
International Journal of Orthopaedics Research(IJOR)
ISSN: 2690-9189 | DOI: 10.33140/IJOR
Impact Factor: 1.6

Research Article - (2026) Volume 9, Issue 1
Traumatic Patellar Tendon Rupture: Does Acute Surgical Treatment Matter?
Received Date: Dec 05, 2025 / Accepted Date: Jan 02, 2026 / Published Date: Jan 16, 2026
Copyright: ©2026 Naser Fuad Shari, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Jwinate, M. N., Aolymate, M. K. A. A., Alawamleh, A. A., Alsaaideh, M. A., Hawawsheh, M. J. A., et al. (2026). Traumatic Patellar Tendon Rupture: Does Acute Surgical Treatment Matter?. Int J Ortho Res, 9(1), 01-05.
Abstract
Background: While acute patellar tendon tears are usually straightforward to identify, they can sometimes be ignored in clinical practice. This article conducted to examine both immediate and long-term results of surgical management in patients with acute patellar tendon injuries. It was hypothesized to identify if surgery would enable most individuals to recover pre-injury knee function.
Methods: In this retrospective review, 31 knees from 29 patients (27 men, 2 women; average age 36.8 ± 7.3 years, range 19–75) were analyzed. Level of injuries was 12 mid-tendon ruptures, 17 tears at the patellar end, and 2 at the tibial attachment. About 97% of repairs were augmented with additional support—using hamstring tendon autografts (17 cases), synthetic ligaments (10 cases), or metal wires (3 cases).
- Early outcomes were identified at an average of 9.1 months duration post-surgery (range 4–18 months), focusing on complications, joint range of motion, and radiological findings.
- Long-term outcomes were obtained through phone calls or interviews at an average of 8.1 years (range 19–246 months), using the Lysholm functional score and patients’ satisfaction.
Results: At the early follow-up, 27 knees were assessed, showing an average knee flexion of 125.5° ± 9.5° (range 65°– 135°) and an average extension lag of −10° (range −15° to 0°). The mean Caton-Deschamps index was 0.93 (range 0.68–1.25). For the long-term follow-up (19 knees), the average Lysholm score was 89.5 (range 61–100). About 94% of patients were either satisfied or very satisfied with their outcome. All studied patients were able to resume their previous work, and 16 resumed sports, with 7 reaching their pre-injury level.
Conclusion: Early surgical repair of acute patellar tendon rupture, the outcome is excellent, with most patients returning to pre-injury level of function and reporting high satisfaction
Keywords
Patellar Tendon Rupture, Patella Alta, Trans Osseous Tunnelling, Anchor Fixation, Lysholm Score, Patients’ Satisfaction.
Level of Evidence
IV – Retrospective case series
Introduction
Patellar tendon ruptures are uncommon, happening about one- fifth as often as patellar fractures. While quadriceps tendon tears are typically seen in older adults, patellar tendon injuries are more likely to impact active individuals in their thirties. These ruptures generally result from an indirect force, such as a powerful contraction of the quadriceps muscle when the knee is slightly bent common during activities like running, jumping, or trying to break a fall [1,2].
It’s rare for a completely healthy patellar tendon to tear. Most of these injuries occur when the tendon has already been compromised by ongoing stress, degeneration, frequent steroid injections or renal dystrophies. Clinically, the most telling sign is an inability to do straight leg raise, though even with this symptom, the injury can sometimes be overlooked in emergency settings [3].
While there are well-defined protocols for treating acute patellar tendon ruptures, there is still a no enough data on long-term outcomes after surgical management [4,5]. This study aims to address this gap.
