
Japanese Journal of Medical Science(JJMS)
ISSN: 2996-2536 | DOI: 10.33140/JJMS

Case Report - (2024) Volume 2, Issue 2
Total Occlusion of the Left Coronary Main Trunk with Medical Treatment and 4-Year Survival
2Radiology CEO CT Scanner Group, Mexico
Received Date: Aug 20, 2024 / Accepted Date: Sep 25, 2024 / Published Date: Oct 09, 2024
Copyright: ©©2024 Jose F. Guadalajara Boo, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Guadalajara Boo, J, F., Hayama, K, E. (2024). Total Occlusion of the Left Coronary Main Trunk with Medical Treatment and 4-Year Survival. Japan J Med Sci, 2(2), 01-05.
Abstract
A case is reported of a 64-year-old woman with anterior Myocardial Infarction with total occlusion of the left main coronary artery and she has survived 4 years with medical treatment alone.
Clinical Case
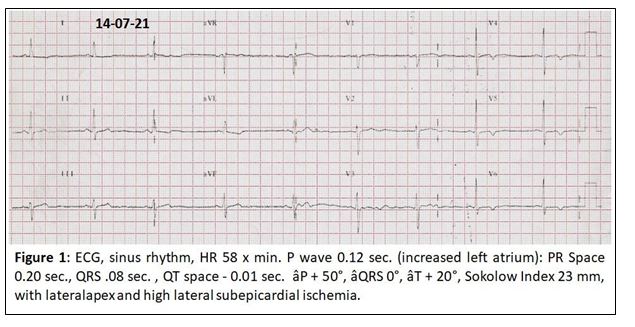
62-year-old female patient with a history of Diabetes mellitus diagnosed 3 months ago, Hyperuricemia, Kidney donor (2008); that on 07/28/20 when around 8:00 p.m. presented oppressive retrosternal pain until neck 5/10 that gradually increased until it became 10/10 over the course of 20 minutes, associated with dyspnea, diaphoresis, pallor, and arrive to “Ignacio Chávez” National Institute of Cardiology in Mexico. The electrocardiogram shows (figure 1).
Lab Exams
HGB 13, HCT 39, PLT 439, LEU 7.5, CREAT 0.98, TROPONIN I 12, GLU 106, NA 136, K 4.29, Cr 1.0't, BUN 11, PCR 31.9, RP
12.5, TTP 29.6, TM 16.2.
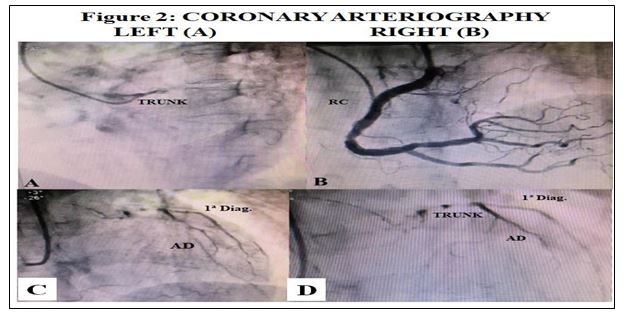
Coronary Arteriography From July 28, 2020 (Figure 2)
A) Left coronary artery: Occluded trunck (figure 2A).
B) Right coronary artery: The contrast shows a large dominant right coronary artery (figure 2B), which irrigates the right heart and the irrigation reaches the LAD that is very small and thin, the same as the 1st diagonal (figures 2C and 2D) that reaches the trunk and perfuse it slightly in a retrograde form, and in this way there is irrigation to the LV.
Interpretation
Diagnosis
I. Acute total occlusion of the left main coronary artery with apicolateral and high lateral subepicardial ischemia.
II. Dominant right coronary artery that partially revascularizes the left ventricle with filling by heterocoronary AD and 1ª Diag.
III. Type 2 diabetes mellitus.
IV. Monorenal.
V. Coronary atherosclerosis.
Treatment
1 - Low cholesterol and carbohydrate diet
2 - Aspirin Protec, 100 mg. 1 x 1
3 - Bisoprolol Fumarate 2.5 mg. 1 x 1
4 - Xarelto 2.5 mg. 1 x 1
5 - Atorvastatin 40 mg. ½ x 2
6 - Isosorvide 20 mg. 1 x 2
7 - Pantoprazole 40 mg. 1 x 2 (2023)
8 - Melox 1 x 6 (2023)
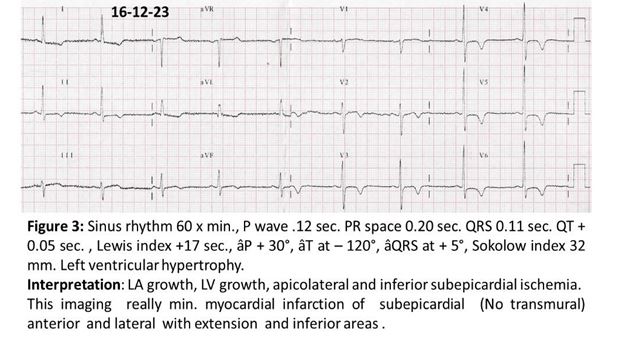
Since the start of her treatment, the patient has remained asymptomatic from a cardiovascular point of view. In 2023, she presented symptoms suggestive of ulcer syndrome, for which treatment with antacids was started; and that same year, she began to present sinus bradycardia and arterial hypotension, for which Bisoprolol fumarate was discontinued and she was prescribed Procoralan 5 mg. 1 x 2. The patient continued to be asymptomatic and a new electrocardiogram 2 years after (Figure 3) showed an image of anterolateral subepicardial ischemia with high and lower lateral extension; signs of left ventricular hypertrophy also appeared.
