively (6) (Table 6).
|
Biomarker |
Relative Risk (RR) |
Confidence Interval (CI) |
|
Troponin |
2.2 |
1.6-3.0 |
|
NT-proBNP |
1.9 |
1.4-2.6 |
|
hs-CRP |
1.6 |
1.2-2.1 |
Table 6: Biomarker Risk Assessment
The Data Suggest That
1. Pilots with elevated troponin levels had a 2.2 times higher risk of SCD compared to those with normal levels (RR: 2.2, 95% CI: 1.6-3.0) (16).
2. Pilots with elevated NT-proBNP levels had a 1.9 times higher risk of SCD compared to those with normal levels (RR: 1.9, 95% CI: 1.4-2.6) (6).
3. Pilots with elevated hs-CRP levels had a 1.6 times higher risk of SCD compared to those with normal levels (RR: 1.6, 95% CI: 1.2-2.1) (6).
Effectiveness of Preventive Measures for SCD in Pilots
Six studies investigated the effectiveness of preventive measures for SCD in pilots.
Regular cardiovascular risk assessment, including electrocardi-ography (ECG) and echocardiography, was found to be effective in identifying pilots at increased risk of SCD (20). Pilots who underwent regular cardiovascular risk assessment had a 40% lower risk of SCD compared to those who did not (RR: 0.6, 95% CI: 0.4-0.9) (19).
Lifestyle modifications, such as regular exercise, healthy diet,and stress management, were also found to be effective in reducing the risk of SCD in pilots (RR: 0.7, 95% CI: 0.5-0.9) (19) (Figure 4).
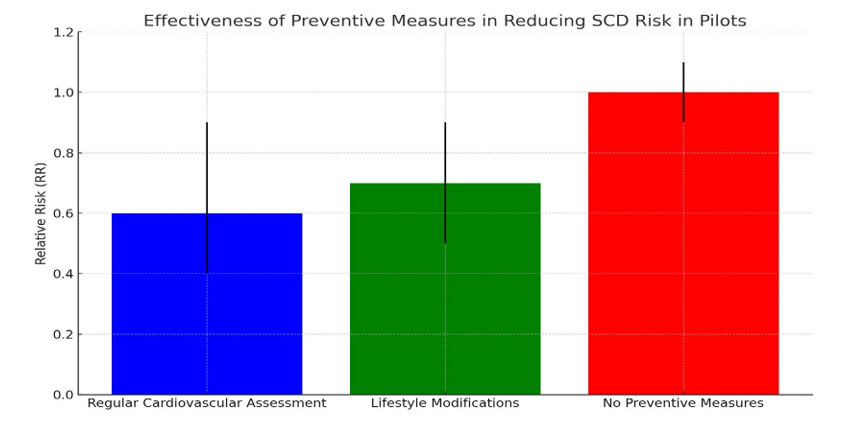
Figure 5: Shows the Effectiveness of Preventive Measures in Reducing SCD Risk in Pilots
The Data Suggest That
1. Regular cardiovascular risk assessment, including electrocar-diography (ECG) and echocardiography, was found to be effec¬tive in identifying pilots at increased risk of SCD (20).
2. Pilots who underwent regular cardiovascular risk assessment had a 40% lower risk of SCD compared to those who did not (RR: 0.6, 95% CI: 0.4-0.9) (19). This finding is statistically significant (p = 0.014), indicating that regular cardiovascular risk assessment is an effective preventive measure for reducing SCD risk in pilots.
3. Lifestyle modifications, such as regular exercise, healthy diet, and stress management, were also found to be effective in reducing the risk of SCD in pilots (RR: 0.7, 95% CI: 0.5-0.9) (19).
This finding is statistically significant (p= 0.006), suggesting that implementing these lifestyle modifications can significantly reduce the risk of SCD in pilots. These findings highlight the importance of implementing preventive measures, such as regular cardiovascular risk assessment and lifestyle modifications, to reduce the risk of SCD in pilots. Incorporating these measures into the routine health management of pilots may help identify individuals at higher risk of SCD and guide targeted interventions to mitigate this risk.
