
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2022) Volume 7, Issue 3
The Trend of Iatrogenic Genitourinary Fistula from 2005 to 2019 and Its Risk Factors at Addis Ababa Fistula Hospital, Addis Ababa, Ethiopia: A Retrospective Study
Received Date: May 30, 2022 / Accepted Date: Jun 09, 2022 / Published Date: Jul 25, 2022
Copyright: ©Maranata Dawit Ambaw. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Maranata Dawit Ambaw. (2022). The Trend of Iatrogenic Genitourinary Fistula from 2005 to 2019 and Its Risk Factors at Addis Ababa Fistula Hospital, Addis Ababa, Ethiopia: A Retrospective Study. Int J Women's Health Care, 7(3):110-118.
Abstract
Background: Genitourinary fistula is one of a public health importance in low- and middle-income countries. It causes multiple health adversities. Mainly, lack of timely and appropriate intervention such as cesarean section causes genitourinary fistula. Nevertheless, iatrogenic genitourinary fistula is a result of medical error during obstetric and gynecological surgery such as while cesarean section and hysterectomy. This study examined the trend of iatrogenic genitourinary fistula, major surgical procedures leading to iatrogenic fistula and its risk factors.
Methods: a facility based cross sectional study design was deployed. The respondents were included retrospectively using their medical history from January 2005 to December 2019 at Addis Ababa fistula hospital, Addis Ababa, Ethiopia. Data was analyzed using SPSS version 20.0 software. Annual percent change and average annual percent change were calculated using joinpoint regression analysis on joinpoint regression program version 4.8.0.1. Bivariate and multivariable regression model was also undertaken to implore the important risk factors for iatrogenic genitourinary fistula.
Results: Total 9229 fistula patients treated in the hospital. Of which 643(6.96%) and 8,586(93.03%) referred iatrogenic genitourinary fistula and obstetric fistula cases, respectively. The mean age of iatrogenic genitourinary fistula patients was 30.02 (± 4.63 SD) years, ranged 17- 45 years. Among the iatrogenic genitourinary fistula cases, 341(53%) were caused by cesarean section. Other causes were errors while repairing ruptured uterus 131(20.4), during undertaking hysterectomy for ruptured uterus 78(12.1%), and while gynecological hysterectomy 93(14.5%). From 2005 to 2019, there was a significant rising trend in iatrogenic genitourinary fistula (1.55% to 52.9%, p<0.001). Average annual percent change from 2005 to 2019 was 13.2% (95% CI: 7.7, 18.9).Statistically significant risk factors for iatrogenic genitourinary fistula were history of obstetric or gynecologic surgery, type of institution where the surgery conducted, and parity.
Conclusion: The trend of IGF substantially increased while the OF declined over 2005 to 2019 period. Patient safety and quality surgical procedure on pelvic surgeries is paramount important. The study also revealed that CS was the most frequent surgery resulting IGF followed by repairing ruptured uterus, hysterectomy for ruptured uterus and gynecologic hysterectomy.
Keywords
Iatrogenic Fistula, Genitourinary Fistula, Cesarean Section
Introduction
An iatrogenic genitourinary fistula (IGF) is an abnormal hole or communication between bladder or ureter and the uterus or cervix or vagina mostlyresulted from medical error while surgical inter¬ventions such ascaesarean section (CS), repair of ruptured uterus, hysterectomy for ruptured uterus, and gynecological hysterectomy [1].
A medical error pertained an intended act either of omission or commission or one that does not achieve its intended outcome, the failure of planned action to be completed as intended or the use of wrong plan to achieve an aim. Annually, more than 200 million surgeries operated in the world.To make sure surgeries are safe to patients, there are several global and national initiatives such as‘100,000 lives campaign’ in 2005/2006,and ‘5 million lives cam-paign’ in 2007/2008 by institute of health care improvement (IHI). The other initiative was the World Health Organization (WHO) safe surgery save lives’ campaign in 2009 [2]. Birth attendance by skilled care providers has substantially increased in the past decade. Globally, 73% of births attended by skilled birth attendant [3].