Methods
In this study group, 17 patients were classified as overweight or obese, with 5 falling into the category of grade 1 obesity or higher. 8 patients (26%) had existing risk factors, including 3 patients with known patellar tendinopathies, 2 patients who had recently received steroid injections, and one each with gout, diabetes, or a history of long-term steroid use. The majority of injuries were related to sports activities (17 cases, 56%), followed by accidents at home (6 cases, 20%), traffic accidents (3 cases, 10%), and work-related incidents (3 cases, 10%). The average time from injury to surgery was about 3.5 days (ranging from the day of injury up to 2 weeks); cases with longer delays were not included in the study. 2.1. Imaging: X-rays taken from the front and side with the knee bent between 20° and 30° showed evidence of tendon rupture in all but one patient. Only four had a normal Caton-Deschamps index, while five showed early signs of joint degeneration—two of which affected the femoropatellar region. Tabel 1 – Figure 1 + 2
|
|
Number (%) |
|
Patella Alta |
25 (80) |
|
Bone avulsion |
8 (27) |
|
Patellar tip |
17(54) |
|
Tibial tuberosity |
2 (7) |
|
indirect radiologic sign |
28 (91) |
|
Mean Caton-Deschamps index |
0.93 (range 0.68–1.25) |
Table 1: Radiologic Signs at Admission
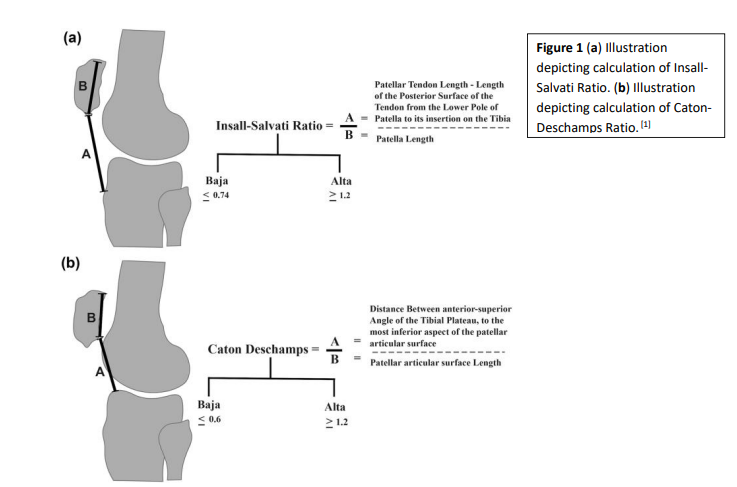

Figure 2: Caton-Deschamps Index (CDI) measurement from sagittal MRI slice with the greatest length of the patella. The CDI equals the distance from the distal aspect of the patellar articular cartilage to the anterosuperior corner of the tibial joint surface (blue line in A), divided by the length of the cartilaginous articular surface (yellow line in B) [6]
Surgical Technique
Patients were positioned on their backs, a tourniquet was applied, and the knee was bent between 45° and 90°. For the 12 mid-tendon ruptures, surgeons used end-to-end absorbable sutures. Of the 17 avulsions from the patellar end, 15 were repaired using sturdy non- absorbable sutures threaded through vertical tunnels in the patella, whereas the three most recent cases were fixed using metal anchors. The two avulsions from the tibial tuberosity were addressed with either thick absorbable sutures or metal anchors [4,5,7].
Additional reinforcement was provided in 29 cases—3 with metal wires (mostly early in the series), 10 with synthetic ligaments, and 16 with hamstring tendon grafts (either gracilis or semitendinosus). Fluoroscopy was routinely used to ensure proper patellar height, aiming for a Caton-Deschamps index close to 1 whenever possible [8]. Table 2
|
|
Avulsion of patella tip (%) |
Mid-tendon rupture (%) |
Avulsion at TT (%) |
Total (%) |
|
Number of knees |
17 (55) |
12 ( 39) |
2 ( 6) |
31 (100) |
|
Type of repair |
|
|
|
|
|
1. End-to-end suture |
0 |
12 |
0 |
12 |
|
2. Transosseous reinsertion |
15 |
0 |
0 |
15 |
|
3. Reinsertion by anchors |
2 |
0 |
1 |
3 |
|
4. Fixation by staples |
0 |
0 |
1 |
1 |
|
Protection frame |
|
|
|
|
|
1. Hamstring |
7 |
7 |
2 |
16 |
|
2. Metal wire |
2 |
0 |
1 |
3 |
|
3. Synthetic ligament |
5 |
4 |
1 |
10 |
|
4. No protection |
2 |
0 |
0 |
2 |
Table 2: Surgical techniques
Post- Surgical Care:
After the operation, the affected leg was placed in a cast that allowed the patient to walk for at least six weeks. This was typically followed by a removable brace until the patient could achieve full and pain-free knee extension, usually after an additional two to four weeks.
Follow-Up:
Patients were monitored at 15 days, 45 days, and again at three months to check on healing, watch for complications, and assess knee movement.
Early Complication and Functional Outcomes
An independent assessor gathered the data, including follow-up phone interviews. Evaluations included comparing knee movement between both legs, assessing pain, the ability to return to work, and participation in sports. Functional status was measured using the Lysholm score, and patients also rated their satisfaction with the outcome [9].
Statistical analysis was performed using R software, with a significance threshold set at P < 0.05
Results
Complication (n = 31):
Among the 31 cases reviewed, one 25-year-old patient with no identifiable risk factors sadly passed away from a major pulmonary embolism 15 days after surgery and another one passed from acute pancreatitis 2 months after his surgery. Three other patients (9.6%) experienced minor skin-related issues: one developed a superficial wound that healed with basic care, another had a skin tear caused by a broken metal wire frame (which resolved once the wire was removed), and the third experienced skin necrosis but recovered after receiving negative-pressure wound therapy. There were no cases of infection, and antibiotics were not required for any patient.
Additionally, one individual needed a second operation after suffering a new injury from a fall two months post-surgery. For this re-rupture, the surgical team used a hamstring tendon graft, resulting in a good final outcome.