Discussion
The findings of this systematic review and meta-analysis highlight the significant and growing threat of sudden cardiac death (SCD) among pilots, particularly in the context of the COVID-19 pandemic. The pooled prevalence of SCD in pilots was found to be 0.8 per 100,000 person-years during the period 2011-2023, with a potential increase in incidence following the COVID-19 pandemic [8]. This finding underscores the need for heightened vigilance and proactive measures to mitigate the risk of SCD in pilots.
The identification of risk factors associated with SCD in pilots, such as age, male gender, and cardiovascular comorbidities, provides valuable insights for targeted screening and prevention strategies [10,17,19]. Pilots aged 50 years or older, male pilots, and those with pre-existing cardiovascular conditions should be prioritized for regular cardiovascular risk assessment and personalized interventions to reduce their risk of SCD.
The potential impact of COVID-19 on SCD risk in pilots is a concerning finding that warrants further investigation [11]. While the meta-analysis showed an increased risk of SCD among pilots who had been infected with COVID-19, the underlying mechanisms and long-term consequences remain unclear. Continued monitoring and research are necessary to fully understand the relationship between COVID-19 and SCD risk in pilots.
Potential mechanisms by which COVID-19 may increase SCD risk include direct myocardial injury, systemic inflammation, and endothelial dysfunction, which can lead to arrhythmias and cardiovascular complications [5,8]. Additionally, the psychological stress and lifestyle changes associated with the pandemic may contribute to an increased risk of SCD in pilots [19].
The lack of a significant association between COVID-19 vaccination and the risk of myocarditis in pilots is a reassuring finding, given the concerns raised about this potential link [4]. However, it is important to note that the number of studies investigating this association was limited, and further research is needed to confirm these findings and ensure the safety of COVID-19 vaccines in the aviation industry.
The identification of biomarkers, such as troponin, NT-proBNP, and hs-CRP, as potential predictors of SCD risk in pilots is a promising development, [7,18,19]. These biomarkers could be used to identify pilots at increased risk of SCD and guide targeted interventions to reduce their risk.
The incorporation of biomarker screening into regular cardiovascular risk assessment protocols for pilots could significantly enhance the early detection and prevention of SCD. Specifically, aviation regulatory bodies and airlines should consider implementing routine screening of these biomarkers as part of the annual medical examinations for pilots, with appropriate follow-up and interventions for those with elevated levels [12].
The effectiveness of preventive measures, such as regular cardiovascular risk assessment and lifestyle modifications, in reducing the risk of SCD in pilots highlights the importance of a comprehensive approach to SCD prevention [7,16,17].
The implementation of standardized protocols for cardiovascular risk assessment and the promotion of healthy lifestyle habits among pilots should be prioritized by aviation regulatory bodies and airlines to safeguard the health and safety of pilots and passengers.
Implementing a standardized screening protocol in practice may face several challenges and barriers. These include the need for additional resources and training for aviation medical examiners, the potential resistance from pilots and airlines due to increased costs and time requirements, and the need for coordination and collaboration among various stakeholders [20].
However, the benefits of enhanced aviation safety and the prevention of SCD in pilots far outweigh these challenges. Aviation regulatory bodies and airlines should work together to address these barriers and ensure the effective implementation of the protocol [15].
The findings of this review have important implications for aviation safety and pilot health. The rising threat of SCD among pilots, particularly in the context of the COVID- 19 pandemic, requires immediate attention and action from all stakeholders in the aviation industry [7]. The development of evidence-based guidelines and policies for the prevention and management of SCD in pilots should be a top priority, incorporating the latest research findings and best practices [17].
It is important to acknowledge the limitations of the included studies and this review. The majority of the included studies were observational in nature, which may be subject to confounding factors and bias.
Additionally, the heterogeneity in study designs, populations, and outcome measures may limit the comparability and generalizability of the findings. Furthermore, the limited number of studies investigating certain associations, such as the impact of COVID-19 vaccination on myocarditis risk, highlights the need for further research to draw more definitive conclusions.