Many developing countries in the world didn’t meet the Millen-nium Development Goal (MDG) for maternal mortality, connoted still a high annual maternal death and countries expected to im¬prove quality of care for maternal and newborns to achieve the-sustainable development goals (SDG) [4]. Many developed and developing countries have made substantial progress toward the eradication of obstetric fistula which is usually caused by pro¬longed and obstructed labor. It seemed thatobstetric fistula from prolonged and obstructed labor decreased but IGFcontinues to be a burden in low- and middle-income countries [5]. Consequently, depression and anxiety, social isolation, depression and grief re¬lated to infertility, inability to work, and stigmatization are a huge health and social problems. The consequences of GF further com¬plicated by recurring infections, infertility, damage to their vaginal tissue and paralysis of the muscles in their lower legs [6].
Beyond this, women with GF are prone forinvisible medical con-dition such as mental health, child and fertility issues and coping mechanisms in developing countries [7]. Some of the determinants for the occurrence of IGF include prolonged labour prior to obstet-ric surgery, medical co-morbidities or case-mix, hospital type or size or location, technological resources of the health care facility and physician’s years in practice, location of training, medical spe-cialization [8].
Estimated IGF coverage directly informs the quality of health care to pregnant women. In many low-resource settings, women have heeded the call to deliver at a health facility to prevent fistula and other adverse outcomes, it is imperative that the health system in turn have to deliver quality care to them [9]. Reliable and valid evaluation of quality of intrapartum care is very important to ad¬dress high maternal and neonatal mortality rates in low- and mid¬dle-income countries but the progress so far is slow. Recent works done to develop and validate instruments for use in sub-Saharan Africa are encouraging but integrating into routine practice is low [10].
Many researches showed the prevalence and risk factors of obstet-ric fistula though recent studies are limited in Sub-Saharan Africa countries including Ethiopia. Moreover, studies specific to trend and risk factors of iatrogenic genitourinary fistula is very scarce. The study, therefore, benefit the government to modify the policy towards quality maternity services and improve health care pro¬vider training.
The study helps to focus the intervention orientation on adequate safety standards as equal as the improving quality sur¬gical care and expansion of essential surgical services in the country. The study will also have implication to implement nationwide routine monitoring of IGU making it as a reportable sentinel event.
Materials and Methods
The study was a facility based retrospective patient information review at Addis Ababa Fistula Hospital. The hospital provided mainly curative and rehabilitative services for women with genito¬urinary fistula surgical conditions.The hospital established in 1974 and has provided care and support for 55,000 fistula patients. Ma¬jority (93%) of cases were treated successfully but yet the remain¬ing (7%) got the rehabilitation services. The hospitals targeted care for4000 women per year [11].
The hospital was chosen due to it was the largest and comprehen¬sive fistula center in Ethiopia.All IGF patients who fulfill the in¬clusion criteria and registered by the Addis Ababa fistula hospital from 2005-2019 were included in the study. For data collection, Data collection checklist which is developed after review of pa-tient’s chart and similar literatures was used and data was recorded on data collection checklist through reviewing of patient medical history retrospectively. Those patients who developed fistula after a major obstetric or gynecologic surgery and presented to the hos¬pital with history of urine leakage were classified under iatrogenic genitourinary fistula. Whereas those patients who developed geni¬tourinary fistula after prolonged or obstructed labour and present¬ed to the hospital with a history of urine leakage were categorized under obstetric fistula patients.
Three BSc nurses who are currently giving nursing care for the cli¬ents under study were recruited for data collection and they were given three days training on data collection tools and techniques. The data was then collected from June 5-July 15 2020GC. Prior to data collection period, three days training was given for data collectors. After the collected data checked for completeness and consistency, data was encoded and entered to EPI-data software then to SPSS Version 20.0 software. Time trends in incidence of iatrogenic genitourinary fistula were analyzed using linear regres¬sion analysis with SPSS version 20.0 software. Annual percent change (APC) and average annual percent change (AAPC) was calculated for iatrogenic genitourinary fistula using join point re¬gression analysis on join point regression program version 4.8.0.1. Binary logistic regression model was used to analyze risk factors associated with iatrogenic genitourinary fistula. Crude odds ratio and adjusted odds ratio was calculated with 95% CI.
Result
Sociodemographic Characteristics of Patients
Between January 2005 and December 2019, 10120 genitourinary fistula (GF) patients were treated at Addis Ababa fistula hospital. Cases with complete information were 9229. Iatrogenic genitouri¬nary fistula (IGF) cases accounted 643(6.96%) and obstetric fistula (OF) cases were 8586(93.03%). The mean age of IGF patients was 31.02 ± 4.625 (SD) years (range, 17- 45 years). 128(19.9%) IGF patients had history of obstetric and gynecologic surgeries while 515(80.1%) of cases didn’t have. Notably, cesarean section (CS) was the most frequent obstetric surgery 102(79.68%) followed by ruptured uterus repair 26(20.32%). Over two-third 99(77.3%) of cases had only one occasion of obstetric surgery. (Table 1) (Fig 1).
