
Journal of Veterinary Health Science(JVHS)
ISSN: 2831-3887 | DOI: 10.33140/JVHS
Impact Factor: 0.762

Research Article - (2022) Volume 3, Issue 3
The Situation of Equity in Maternal Health in Bangladesh
Received Date: Aug 13, 2022 / Accepted Date: Aug 19, 2022 / Published Date: Sep 26, 2022
Copyright: ©Copyright: ©2022 Mohammed Moshiur Rahaman. This is an openaccess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Rahaman MM, Haque M, Uddin MM, Shihab E, Khan SH. (2022). The Situation of Equity in Maternal Health in Bangladesh. J Vet Heal Sci, 3(3),295-299.
Abstract
Background: To assess the equity in maternal health services in Bangladesh.
Methods: The report was prepared primarily relying on secondary available data, in particular the BDHS report from 2007 to 2014. Based on key identified indicators, a survey was conducted with a short set of a questionnaire among sample size 200.
Results: 50% of women did get antenatal care from any trained/untrained health worker, 35% of pregnant women did not get assistance from any qualified health worker and another 15% get assistance from untrained birth attendance, 80% of mother did not have enough education to know or concern about what should they during delivery or after delivery or what kind of complications can be risen, 25% of mother received antenatal care from the private sector after delivery, 70% of mother did not receive any post-natal check-up after delivery.
Conclusion: Inequity in maternal health in Bangladesh is visible which is aligned with national delivery care, antenatal care, and postnatal care. Inequity problems mostly in poor families. Antenatal care from the private sector after delivery indicates that higher treatment costs in the private sector pushed them under the poverty line.
Keywords
Equity, Maternal Health, Bangladesh, Delivery Care, Antenatal Care, Postnatal Care
Introduction
Bangladesh is that the world’s eighth most densely inhabited country wherever most (75%) of the population resides in rural areas, though the country is changing into more and more urban-ized. The population consists of roughly ninety-eight percentage ethnic Bengalis, with totally different social group teams creat-ing up to two percent of the population. The bulk majority of the population are Muslim (89.5%) with the rest comprised of 9.6% of Hindus, 0.5% of Buddhists, 0.3% Christians, and different spiritual teams [1].
Due to the economic, social, health conditions and strong patri-archal structure of society, Women are relatively disadvantaged. As a result, these factors create movement restriction, a culture of acceptance, early wedding, and low vanity, lack of effective community support structure, and inappropriate allocation and utilization of resources [2].
In Bangladesh, Family planning was introduced in the early 1950s and adopted as a government sector program in 1965. The necessity of population control and maternal health care was em- phasized in the first Five-Year Plan (1973-1978), and integrated with health service since 1980 and aimed to provide a package of essential and quality health care services by the sector-wide approach (SWAp) in 1998.
HPNSDP (Health, Population, and Nutrition Sector Develop-ment Program) was initiated by MoHFW (Ministry of Health and Family Welfare from July 2011 to June 2016 (5 years) to prosper and preserve the highest accessible level of health as a basic right and difficulty of social justice [3]. Women’s health during pregnancy, childbirth, and the post-partum period are maternal health, and ANC (antenatal care), delivery care, PNC (postnatal care) services, and child care are maternal health care services (Maternal and new-born health-WHO/Europe).
The lack of avoidable varations among group of people, who are or not outlined socially, economically, demographically, or geographically is equity.
Health inequities are quite difference from others in terms of health determinants, right to use the resources required to in-crease and preserve health or health outcomes (WHO- Equity).
Objectives
General objective:
To assess the equity in maternal health services in Bangladesh.
Specific Objective:
• To explore the maternal health care situation and its equity of access by the targeted population in Bangladesh.
• To analyse the trend of the maternal health care equity in Ban¬gladesh
• To compare the secondary findings with a small scale pilot sur-vey conducted in Kurigram district of Bangladesh.