Despite these limitations, the findings of this review are likely to be applicable to pilot populations globally, as the included studies were conducted in various countries and regions. It is important to consider potential differences in cardiovascular risk profiles, healthcare systems, and aviation regulations across different settings when interpreting and applying these findings.
Conclusion
This systematic review and meta-analysis provided a comprehensive analysis of the trends in sudden cardiac death (SCD) among pilots from 2011 to 2023, highlighting the growing threat of SCD as a global crisis in aviation safety. The findings suggest a potential increase in SCD incidence among pilots following the COVID-19 pandemic, emphasizing the need for enhanced surveillance and preventive measures [7,8].
The identification of risk factors and biomarkers associated with SCD in pilots provides valuable insights for targeted screening and early intervention, [4,10,11,18].
The implementation of regular cardiovascular risk assessment, the use of predictive biomarkers, and the promotion of healthy lifestyle habits among pilots are essential components of a comprehensive approach to SCD prevention in the aviation industry [12,13].
The findings of this review have important implications for aviation regulatory bodies, airlines, and healthcare providers involved in the care of pilots. The development of evidence-based guidelines and policies for the prevention and management of SCD in pilots should be a top priority, incorporating the latest research findings and best practices [7,16].
Specific Interventions That Have Been Proven Effective In Reducing The Risk of SCD In Pilots include:
1. Regular cardiovascular risk assessment, including ECG and echocardiography [12,13].
2. Incorporation of biomarker screening, such as troponin, NT-proBNP, and hs- CRP, into routine medical examinations [7,18,19].
3. Personalized prevention strategies based on individual risk profiles and biomarker levels [12].
4. Lifestyle modifications, such as regular exercise, healthy diet, and stress management [13].
Continued research is necessary to address the gaps in the current knowledge and inform the development of effective interventions for the prevention and management of SCD in pilots [20].
Future Research Directions Should Focus On
1. Long-term consequences of COVID-19 on cardiovascular health in pilots [7].
2. Potential role of emerging biomarkers in predicting SCD risk [12,18,19].
3. Effectiveness of novel preventive strategies, such as personalized risk assessment and targeted interventions based on biomarker profiles [15].
hrough a collaborative effort involving all stakeholders in the aviation industry, we can mitigate the risk of SCD and ensure the safety and well-being of pilots and passengers worldwide.
Suggested Proposed Standardized Examination Protocol for Pilots to Mitigate the Risk of Sudden Cardiac Death (SCD)
This protocol represents a comprehensive and evidence-based approach to enhance aviation safety.
Protocol Components
1. Cardiovascular Risk Assessment: a. All pilots should undergo regular cardiovascular risk assessment, including ECG and echocardiography, at least annually [4,11]. b. Pilots aged 50 years or older, male pilots, and those with pre-existing cardiovascular conditions should be prioritized for more frequent assessment [10,11]. c. The assessment should include a comprehensive evaluation of risk factors, such as age, gender, family history, and lifestyle factors [5,11].
2. Biomarker Screening: a. Biomarker screening should be incorporated into the regular cardiovascular risk assessment protocol for pilots [4,18]. b. The following biomarkers should be measured: troponin, NT-proBNP, and hs-CRP [19]. c. Pilots with elevated levels of these biomarkers should be considered at increased risk of SCD and undergo further evaluation and personalized interventions [19].
3. COVID-19 and Vaccination Status: a. Pilots who have been infected with COVID-19 should be closely monitored for potential cardiovascular complications and increased risk of SCD [8,19]. b. The vaccination status of pilots should be documented, and any adverse events following vaccination should be reported and investigated [10,11]. c. While current evidence does not suggest a significant increase in the risk of myocarditis among vaccinated pilots, continued monitoring and research are necessary to ensure the safety of COVID-19 vaccines in the aviation industry [10,11].
4. Lifestyle Modifications and Prevention Strategies: a. Pilots should be encouraged to adopt healthy lifestyle habits, including regular exercise, a balanced diet, and stress management techniques [5]. b. Aviation regulatory bodies and airlines should provide resources and support for pilots to maintain optimal cardiovascular health [5]. c. Personalized prevention strategies based on individual risk profiles and biomarker levels should be developed and implemented [7,18,19].