Table 1: Respondent’s Sociodemographic characteristics, Addis Ababa fistula hospital from 2005 to 2019
|
Variable |
Frequency (%) (n=9229) |
|
Age (yrs) |
|
|
10-19 |
1878(20.9) |
|
20-29 |
3923(42.5) |
|
30-39 |
2996(32.4) |
|
40-49 |
432(4.6) |
|
Parity |
|
|
0 |
437(4.7) |
|
1 |
5656(61.3) |
|
2-5 |
2893(29) |
|
>5 |
243(4,9) |
|
Height |
|
|
1.≤1.50m |
3615(39.2) |
|
2. 1.50-1.60m |
3709(40.2) |
|
3.≥1.60m |
1905(20.6) |
|
Previous history of surgery |
|
|
Yes |
821(8.9) |
|
No |
8408(91.1) |
|
Frequency of previous surgery |
|
|
Once |
634(77.5) |
|
Twice or more |
184(22.5) |
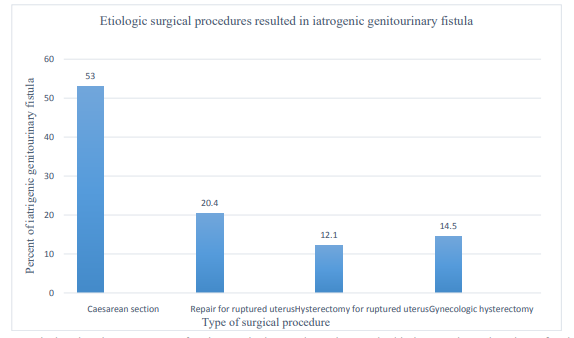
Figure 1: Bar graph showing the percentage of major surgical procedures that resulted in iatrogenic genitourinary fistula at Addis Ababa Fistula Hospital from 2005G.C to 2019G.C, Addis Ababa, Ethiopia
From a total of 643 IGF cases, more than half 346 (53.8 %) were Vesico-cervico vaginal fistula followed by ureteric injuries 179 (27.8 %).Majority 552(85.5 %) of IGF occurred as a consequence of surgery to treat obstetric complications. From the obstetric sur¬geries, cesarean section 341(53.0%), repair for ruptured uterus 131(20.4), hysterectomy for ruptured uterus 78(12.1%), and gyne¬cological hysterectomy 93(14.5%) attributed the IGF. respectively. Majority 533(82.9%) of IGF referred from governmental institu-tions.Among the IGF, 215(33.4%) of them had operation at prima¬ry hospitals and 428(66.6%) them at general hospitals. Patients mean age developed fistula was 30.41±4.57 SD) years and mean age to fistula repair was 31.02±4.625 (SD) years.The modal parity was 2. A greater proportion of multiparous women had IGF (72.3%) compared with primigravid (27.7%). The mean duration of urine leakage of IG patients was 10.142±9.98 (SD) months (ranged 0.5 to 46 months of urine leakage).
Trend of Iatrogenic Genitourinary Fistula
The IG cases dramatically increased from 1.6% to 52.9% between 2005 and 2019. But, OF substantially decreased from 98.5% to 47.1 % (Table 3) (Fig 3). From the cause of IGF, sections trend rose over the years from 2005.
Table 2: Yearly Trend of genitourinary fistula, Addis Ababa fistula hospital, Addis Ababa, Ethiopia, 2020
|
Year |
Fistula type |
|
|
Obstetric fistula |
Iatrogenic genitourinary fistula |
|
|
Frequency (%) |
Frequency (%) |
|
|
2005-2006 |
2375(98.45) |
37(1.55) |
|
2007-2008 |
2253(98.05) |
44(1.95) |
|
2009-2010 |
1717(96.69) |
57(3.31) |
|
2011-2012 |
1329(93.46) |
87(6.54) |
|
2013-2014 |
610(81.7) |
112(18.3) |
|
2015-2016 |
423(78.73) |
90(21.27) |
|
2017-2018 |
350(64.29) |
125(35.71) |
|
2019 |
172(47.1) |
91(52.9) |
The IGF showed a significantly rising trend over the years(p<0.001). Among the total GF patients, 1.97% were IGF over the year 2005 to2009, 9.16% in 2010 to2014, and 47.65% in 2015-2019. We not- ed that 12.3% of change in IGF cases were explained by a change in year (R2 = 0.123, B coefficient =4.23, 95% CI= 3.04, 5.42).