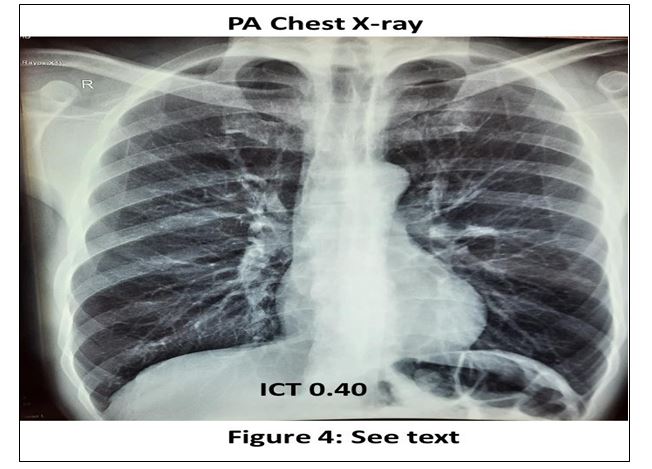
Chest PA Rx (figure 4)
The ICT is 0.40, there are signs of left ventricular hypertrophy as judged by the rounded morphology of the cardiac apex; the aorta
is opaque ++ (aortosclerosis) and the pulmonary fields are clear with normal pulmonary artery circulation morphology.
On August 27, 2024, the patient is asymptomatic and treatment is adjusted as follows
1. Procoralan 5 mg. 1 x 2 4. Apirina Protec 100 mg 1 x 1
2. Isosorbide 20 mg. 1 x 2 5. Xarelto 5 mg. 1 x 1
3. Atorvastatin Tabs. 40 mg. 1 x 1 6. Medformin 850 mg. 1 x 1
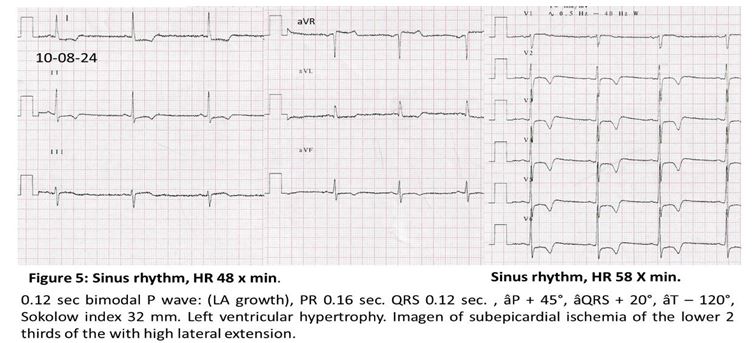
The patient remains asymptomatic, is in functional class I and the ECG shows acentuation of the anterolateral imagen of subepicardial ischemia with high lateral extension and to the inferior surface.
On August 27, the coronary arteriography scan is performed (figure 6)
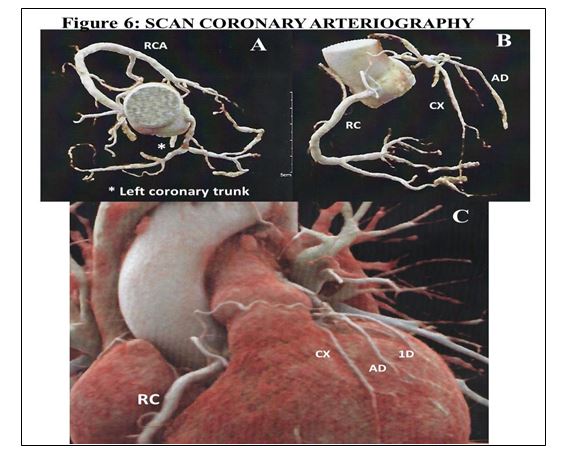
In this study, the following were found
1. Calcium index of 176 UA (CAC-DRS A2/N4, 75-90 percentile according to gender and age)
2. Epicardial coronary arteries with significant trivascular atherosclerotic disease, corresponding to CAC-RADS category 5/P2/E, for the following
a) Total occlusion of the left main trunk Score CT-RECTOR 3 and J-CTO 3 with extension to the LAD and LCx (Medina 1-1-1) where it causes significant stenosis.
b) Middle LAD with non-calcified plaque with significant stenosis. The vessel is reconstructed from the collateral of the RCA
(Vieussens arch).
c) LCx in the interline of proximal and distal segments with stenosis > 70%
d) Rest of coronary lesions with stenosis < 25%.