Methodology
Design: The report was prepared primarily relying on secondary available data, in particular BDHS (Bangladesh Demographic and Health Survey) report from 2007 to 2014. Based on key identified indicators, a survey was conducted with a short set of a questionnaire (Annex 01) among limited sample size 200.
Survey site: Kurigram Sadar Upazila (Rural) and Ulipur Upazi¬la of Kurigram district, Bangladesh.
Survey duration: November 01, 2019, to November 14, 2019.
Survey population: Mother, who has delivered a baby in the last 6 months. Sampling technique: A randomized convenient sampling tech-nique was used for the survey.
Sample size: The survey does not follow the systemic calcula-tion of sampling rather interviewed 200 participants. Survey tool: Data was collected using a structured question-naire in English with appropriate response options.
Data collection, data entry, and data analysis: Face to face interview was conducted using a structured questionnaire. Data were entered in Microsoft Excel to analyse and produce tables and graphs.
Results and Findings
Maternal Health and Millennium Development Goals (MDGs)
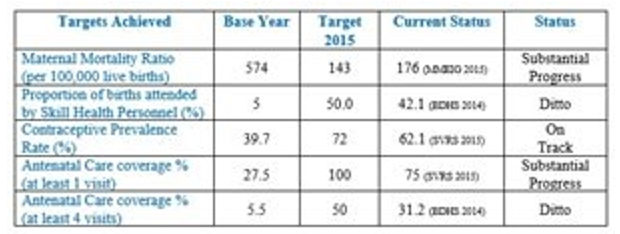
Maternal health as a worldwide public health priority is point up in the millennium development goal Five (MDG 5). Maternal mortality was reduced by ¾ between 1990 and 2015 and 2 in-dicators was set in the MDG 5 for achieving universal access to generative health by 2015 [4].
Table 1: Improved maternal health in MDGs
Equity in Antenatal Care
During the analysis of the BDHS 2014 report, Antenatal Care (ANC) coverage is substantially increased from 58% in 2004 to 78% in 2014 (Figure 01).
But the unmet need is higher among rural people, is 25.3% in contrast in urban it is 10.5%. It is also alarming that people's access to ANC care drastically decreases from 1st baby to the next babies for instance access to a qualified doctor during 1st baby is 64.9% but its decrease for next babies as 56.7%. 45.6% respectively for 2-3 birth order and 4-5 birth order, alarmingly the rate is only 27.4% for 6+ babies.
The level of education significantly contributed to influence in accessing ANC among mothers; the unmet need among second¬ary or higher education completed mother is 5.3% whereas it is 42.9% among mothers who have no education. This figure is almost similar when it depends on wealth quantile; only 4.5% of the mother from the highest wealth quantile didn’t receive ANC care while the unmet need among the lowest wealth quan¬tile group is 42.5%.
The ANC coverage is lowest in the Sylhet region compared to height in the Khulna region respectively 46.6% and 67.1% in terms of accessing qualified doctor for ANC care.
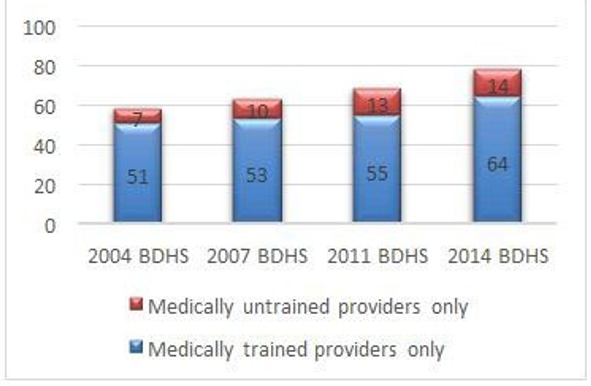
Figure 1: Use of antenatal care, 2004-2014
Equity in Antenatal Care (from the survey)
Our survey report showed that 50% of women did get antena-tal care from any trained/untrained health worker which aligned with national antenatal care (Figure 02).