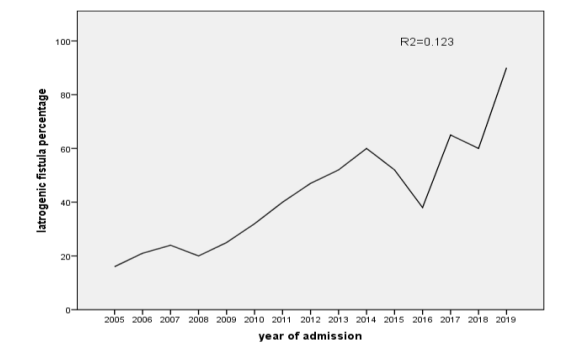
Figure 2: Overall trend of iatrogenic genitourinary fistula patients between 2005 and 2019, Addis Ababa fistula hospital, Ethiopia,2020
According to the Joinpoint regression analysis IGF annual per-cent change (APC) and over the years from 2005-2019 was very substantially increased from 2016 to 2019. The overall IGF rate increased significantly by 13.2% (95% CI 7.7, 18.9) per year from 2005-2019. A change point occurred over the years 2013-2016 where Iatrogenic genitourinary fistula cases decreased signifi-cantly with APC of -6.39% (95% CI -3.7,15.7) but it significantly increased far more rapidly over the years 2016-2019 with APC of23.28% (95% CI 12.9,34.6).
Table 3: IGF Annual percent change and average annual percent change over the years from 2005 to 2019, Addis Ababa fistula hospital, Ethiopia, 2020
|
Year |
APC (95% CI) |
AAPC (2005-2019) (95% CI) |
|
2005-2013 |
19.89(9.8,27.2) |
13.2(7.7-18.9) |
|
2013-2016 |
-6.39(-3.7,15.7) |
|
|
2016-2019 |
23.28(12.9,34.6) |
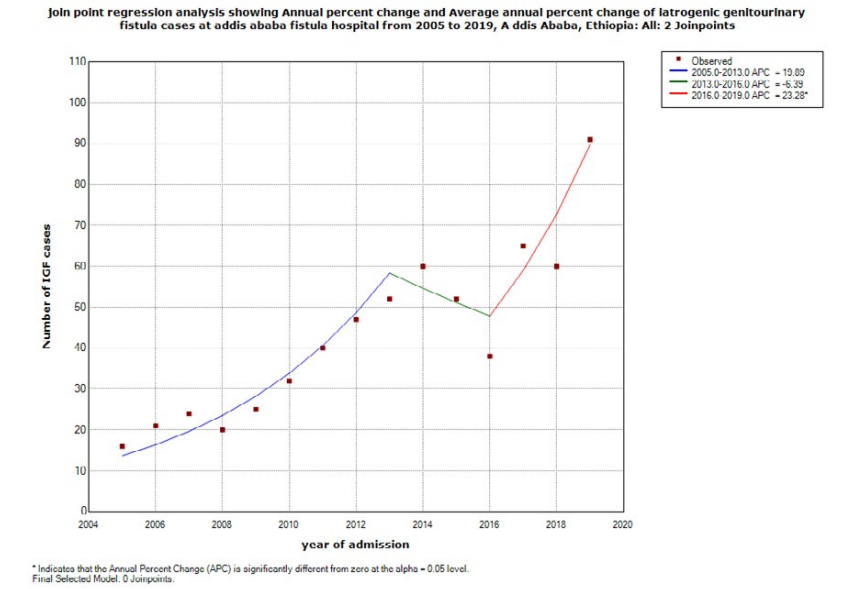
Figure 3: Joinpoint regression analysis of iatrogenic genitourinary fistula, Addis Ababa fistula hospital, Ethiopia, 2020
Risk Factors for Iatrogenic Genitourinary Fistula
Statistically significantly associated factors with IGF were history of obstetric or gynecologic surgery, hospital type where patients referred, height of patients, and parity. The odds of women with history of obstetric and gynecologic surgery were twice higher than those without surgery history (AOR=2.38; 95% CI: 1.03-3.42). The odds of those patients who were referred from governmen¬tal institutions were nearly twice more likely to develop IGF than those who were referred from private hospitals(AOR=1.71; 95% CI: 0.97, 3.34). The odds of IGF Patients with height ≥1.60 me¬ter were six times more likely to develop IGF than patients with height <1.50 meter (AOR=6.32; 95% CI: 4.71-7.89).Woman with 2 to 5 parity had 7 times higher risk to develop IGF compared to women with parity above or equal to5 (AOR=7.67; 95% CI (1.34-10.41)} {AOR=0.92; 95% CI (0.73-1.48)},respectively.