Comment
We present the case of a woman in her seventh decade of life, with a history of having donated a kidney and diabetes mellitus who presents an acute myocardial infarction (tropponin of 14) with a first ECG whit imagen (figure 1) showing anterior subepicardial ischemia.
This patient were presented for medical-surgical sessions, but it has been concluded that she is inoperable and on the other hand she cannot be treated with interventional techniques, since the risk of both procedures is practically fatal, because the vessels to be revascularized are small in length and in their lumen that would not allow any procedure, so the medical treatment has continued to date.
The patient's evolution has been asymptomatic, leading a normal life, and in 2023, two and a half years later, the ECG shows anterolateral subepicardial ischemia with high and lower lateral extension; the ECG also shows the appearance of left ventricular hypertrophy (Figure 3).
On the other hand, the PA chest X-ray also shows the presence of signs of LVH and aortosclerosis, but without any clinical or radiological manifestations of heart failure.
Medical treatment has been effective in reducing coagulation (anticoagulants and antiplatelets), ivabradine (procoralan) has allowed to maintain a reduced heart rate thereby decreasing MVO2 consumption, while maintaining the significant decrease in plasma cholesterol concentration is a powerful inhibitor of atherosclerosis and long-acting isosorbide to prevent coronary spasm and reduce the possibility of myocardial ischemia and finally with adequate control of plasma glycemia, are all factors that prevent progressive atherosclerosis; Thus, after 4 years, the patient remains asymptomatic and in functional class 1.
The last imaging study performed with noninvasive coronary angiotac (figure 6) shows that the occlusion of the left coronary trunk continues under the same conditions, but the dominant right coronary artery has managed to revascularize the anterior face of the heart, which maintains normal ventricular function and without clinical or electrocardiographic manifestations that show the presence of Coronary Insufficiency, that is, the patient maintains a normal life, asymptomatic and with normal ventricular function as well.
In the literature review we found that total occlusion of the trunk that does not have immediate mortality, has a prevalence of 0.04%; and 50% of these patients die upon arrival at the hospital; and those who survive do so thanks to the existence in all of them, of a dominant right coronary artery with wide collateral circulation to the left coronary artery , the ventricular function has been found preserved in 50% of the cases although cases have been reported that ideally can receive coronary revascularization, this has been due to the fact that the left ventricular circulation is sufficient to be able to receive a hemoduct or a choreographer stent, this has been possible because the circulation coming from the DA or Cx arteries are adequate to receive the hemoducts , but in this case if a revascularization had been attempted with any of the two techniques, surgical or interventional, it would have ended with death, because the DA and Cx arteries are impossible to revascularize due to their short length and caliber [1-3].
Finally, in this case, the natural evolution of the left ventricle allowed it to compensate for its function with ventricular hypertrophy, which is what has kept the patient alive; in other words, ventricular hypertrophy has been an adaptive mechanism in this case, which has allowed this patient to survive without heart failure.
Conclusion
This is probably the first case that has survived 4 years with total occlusion of the coronary main trunk, with medical treatment,
without interventional or surgical revascularization.
The good evolution of the patient can be explained because the myocardial infarction affected only the epicardium of the anterior wall of the left ventricle, because the ECG does not lose the R waves in the precordial leads as occurs in an anterolateral infarction that affects the entire wall in a transmural manner, with extension to its upper lateral region and the lower face, that is, it was a subepicardial myocardial infarction with truncal lesion in which the infarction affected only the ventricular epicardium since it was not transmural and this is what explains the good evolution of the patient due to the important revascularization coming from the right coronary artery that by irrigating the anterior descending, 1st diagonal and circumflex arteries, allowed circulation of the left ventricle [4].
References
1. Crespo, M. C., Garrido, J. C., Mas, P. T., Ribas, E. D., & Soler-Soler, J. (1997). Oclusión crónica total del tronco común de la coronaria izquierda. Revista Española de Cardiología, 50(9), 658-661.
2. Zimmern, S. H., Rogers, W. J., Bream, P. R., Chaitman, B. R., Bourassa, M. G., Davis, K. A., ... & Killip, T. A. (1982). Total occlusion of the left main coronary artery: the Coronary Artery Surgery Study (CASS) experience. The American Journal of Cardiology, 49(8), 2003-2010.
3. Moreno-Martínez, F. L., Chinea, R. G., Hidalgo, Á. L. L., Hernández, R. S. I., Miranda, I. F. A., Fleites, L. F. V., ... & Yera, R. B. (2012). Oclusión total crónica del tronco coronario izquierdo y estenosis de la coronaria derecha. CorSalud, 4(1), 67-72.
4. Guadalajara-Boo, J, F. (2019). Electrocardiografía clínica. Autoevaluación. Ed. Méndez Editores, 163-164.