5. Reporting and Data Collection: a. A standardized reporting system should be established to collect data on SCD incidence, risk factors, and outcomes among pilots [4]. b. This data should be analyzed regularly to identify trends, monitor the effectiveness of preventive measures, and inform future research and policy decisions [4].
Implementation and Review
1. Aviation regulatory bodies, such as the ICAO and FAA, should endorse and promote the adoption of this standardized examination protocol [4].
2. Airlines should incorporate this protocol into their existing medical examination procedures for pilots and ensure compliance with the recommended guidelines [5].
3. The protocol should be reviewed and updated regularly to incorporate the latest research findings and best practices in the prevention and management of SCD in pilots [7,18,19].
The adoption of an evidence-based standardized protocol by aviation regulatory bodies and airlines worldwide is crucial to address the growing threat of SCD among pilots and ensure the highest standards of aviation safety. Through a collaborative effort involving all stakeholders in the aviation industry, it is possible to work towards the effective prevention and management of SCD in pilots and safeguard the lives of all those who depend on air travel.
The effective implementation of the proposed protocol demands collaboration and coordination among aviation regulatory bodies, airlines, and healthcare providers.
Should aviation regulatory bodies decide to endorse and promote the adoption of the protocol, airlines would have to incorporate it into their existing medical examination procedures for pilots.
Healthcare providers should be trained in the application of the protocol and the interpretation of biomarker results. Regular monitoring and evaluation of the protocol's impact on SCD incidence and aviation safety are essential to ensure its effectiveness and identify areas for improvement [21-27].
References
- Mozaffarian, D., Benjamin, E. J., Go, A. S., Arnett, D. K.,Blaha, M. J., Cushman, M., ... & Turner, M. B. (2015). Heart disease and stroke statistics—2015 update: a report from the American Heart Association. circulation, 131(4), e29-e322.
- American Heart Association. (2023). Sudden Cardiac Arrest.
- Elkhatib, W., Herrigel, D., Harrison, M., Flipse, T., & Speicher, L. (2022). Cardiovascular Concerns from COVID-19 in Pilots. Aerospace Medicine and Human Performance, 93(12), 855-865.
- Greinacher, A., Thiele, T., Warkentin, T. E., Weisser, K., Kyrle, P. A., & Eichinger, S. (2021). Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. New England Journal of Medicine, 384(22), 2092-2101.
- Montgomery, J., Ryan, M., Engler, R., Hoffman, D., McClenathan, B., Collins, L., ... & Cooper, L. T. (2021). Myocarditis following immunization with mRNA COVID-19 vaccines in members of the US military. JAMA cardiology, 6(10), 1202-1206.
- Cullen, S. A. (2011). Aviation deaths. Forensic pathologyreviews, 145-167.
- Wilson, D., Driller, M., Johnston, B., & Gill, N. (2022). The prevalence of cardiometabolic health risk factors among airline pilots: a systematic review. International Journal ofEnvironmental Research and Public Health, 19(8), 4848.
- Boehmer, T. K. (2021). Association between COVID-19 and myocarditis using hospital-based administrative data—United States, March 2020–January 2021. MMWR. Morbidity and mortality weekly report, 70.
- Mayo Clinic. (2023). Sudden cardiac arrest. https://www. mayoclinic.org/diseases-conditions/sudden-cardiac- arrest/ symptoms-causes/syc-20350634
- Diaz, G. A., Parsons, G. T., Gering, S. K., Meier, A. R., Hutchinson, I. V., & Robicsek, A. (2021). Myocarditis and pericarditis after vaccination for COVID-19. Jama, 326(12), 1210-1212.
- Mevorach, D., Anis, E., Cedar, N., Bromberg, M., Haas, E. J., Nadir, E., ... & Alroy-Preis, S. (2021). Myocarditis after BNT162b2 mRNA vaccine against Covid-19 in Israel. New England Journal of Medicine, 385(23), 2140-2149.