Table 4: Binary regression for factors associated with iatrogenic genitourinary fistula, Addis Ababa fistula hospital, Addis Ababa, Ethiopia 2020
|
Category |
Iatrogenic genitourinary fistula |
|||
|
No (%) |
Yes (%) |
COR1(95% CI) |
aOR2(95% CI) |
|
|
8588(93.4%) |
643(6.96%) |
|||
|
Parity |
||||
|
0 |
430(98.39%) |
7(1.61%) |
1 |
1 |
|
1 |
5482(96.97%) |
171(3.03%) |
1.91(0.89,4.1) |
1.23(0.53,3.41) |
|
2-5 |
2242 (83.56%) |
441(16.44%) |
12.08(5.68,25.67) *** |
7.67(1.34,10.41) *** |
|
≥5 |
432 (94.73) |
24(5.27%) |
3.41(1.45,8.00) *** |
0.92(0.73,1.48) |
|
Type of referral hospital |
||||
|
Private institution |
818(95.78%) |
36(4.22%) |
1 |
1 |
|
Government institution |
6145(92.01%) |
533(7.99%) |
1.97(1.39,2.78) *** |
1.71(0.97,3.34) *** |
|
Non-Governmental organizations |
1623(95.63%) |
74(4.37%) |
1.03(0.68,1.55) |
0.92(0.43,1.53) |
|
History of surgery3 |
||||
|
No |
7833(93.87) |
515(6.13) |
1 |
1 |
|
Yes |
693(84.40) |
128(15.61) |
2.80(2.28,3.46) *** |
2.38 (1.03,3.42) *** |
1COR – crude odds ratio; 2AOR - Adjusted odds ratio; 3 history of surgery included obstetric and gynecologic surgery; ***= P<0.001
Discussion
The study examined the trend of IGF from 2005 to 2019, major etiologic surgical procedures and risk factors associated with IGF in Ethiopia.
The study revealed that about 7% of GF patients were IGF while 93.4% of fistula cases classified in OF, commonly occurred fol-lowing prolonged and obstructed labor. The finding concurs with a study conducted in Democratic Republic of the Congo (8.3%) and Niger (9.9%) of iatrogenic origin (9). Contrary to this finding, higher number of IGF cases reported in 11 SSA countries where 13.2% were IGF [12]. Similarly, a study in North West Nigeria found 16.1% of 728 fistula repair surgeries were iatrogenic causes [12]. Furthermore, a study in India and Pakistan reported 39% and 58.5% of IGF, respectively [13,14]. This finding is relatively high¬er compared with this study and the study done in 11 sub-Saharan countries which found 13.2% prevalence of iatrogenic genitouri¬nary fistula [12].
This high discrepancy in prevalence of iatrogenic genitourinary fistula from country to country might be because in African coun¬tries specially in sub-Saharan countries obstetric fistula which is commonly caused after prolonged and obstructed labor takes many proportions of the overall genitourinary fistula cases. But in developed countries obstetric fistula takes smaller proportion of the overall fistula cases than iatrogenic genitourinary patients. Another reason for this discrepancy might be because of the study area at which this study done is only limited to one hospital which is giving most of the treatment for fistula patients in the country but doesn’t include regional hospitals.
This study found that the most frequent surgical procedures caus¬ing IGF was CS (53%). Also, findings from 11 SSA countries informed a similar result, CS (57.4%) [12]. However, a study in North West Nigeria reported a higher one (73.6%) of IGF cases attributed by emergency CS [15]. Differently, the Pakistan study showed the major cause of IGF was hysterectomy (52.5%), hys¬terectomy for ruptured uterus (26.4%), and CS (19.9%). The rea¬son for this discrepancy might be because cesarean section is the frequently performed obstetric surgery in Ethiopian than repair for ruptured uterus and hysterectomy for ruptured uterus.
