
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Case Report - (2020) Volume 5, Issue 2
The Role for Intra-Partum Antibiotics in Previously GBS-Colonised Pregnancies, Not So Straightforward After All: A Case Study
2MBChB, MSc, Department of Urogynaecology, KK Women’s and Children’s Hospital, Singapore
3MBBS, FRCOG, MMed (O&G), FAMS, Department of Obstetrics and Gynaecology, Singapore General Hospital, Singapore
Received Date: Mar 23, 2020 / Accepted Date: Apr 09, 2020 / Published Date: Apr 17, 2020
Copyright: ©Jill Cheng Sim Lee, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Group B Streptococcus (GBS) is the most frequent pathogen involved in early-onset infection in newborn infants. The incidence of early-onset GBS disease (EOGBS) is estimated at 0.4 and 0.57 per 1000 births in the United States of America and the United Kingdom respectively. It is clear that administration of intrapartum antibiotics (IAP) significantly reduces risk of EOGBS (RR 0.17, 95% CI 0.04 to 0.74; number needed to treat to benefit 25, 95% CI 14 to 100), hence institutes such as the Royal College of Obstetrics and Gynecology (RCOG), and American College of Obstetrics and Gynecology (ACOG), have released clinical practice guidelines (CPGs) with the aim to improve the standard of care in GBS screening and IAP for the prevention of EOGBS in neonates. CPGs guide clinicians in their management based on a consensus of care drawn from clinical evidence and offer a standard of care for them to fall back on to guard against medical malpractice litigation. However, deviation from the intended clinical context or the failure to recognize the limits of such guidelines could compromise patient safety.
Aim: The aim of this case study is to highlight the role and limitations of clinical practice guidelines in medical practice, through a case of an early onset GBS infection in a neonate that was a result of selectively applying the RCOG and ACOG guidelines outside their intended context.
Conclusion: The case illustrates the importance of applying guidelines correctly within the appropriate clinical context but serves also as a reminder for clinicians to understand the limitations of them when accounting for other co-conditions patients often present with in daily medical practice.
Introduction
Group B Streptococcus (GBS) is the most frequent pathogen involved in early-onset infection in new-born infants [1]. The incidence of early-onset GBS disease (EOGBS) is estimated at 0.4 and 0.57 per 1000 births in the United States of America and the United Kingdom respectively [2]. It is clear that administration of intrapartum antibiotics (IAP) significantly reduces risk of EOGBS (RR 0.17, 95% CI 0.04 to 0.74; number needed to treat to benefit 25, 95% CI 14 to 100), hence institutes such as the Royal College of Obstetrics and Gynaecology (RCOG), and American College of Obstetrics and Gynaecology (ACOG), have released clinical practice guidelines (CPGs) with the aim to improve the standard of care in GBS screening and IAP for the prevention of EOGBS in neonates [3]. CPGs guide clinicians in their management based on a consensus of care drawn from clinical evidence and offer a standard of care for them to fall back on to guard against medical malpractice litigation [4]. However, deviation from the intended clinical context or the failure to recognize the limits of such guidelines could compromise patient safety. The aim of this case study is to highlight the role and limitations of clinical practice guidelines in medical practice, through a case of an early onset GBS infection in a neonate that was a result of selectively applying the RCOG and ACOG guidelines outside their intended context.