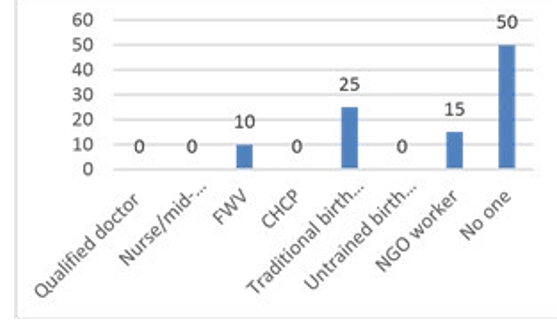
Figure 2: Use of antenatal care (from the survey)
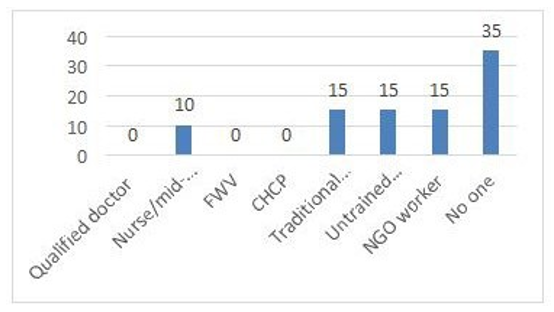
The report showed that 35% of pregnant women did not get as-sistance from any qualified health worker and another 15% get assistance from untrained birth attendance (Figure 03).
Among the surveyed mother, 80% of mothers did not have enough education to know or concern about what should they during delivery or after delivery or what kind of complications can be risen (Figure 04).
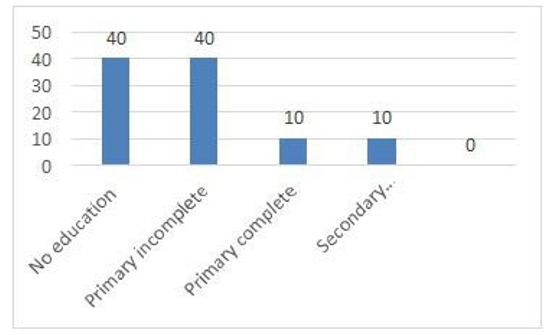
Figure 4: Education level (from the survey)
Delivery Care
The place of delivery is most important for maternal care. Though the overall progress shows a significant improvement in facilities-based care from 12% in 2004 to 37% in 2014 a notable
inequality is observed. Alarmingly, 69.1% delivery still happening at home in rural, and among the poorest people, this is 84.8%. Similar to ANC care the unmet need or poor coverage among people with „no educa-tionâ?? and in the Sylhet region which is respectively 83.8% and 76.6% (Table 02).
Table 2: Inequity in delivery care in Bangladesh

If we compare between 2011 and 2014, shows positive trends to access facility-based delivery but the inequality between wealth quantile remain similar (Figure 05)
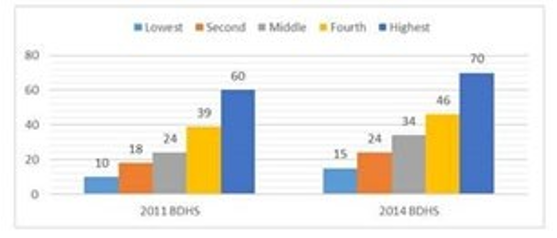
Figure 5: Facility delivery by wealth quintile, 2011 and 2014
From the survey report, it is clear that women who did not take/ receive any antenatal care all from extremely poor or poor health quintile segment. We can say that the inequity problem mostly in poor families.
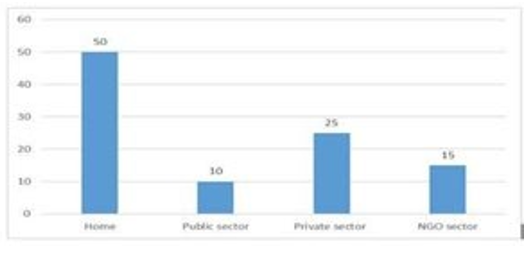
Figure 6: Antenatal care place (from the survey)
The survey report indicated that 25% of mothers received an-tenatal care from the private sector after delivery that means at that time the public sector may provide care or they are spending more money on their treatment. This kind of costly treatment options pushed them under the poverty line (Figure 06).