Following cesarean section this study also found the most frequent surgical procedures resulted in iatrogenic genitourinary fistula were Repair for ruptured uterus, hysterectomy for ruptured uter¬us and gynecologic hysterectomy constituting 20.4%,12.1% and 14.5% respectively whereas the findingof 18 years retrospective study of iatrogenic genitourinary fistula cases at 11 sub Saharan African countries revealedhysterectomy (19.8 %)is the major sur¬gical procedure that resulted in iatrogenicgenitourinary fistula fol¬lowing cesarean section followed by gynecological hysterectomy (19.6 %), ruptured uterus repair (3.1 %) [12].Therefore the find¬ings from this study shows there is a need for advanced training for improved decision-making and surgical skills in both obstetric and gynecologic surgeries, especially for safe cesarean delivery and hysterectomy. Unnecessary cesarean section delivery includ¬ing elective cesarean delivery rate have to be lowered to decrease the incidence of iatrogenic genitourinary fistula.
Regarding the type of iatrogenic genitourinary fistula this study found almost similar findings with other researches done in differ-ent countries. Of the 643 IFs, 346 (53.8 %) were VCVF, 179 (27.8 %) were ureteric injuries, and 118 (18.4 %) were Vault fistulas. This finding is almost similar with the report of retrospective study done in 11 sub Saharan countries found that 33.9 % were ureteric injuries, 22.5 % were vault fistulas, and 43.6 % were VCVF [12]. The findings from two-year retrospective insight of all cases that underwent repair for iatrogenic genitourinary fistula at the Nation¬al Obstetric Fistula Centre, BabbarRuga, Katsina, Katsina State, North West Nigeria from 1 Jan 2015 to 31 December 2016 report¬ed 62.7% of IF cases were VCVF [15]. These types of IF mainly result after obstetric surgeries like cesarean section and repair for ruptured uterus. The high proportions of this types of fistula indi¬cates the need to supervision and monitoring of obstetric surgeries by quality improvement teams in every hospital performing these surgical procedures.
The other objective of this study was to assess the trends of iat-rogenic fistula cases over 15 year’s period.The causes of genito-urinary fistula in low- and middle-income countries is prolonged and obstructed labour which eventually lead to obstetric fistula but not linked to iatrogenic origin which is result after medical error during surgeries. However, cases of iatrogenic genitourinary fistu¬la appear to be increasing in recent years. This study revealed the rising trend of iatrogenic fistula over the study period with only 1.55% of the total genitourinary fistula patients at the beginning of the study period 2005–2006 were iatrogenic in origin, 18.3% in 2013-14 and 52.9% in 2019. The continuous rise in iatrogenic genitourinary fistula cases were found to be significant (p<0.001). A decreasing trend in obstetric fistula, from 98.45% to 47.1%, was also observed. On Linear regression analysis R2 was found to be 0.123 which can be interpreted as 12.3% of change in iatrogenic genitourinary fistula cases can be explained by a change in year of admission. B coefficient is 4.23(95% CI 3.04, 5.42) which can be interpreted as for every unit increase in year of admission iatrogen¬ic genitourinary fistula cases increased by 4.23. Join point regres¬sion analysis was also done to calculate the annual percent change and the average annual percent change of iatrogenic genitourinary fistula. The average annual percent change over the years from 2005 to 2019 was found to be 13.2 % (95% CI 7.7, 18.9).
A change point occurred over the years 2013-2016 where Iatrogen¬ic genitourinary fistula cases decreased significantly with APC of -6.39% (95% CI -3.7,15.7) but it significantly increased far more rapidly over the years 2016-2019 with APC of23.28% (95% CI 12.9,34.6).Another study which is a 14 years retrospective study done at Pakistan, institute of medical sciences found rising trend in iatrogenic fistula over the study period (2006–2018) from 43.5% to 71.4% and a decreasing trend in ischemic fistula, from 56.5% to 28.6%, was also observed [14].
The recent decrease in obstetric fistula cases can be explained by an increasing access to skilled birth attendants on the last decade.
But alarmingly increasing cases of iatrogenic genitourinary fistula cases over the last decade and half indicated the need to work on improving not only access to skilled birth attendant but on quality of health service especially surgical quality and safety have to be given emphasis.