Short- Term Outcomes (n = 27):
The surgical team directly evaluated 27 knees, while the other cases were followed elsewhere. The average follow-up period was 9.1 months duration post-surgery (range 4–18 months). Notably, two patients who were only three months out from surgery had already regained full mobility in their knees.
At the early follow-up, 27 knees were assessed, showing an average knee flexion of 125.5° ± 9.5° (range 65°–135°) and an average extension lag of −10° (range −15° to 0°). The mean Caton- Deschamps index was 0.93 (range 0.68–1.25). One of the patients with the most limited knee bending (85°) was the oldest in the group and had severe pre-existing arthritis. Among those unable to bend their knee past 100°, one had a history of patellofemoral arthritis, while the other was a younger, otherwise healthy man who’d received a hamstring graft. On average, patients had extension lag of −10° (range −15° to 0°), and about 10% could not fully straighten their knee. Importantly, none of the patients reported ongoing pain.
X-rays revealed that three knees (10%) had some widening of the bone tunnels, but this did not seem to affect how the knees functioned. The average Caton-Deschamps index (CDI) was 0.91, with values ranging from 0.57 to 1.29. Two knees had a lower- than-normal patellar position (CDI < 0.6), while two others were higher than normal (CDI > 1.2); however, these variations did not negatively impact patient outcomes. No progression of joint degeneration was seen during the follow-up period. Table 3.
|
Number of patients: 27 |
Results at a mean 9.1 months |
|
Mean flexion |
125.5° ± 9.5° (range 65°–135°) |
|
Active extension lag |
−10â?¦ (−15â?¦ to 0â?¦) |
|
Complete active extension |
24 (90%) |
|
Pain |
0 |
|
Caton-Deschamps index |
0.93 (range 0.68–1.25) |
|
Tunnel enlargement |
3 (10%) |
Table 3: Short-Term Outcomes
Long – Term Outcomes (n = 25):
Long-term follow-up was conducted via phone interviews with 25 patients, as some could not be reached and one had died from acute pancreatitis. On average, patients were followed for about 8.1 years (range 19–246 months). The average Lysholm score was 94.9, reflecting very good knee function. Twenty-two of these patients were able to resume sports, with several returning to their previous level of activity.
Statistical analysis showed no significant relationship between functional outcome or return to sports and factors such as age, body mass index (BMI), or use of hamstring grafts for reinforcement. Table 4
|
Number 0f patients: 25 |
Results at a mean 10.1 years |
|
Flexion symmetry with healthy side |
21 (82 %) |
|
Extension symmetry with healthy side |
24 (96 %) |
|
Pain |
3 (12 %) |
|
Mean Lysholm score |
94.9 points (61–100) |
|
Excellent: 98–100 |
13 (54%) |
|
Very good: 93–97 |
6 (24%) |
|
Good: 82–92 |
4 (16 %) |
|
Moderate: 66–81 |
1 (3%) |
|
Poor: < 65 |
1 (3%) |
|
Return to sport |
22 (88%) |
|
At previous level |
9 (36%) |
|
Lower level |
10 (40%) |
|
Return to work |
25 (100%) |
|
Subjective satisfaction |
|
|
Very satisfied |
13 (53%) |
|
Satisfied |
11 (43%) |
|
Moderately satisfied |
1 (4%) |
|
Dissatisfied |
0 |
Table 4: Long-Term Outcomes
Discussion
With a nearly ten-year average follow-up, this study found outstanding results—patients achieved a mean Lysholm score of 94.9 points out of 100, and 96% reported being satisfied or highly satisfied with their outcomes. The extended follow-up period is a major strength of this research. However, some limitations should be noted: the number of cases was relatively modest, the study was conducted at a single center, and the design was retrospective. About a quarter of patients were lost to long-term follow-up, but every patient who could be reached agreed to participate. Because follow-up at later stages was done by phone, new radiographic data could not be collected [10,11]. The vast majority of patients in this study were men (93%), which is consistent with findings from other large studies. Other research has also shown a similar male predominance, though the average age in those studies tends to be slightly higher than in this group. Several patients in this study had known risk factors for tendon rupture, such as multiple steroid injections or existing tendon degeneration [12,13].
Overall, these results align closely with previous long-term studies, which have also reported high levels of patient satisfaction and strong rates of returning to sports following surgical repair.
When it comes to surgical technique for tears in the middle of the patellar tendon, surgeons usually use end-to-end suturing. When the tendon tears away from the patella, the repair can be done using either suture anchors or trans osseous sutures, with no clear evidence that one approach is better than the other. Reinforcement—whether with hamstring tendon grafts, strong non-absorbable sutures, or metal wires—is commonly used to add strength to the repair, as supported by biomechanical studies [14,15].