Postnatal Check-up for Mother
According to the 2014 BDHS report, medically trained health works provider postnatal care to 37% of mothers within 42 days in which 36% within the crucial first two days. On the other hand, 63% of mothers deprived of postnatal check-up (Figure 07).
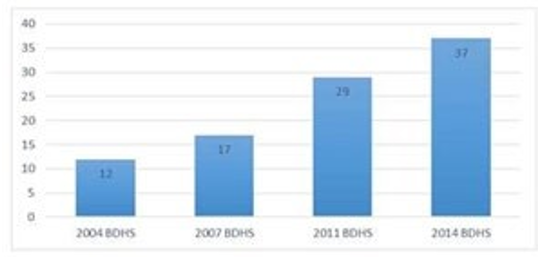
Figure 7: Trends of PNC (Postnatal Care)
But if we have a deeper look at the situation, still 67.8% of mothers living in rural areas do not have access to postnatal care (BDHS 2014) (Table 03).
Table 3: Postnatal care situation in the rural and urban area
img src="https://www.opastpublishers.com/scholarly-images/4194-69cd06e9b2ec9-the-situation-of-equity-in-maternal-health-in-bangladesh.png" width="400" height="100">
If we consider the education domain, the inequality is signifi-cantly visible to access postnatal care worryingly 82.5% mother with „no-educationâ?? does not go for postnatal care compared to 27.9% among higher educated mothers (Table 04).
Table 4: Situation of post-natal care
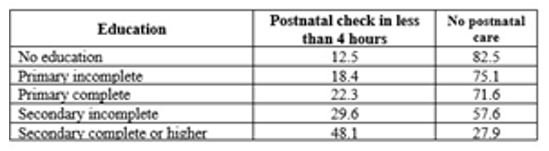
The above situation is similar in the case of accessing postnatal care among the poorest and rich people respectively 83% and 25.7% of the mother have an unmet need for postnatal care. Again the situation is worst in the Sylhet area which is 75.1% mother has no access and the lowest unmet need is in Khulna but still 45.6%. The postnatal check-up does not much depend on the age of the mother but it was observed that mother with age group 35-49 years have less access to postnatal check-up which is 69.1% while it is 59.8% among mother 20-34 age group.3
Postnatal Check-up for Mother (From the Survey)
From our survey report, it is clear that 70% of the mother did not receive any post-natal check-up after delivery. It is almost aligned with the national post-natal check-up report of BDHS 2014 which is indicated that a lot of numbers of mothers in the risk of post-natal complications. It is another inequity in mater¬nal healthcare (Figure 08).
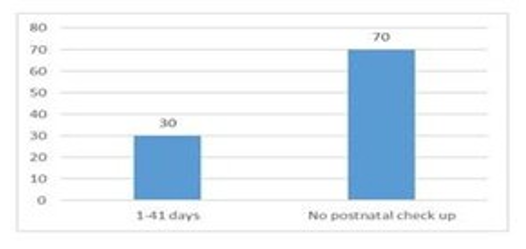
Figure 8: Postnatal check-up for mother (from the survey)
Recommendations
a. Raise awareness among the general population on the impor¬tance of maternal healthcare especially among women and girls - specifically targeting those living in the rural area and have no/ limited access to education.
b. Introduce a cash voucher system for low-income populations so that they can access necessary maternal healthcare services.
c. Enhance stewardship in maternal healthcare service by engag¬ing private hospitals, NGOs, and profit organizations to support poor people, which could be compensated by tax exemption.
d. Ensure quality of birth attendance, health workers, and mid-wives so that they can even ensure home-based ANC and PNC.
e. Provide incentives for facility-based delivery, ensure neces-sary elements to ensure facility delivery; it may be transporta-tion, the flexile opening time of service facilities.
f. Maternal healthcare could be introduced in school curricula.
g. Ensure adequate budget in the national health system to achieve universal coverage of maternal health care including the expansion of facilities and health workforce in rural areas.