Regarding the factors associated with iatrogenic genitourinary fistula this study found that previous history of obstetric or gy-necologic surgery was one of the factors significantly associat-ed with iatrogenic genitourinary fistula. Those with no previous history of obstetric or gynecologic surgery were found to be 0.42 {AOR=0.42; 95% CI (0.34-0.51)}times less likely to develop iat¬rogenic genitourinary fistula than those with previous history of obstetric or gynecologic history. This finding is consistent with similar researches done in different countries. A research done at Kilimanjaro medical center, Tanzania on women who were treat¬ed for iatrogenic ureter and bladder injuries after obstetric and gynecologic surgical procedures showed prior uterine operation, endometriosis, cervical myoma and prior pelvic radiation are the factors associated with iatrogenic genitourinary fistula [16]. The retrospective study done in 11 sub-Saharan African countries also mentioned Scar tissue and adhesions from prior laparotomies can create challenges for providers performing obstetric and gyneco-logical surgery that might result in occurrence of iatrogenic geni¬tourinary fistula [12].
The other factor that was found to be significantly associated with iatrogenic genitourinary fistula is the type of health institution in which the surgical procedure takes place. This study found that those patients who had obstetric or gynecologic surgical proce¬dures at governmental institutions were 2 times {AOR=1.71; 95% CI (0.97-3.34)} more likely to develop Iatrogenic genitourinary fistula. This might be because of poor surgical quality of care, lack of technological resources and lack of continuous in job training for the physicians who are performing the surgical procedures in these hospitals. There are limited researches done that shows the association between the type of health institution and iatrogenic genitourinary fistula. But this finding can be associated with the rate of delivery by cesarean section in this hospital. A study done by LSHTM on The Landscape of Cesarean Section of 44 countries in Sub-Saharan Africa and South and Southeast Asia to compare percentages of cesareans with a non-doctor SBA by facility own¬ership in 28 of the 44 countries. In Sub-Saharan Africa, 18 of the 20 countries with data had a higher percentage of non-doctor SBA cesareans in public facilities than in nonpublic facilities; the wid¬est difference was in Namibia, with 39% in public facilities but only 3% in nonpublic facilities. In South and Southeast Asia, four countries had higher percentages in public facilities (with India having the widest difference between public and nonpublic facili¬ties, at 7% vs. 3%), and four had higher proportions in nonpublic facilities (with the widest difference in Indonesia, at 10% public vs. 23% nonpublic) [17].
This study also found parity of women was significantly associat¬ed with iatrogenic fistula patients. Those woman with parity of2 up to 5 were 7 times more likely to develop iatrogenic genitouri¬nary fistula compared to those with parity ≥5{AOR=7.67; 95% CI (1.34-10.41)} {AOR=0.92; 95% CI (0.73-1.48)}, respectively. Although there is no previous evidence that link parity of the pa-tients with iatrogenic genitourinary fistula this association can be explained by the formation of scar and adhesion from previous repeated deliveries especially if previous deliveries were made by cesarean section.
Strength and Limitation of the Study
There are very limited researches done related to trends of iatro-genic genitourinary fistula and its associated risk factors, so the finding of this research will be very useful resource for further research regarding the topic. Since all information was taken from patient’s chart, there is incompleteness of data to have full infor¬mation and there are limited researches done regarding factors associated with iatrogenic genitourinary fistula to discuss the find¬ings with other studies.
Abbreviations
OF: obstetric fistula
IGF: Iatrogenic genitourinary fistula
IHI: institute of health care improvement
CS: Cesarean section
GF: Genitourinary Fistula
APC: Annual percent change
AAPC: Average annual percent change
Conclusion and Recommendation
The trend of IGF substantially increased while the OF declined over 2005 to 2019 period. Patient safety and quality surgical pro-cedure on pelvic surgeries is paramount important. The study also revealed that CS was the most frequent surgery resulting IGF followed by repairing ruptured uterus, hysterectomy for ruptured uterus and gynecologic hysterectomy. History of obstetrics and gynecologic surgery, referral hospital type, and parity were signifi-cantly associated risk factors for IGF. Overall, the study provides information the required adequate maternity service centers and providers for the current and future need of quality surgical care. Understanding the burden of IGF and OF burden of morbidity in Ethiopia can have positive implications for policy development and advocacy efforts.