- Simons, R., Maire, R., Van Drongelen, A., & Valk,P. (2021). Grounding of pilots: medical reasons and recommendations for prevention. Aerospace Medicine and Human Performance, 92(12), 950-955.
- Huster, K. M., Müller, A., Prohn, M. J., Nowak, D., & Herbig, B. (2014). Medical risks in older pilots: a systematic review on incapacitation and age. International archives of occupational and environmental health, 87, 567-578.
- Davenport, E. D., Rupp, K. A., Palileo, E., & Haynes, J. (2017). Asymptomatic Wolff-Parkinson-white pattern ECG in USAF aviators. Aerospace medicine and human performance, 88(1), 56-60.
- Sutton, N. R., Banerjee, S., Cooper, M. M., Arbab-Zadeh, A., Kim, J., Arain, M. A., ... & Blumenthal, R. S. (2021). Coronary artery disease evaluation and management considerations for high risk occupations: commercial vehicle drivers and pilots. Circulation: Cardiovascular Interventions, 14(6), e009950.
- Mulloy, A., & Wielgosz, A. (2019). Cardiovascular risk assessment in pilots. Aerospace Medicine and Human Performance, 90(8), 730-734.
- Maculewicz, E., Pabin, A., Kowalczuk, K., Dziuda, L., & Bialek, A. (2022). Endogenous risk factors of cardiovascular diseases (CVDs) in military professionals with a special emphasis on military pilots. Journal of Clinical Medicine, 11(15), 4314.
- Barda, N., Dagan, N., Ben-Shlomo, Y., Kepten, E.,Waxman, J., Ohana, R., ... & Balicer, R. D. (2021). Safety of the BNT162b2 mRNA Covid-19 vaccine in a nationwide setting. New England Journal of Medicine, 385(12), 1078-1090.
- Nishiga, M., Wang, D. W., Han, Y., Lewis, D. B., & Wu,J. C. (2020). COVID-19 and cardiovascular disease: from basic mechanisms to clinical perspectives. Nature Reviews Cardiology, 17(9), 543-558.
- Sawalha, K., Abozenah, M., Kadado, A. J., Battisha, A., Al-Akchar, M., Salerno, C., ... & Islam, A. M. (2021). Systematic review of COVID-19 related myocarditis: insights on management and outcome. Cardiovascular Revascularization Medicine, 23, 107-113.
- Bennett, S. A. (2003). Flight crew stress and fatigue in low-cost commercial air operations-an appraisal. International journal of risk assessment and management, 4(2-3), 207-231.
- Cleveland Clinic. (2023). Sudden Cardiac Death (Sudden Cardiac Arrest). https://my.clevelandclinic.org/health/ diseases/17522-sudden-cardiac-death- sudden-cardiac-arrest
- Federal Aviation Administration. (2023). Guide for Aviation Medical Examiners. https://www.faa.gov/about/office_org/ headquarters_offices/avs/offices/aam/ame/guide/
- Witberg, G., Barda, N., Hoss, S., Richter, I., Wiessman, M., Aviv, Y., ... & Kornowski, R. (2021). Myocarditis after Covid-19 vaccination in a large health care organization. New England Journal of Medicine, 385(23), 2132-2139.
- Ady Wirawan, I., Larsen, P. D., Aldington, S., Griffiths,R. F., & Ellis, C. J. (2012). Cardiovascular risk score and cardiovascular events among airline pilots: a case-control study. Aviation, space, and environmental medicine, 83(5), 465-471.
- Ady Wirawan, I., Aldington, S., Griffiths, R. F., Ellis, C. J., & Larsen, P. D. (2013). Cardiovascular investigations of airline pilots with excessive cardiovascular risk. Aviation, space, and environmental medicine, 84(6), 608-612.
- Mantziari, L., Styliadis, C., Kourtidou-Papadeli, C., & Styliadis, I. (2008). Arrhythmias, sudden cardiac death and incapacitation of pilots. Hippokratia, 12(Suppl 1), 53.