Discussion
Maternal health is the most important points in the Millennium Development Goals and Sustainable Development Goals. After achieving some goals/targets in MDGs within 2015, Bangladesh received its award for its achievement from different renowned organizations.
Now from 2015 Bangladesh adopted the Sustainable Devel-opment Goals which need to achieve within 2030. We indeed achieved some goals/targets from MDGs, but in Goals 5 of Im-prove maternal health, we are just showed Substantial progress/ Ditto/On track in 5 indicators of Improve maternal health. If we comparing the MDGs achievement report to the SDGs progress report of the General Economics Division of Bangladesh Plan¬ning Commission, after adaptation of SDGs, we are just able to reduce the maternal mortality ratio to 172 after 2017 which is far away from MDGs 2015 target. But according to SDGs, it should be less than 70 within 2030. If we have more than 10 years to achieve these goals, but according to this rate we could not meet this goal within the time limit. It is alarming for us due to ineq-uities in maternal healthcare.
Through this report, we are trying to find out where the inequi-ties are in maternal healthcare and how to solve these inequities to achieve this goal in SDGs within time. We also believe that if we can solve these inequities in maternal healthcare, it will help to reduce the ratio of maternal mortality and prevent deaths of the new-born to ensure access to sexual and reproductive health care services.
Conclusions
Maternal health is not only “women’s issue”, but also concern-ing matter of societies, and nations, lads, women, boys, and la-dies whose life depend on healthy ladies and mothers.
Maternal health is not only required for social development and economic productivity, but also reduces prices and burdens to communities, families, service suppliers. Overall health system will be strengthen and the cost-effectiveness of resources allot¬ted to the health sector will be increased by investing in maternal health [6-8].
Reducing health inequities is vital as a result of health may be a basic precise and its enlightened realization can eradicate in-equalities that result from variations in health standing.5 Rising maternal health contributes a lot of broadly speaking to poverty reduction. Thus, guiding sources to maternal health is an effi¬cient manner of achieving many country planning and enlarge¬ment goals [5].
Limitations
The report is a reply to secondary data, mainly Bangladesh De-mographic and Health 2014, 2011, and 2007. The recent version of the Bangladesh Demographic and Health survey report 2017 is not available from any source.
Due to the time constraint and the limitation in the number of people who conduct field sampling, this pilot survey is limiting field sampling (200 samples) from one district only. Thus, the findings and recommendations canâ??t be generalized.
Abbreviations
HPNSDP: Health, Population and Nutrition Sector Development Program, BDHS: Bangladesh Demographic and Health Survey, MMR: Maternal Mortality Ratio, FWV: Family Welfare Visitor, CHCP: Community Health Care Provider
References
- World health organization bangladesh. (2015). Ministry of health and family welfare. Success factors for womenâ??s and childrenâ??s health:bangladesh. World health Organization.
- Rahman, S. A., Parkhurst, J. O., & Normand, C. (2003). Maternal Health Review, Bangladesh. Policy Research Unit (PRU), Ministry of Health and Family Welfare, Government of Peoples Republic of Bangladesh, Health Systems Development Programme.
- National Institute of Population Research and Training - NIPORT/Bangladesh, Mitra and Associates, and ICF International. 2016. Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh: NIPORT, Mitra and Associates, and ICF International.
- Roy, A., & Shengelia, L. (2016). An analysis on maternal healthcare situation in Bangladesh: a review. Divers Equal Health Care, 13, 360-4.
- Maternal Health. (2010). Investing in the lifeline of healthy societies and economies, Africa Progress Panel Policy Brief September.
- Maternal and newborn health-WHO/Europe.
- Millennium Development Goals BANGLADESH Progress Report 2015.
- WHO. (2016). Equal. Heal. Care 13, 360–364 (2016).