I recommend from the findings of this research to Strengthen pro¬vider and system capacity to provide and sustain quality services, improve health institution’s surgical quality and safety through supervision and monitoring of surgical procedures by quality im¬provement teams, Modify the policy of health professionals train¬ing in the country to focus more on the quality rather than quanti¬ty of graduating health professionals. Moreover, it is essential to Advocate for regular investigation and standardized classification of iatrogenic genitourinary fistula and Increase awareness about iatrogenic genitourinary fistula trends among obstetric, midwifery, and safe motherhood communities of practice at the national level.
Acknowledgement
I am very grateful of administrative and medical staffs of Addis Ababa fistula hospital, without their support it would have been difficult to conduct this research.
Authors Contribution
Conception and design of the study, supervised data collection and management, data analysis, interpretation of the finding and final approval of the manuscript.
Availability of Data and Materials
Datasets generated during and/or analyzed during the current study are available in corresponding author.
Ethics Approval and Consent to Participate
Ethical approval on study design, participants and data collection method was obtained from the ethical clearance board of Addis Ababa University with reference number IRB/098/12, according to the standardized principles and procedures in line with national and WHO guideline. Moreover, all essential ethical considerations to insure the confidentiality of the identity of patients (fistula pa¬tients) was taken. Official letter informing the medical director of the hospital about the objective of the study was written from the university prior to actual data collection period and permission was obtained. During patient chart review confidentiality was kept no patient names were stored and any patient information were not transferred to any other organ. There was not being any harm on patients associated with this research and the patients was not being paid in cash for their information.
References
- Fistula O PTM. (2010). Obstetric Fistula – Definition, Causes and Contributing Factors, and Impact on Affected Women. What is an obstetric fistula.
- Grober, E. D., &Bohnen, J. M. (2005). Defining medical error. canadian Journal of Surgery, 48(1), 39.
- WHO. Skilled attendants at birth. Global Health Observatory Data. 2016.
- (UN) UN. The Millennium Development Goals Report 2015.
- Organization WH. 10 facts on obstetric fistula. 2014.
- WHO. Obstetric Fistula Guiding principles for clinical man-agementandprogramme development. integrated management of pregnancy and child birth. 2016.
- Bashah, D. T., Worku, A. G., & Mengistu, M. Y. (2018). Consequences of obstetric fistula in sub-Sahara African countries, from patients’ perspective: a systematic review of qualitative studies. BMC women’s health, 18(1), 1-12.
- Andargie, A. A., &Debu, A. (2017). Determinants of obstetric fistula in Ethiopia. African health sciences, 17(3), 671-680.
- Plus, F. C. (2016). Iatrogenic Fistula: An Urgent Quality of Care Challenge. New York, NY, USA: Fistula Care Plus/En-genderHealth.
- Faye, A., Dumont, A., Ndiaye, P., & Fournier, P. (2014). Development of an instrument to evaluate intrapartum care quality in Senegal: evaluation quality care. International journal for quality in health care, 26(2), 184-189.
- Attard M. “Dr Catherine Hamlin, Founder of the Addis Ababa Fistula Hospital” Sunday Profile ABC, Australia. 2011.
- Raassen, T. J., Ngongo, C. J., &Mahendeka, M. M. (2014). Iatrogenic genitourinary fistula: an 18-year retrospective review of 805 injuries. International Urogynecology Journal, 25(12), 1699-1706.
- Priyadarshi, V., Singh, J. P., Bera, M. K., Kundu, A. K., & Pal,D. K. (2016). Genitourinary fistula: an Indian perspective. The Journal of Obstetrics and Gynecology of India, 66(3), 180-184.
- Tasnim, N., Bangash, K., Amin, O., Luqman, S., &Hina, H. (2020). Rising trends in iatrogenic urogenital fistula: A new challenge. International Journal of Gynecology & Obstetrics, 148, 33-36.
- Nasir, S., Elladan, A. M., Hassan, M., &Panti, A. A. (2018). Pattern and Outcome of Iatrogenic Genitourinary Fistula from Obstetric and Gynaecological Surgeries in a Tertiary Institution, North-Western Nigeria. AJMAH, 10(3), 1-7.
- Mteta, K. A., Mbwambo, J., &Mvungi, M. (2006). Iatrogenic ureteric and bladder injuries in obstetric and gynaecologic surgeries. East African Medical Journal, 83(2), 79-85.
- Benova, L., Cavallaro, F. L., & Campbell, O. (2017). The Landscape of Cesarean Section in Sub-Saharan Africa and South and Southeast Asia.