In this study, the use of hamstring tendon grafts for reinforcement became more common over time. These grafts are relatively easy to obtain and help avoid the complications sometimes seen with metal wires. The repair methods evolved over the study period, shifting from metal wires to synthetic ligaments and, eventually, to a preference for hamstring tendons. Many previous studies support starting knee movement early after surgery, and in this group, over 80% of patients regained a near-normal range of motion. This is consistent with the literature. While immobilizing the knee after surgery can help protect the repair, it may also result in limited extension and muscle weakness, especially if rehabilitation is not followed as prescribed.
Conclusion
Early follow-up showed that most patients regained good movement, with an average knee bend of 125.5° ± 9.5° (range 65°–135°), and extension lag averaging ten degrees. The Caton- Deschamps index suggesting satisfactory patellar alignment. long-term follow-up Lysholm score indicating satisfactory knee function overall. The vast majority of patients reported being happy or very happy with their progress. Everyone was able to get back to work, and most returned to sports, with nine reaching the same level they had before their injury.
Overall, these results show that prompt surgical repair of acute patellar tendon injuries leads to excellent recovery, high patient satisfaction, and a strong likelihood of returning to previous activity levels—both at work and in sports.
References
- Kannus, P. E. K. K. A., & Jozsa, L. (1991). Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 891 patients. JBJS, 73(10), 1507-1525.
- Kelly, D. W., Carter, V. S., Jobe, F. W., & Kerlan, R. K. (1984). Patellar and quadriceps tendon ru p tures—jumper's knee. The American journal of sports medicine, 12(5), 375-380.
- Greis, P. E., Holmstrom, M. C., & Lahav, A. (2005). Surgical treatment options for patella tendon rupture, part I: acute. Orthopedics, 28(7), 672-679.
- Lee, D., Stinner, D., & Mir, H. (2013). Quadriceps and patellar tendon ruptures. The journal of knee surgery, 26(05), 301-308.
- Caton, J., Deschamps, G., Chambat, P., Lerat, J. L., & Dejour,H. (1982). Patella infera. Apropos of 128 cases. Revue de chirurgie orthopedique et reparatrice de l'appareil moteur, 68(5), 317-325.
- Brutico, J., Paul, R. W., Wright, M., Destine, H., Johnson,E. E., Bishop, M. E., ... & Tjoumakaris, F. P. (2023). Preoperative patella alta on Caton-Deschamps index is a predictor of outcome following isolated medial patellofemoral ligament reconstruction. Arthroscopy, Sports Medicine, and Rehabilitation, 5(2), e523-e528.
- Marder, R. A., & Timmerman, L. A. (1999). Primary repair of patellar tendon rupture without augmentation. The American journal of sports medicine, 27(3), 304-307.
- Kasten, P., Schewe, B., Maurer, F., Gösling, T., Krettek, C., & Weise, K. (2001). Rupture of the patellar tendon: a review of 68 cases and a retrospective study of 29 ruptures comparing two methods of augmentation. Archives of orthopaedic and trauma surgery, 121(10), 578-582.
- Bhargava, S. P., Hynes, M. C., & Dowell, J. K. (2004).Traumatic patella tendon rupture: early mobilisation following surgical repair. Injury, 35(1), 76-79.
- West, J. L., Keene, J. S., & Kaplan, L. D. (2008). Early motion after quadriceps and patellar tendon repairs: outcomes with single-suture augmentation. The American journal of sports medicine, 36(2), 316-323.
- Boudissa, M., Roudet, A., Rubens-Duval, B., Chaussard, C., & Saragaglia, D. (2014). Acute quadriceps tendon ruptures: a series of 50 knees with an average follow-up of more than 6 years. Orthopaedics & Traumatology: Surgery & Research, 100(2), 217-220.
- Ettinger, M., Dratzidis, A., Hurschler, C., Brand, S., Calliess, T., Krettek, C., ... & Petri, M. (2013). Biomechanical properties of suture anchor repair compared with transosseous sutures in patellar tendon ruptures: a cadaveric study. The American journal of sports medicine, 41(11), 2540-2544.
- Bushnell, B. D., Byram, I. R., Weinhold, P. S., & Creighton, R.A. (2006). The use of suture anchors in repair of the ruptured patellar tendon: a biomechanical study. The American Journal of Sports Medicine, 34(9), 1492-1499.
- Bushnell, B. D., Tennant, J. N., Rubright, J. H., & Creighton,R. A. (2008). Repair of patellar tendon rupture using suture anchors. The journal of knee surgery, 21(02), 122-129.
- Vella-Baldacchino, M., Cipolla, A., Asghar, Z., LiArno, S., Faizan, A., Argenson, J. N., & Ollivier, M. (2025). Patella height ratios diagnose the same healthy knees differently. Scientific Reports, 15(1), 89.