Case
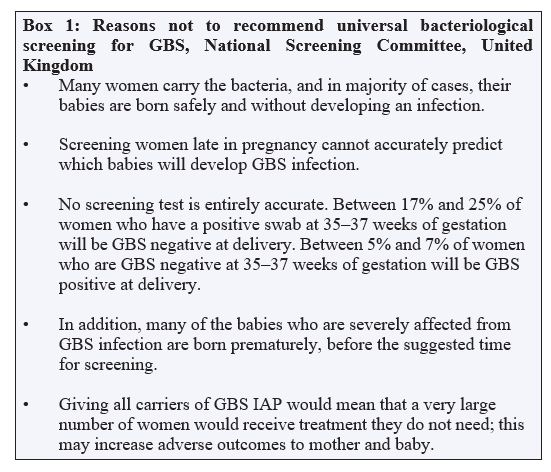
Mrs X is a 30-year old G3P1 (1 termination of pregnancy and 1 term normal vaginal delivery), with a history of GBS carriage during her previous pregnancy. She received IAP for that pregnancy, and her baby was not affected by EOGBS. When she booked in the first trimester of her third pregnancy, she was counselled to repeat screening for GBS at 35-37 weeks. At 34 weeks, fetal growth restriction (FGR) was detected on ultrasound, with estimated fetal weight centiles declining from 33.3% at 28 weeks to 9.7%. She declined inpatient monitoring and missed her scheduled visit at 36 weeks. At the subsequent follow-up visit at 37 weeks and 2 days, ultrasound studies continued to show FGR, with the estimated fetal weight declining to the 5th centile. She was advised delivery and consented to induction of labour. She was not given IAP in accordance with the ACOG guidelines and had a normal vaginal birth after a quick labour. Two days later, the baby presented with multiple episodes of regurgitation associated with fever and was diagnosed with EOGBS meningitis based on positive blood and lumbar puncture cultures. Reviewing the Guidelines The core difference between the RCOG and ACOG guidelines for prevention of EOGBS are their opposing stances on antepartum screening for GBS. The ACOG in conjunction with the CDC guidelines in 2010 recommends universal screening with a lower vaginal and rectal swab culture, while the RCOG opposes this. Box 1 cites the reasons the RCOG, in conjunction with the National Screening Committee is opposed to universal screening [5].
GBS = Group B Streptococcus, IAP = intrapartum antibiotic prophylaxis
With regard to women who have previously been colonised by GBS, the ACOG and RCOG guidelines have important differences on the issues of screening and the administration of IAP. These differences are summarised in Table 1.
Table 1: RCOG and ACOG guidelines on previous GBS colonisation
|
RCOG 2017 Guidelines [5] |
ACOG 2011 Guidelines [6] |
Discuss option of IAP or late pregnancy bacteriological testing followed by IAP if positive. If desired, test 3-5 weeks before anticipated delivery for risk assessment.
Before testing by vaginal/rectal swab culture:
After testing by vaginal/rectal swab culture:
|
No routine IAP unless there is indication for GBS prophylaxis this pregnancy |
Why was IAP not given?
As our hospital is outside the USA or UK, we do not fall under the specific jurisdiction of either of these national guidelines. Our hospital’s management guidelines for GBS mirrors the ACOG guidelines but the clinicians in our hospital predominantly consist of members of the RCOG. This situation is not dissimilar to that of many other countries.
In accordance with our hospital guidelines, screening was scheduled at 36 weeks gestation for Mrs X, but she unfortunately did not attend for screening. Following the ACOG guidelines, Mrs X did not require IAP, as she was term and the guideline advises that she is unlikely to be colonised in subsequent pregnancies. With the fetal growth restriction at term indicating delivery, the absence of GBS testing was read in the context of the RCOG guidelines where universal screening is not advocated. This unfortunately misses the recommendations for previous GBS colonisation which is addressed in a sub-section, recommending counselling the pregnant woman to choose at that stage empirical IAP or repeat screening and delaying delivery for 24-48 hours prior to deciding on IAP. In addition, the option of offering nucleic acid amplification test (NAAT) for GBS is stated in the RCOG guidelines, but it is not available at our centre, further restricting the screening test options in this case. Where available, NAAT has been shown to be more sensitive than culture (73% vs 67%) in identifying GBS from vagina/rectal swabs [7]. Unfortunately, selective application of different guidelines resulted in poor outcome for the baby with GBS meningitis, a condition carrying 10-15% risk of mortality in developed countries with survivors having a 10 times higher risk of having moderate or severe disability than children who have never had neonatal meningitis [8].
Discussion
This case serves to illustrate two points; the role of guidelines and the need for their application within their given context, and the importance of understanding the limitations of these guidelines.
CPGs have a dual role in medical malpractice claims. While offering a minimum standard of care, they also offer clinicians a defense when patients allege to a breach in the standard of care [4]. Studies have shown that the implementation of CPGs have improved clinical practice in medicine in general [9]. However, as this case illustrates, guidelines need to be understood and applied within their given context. While the ACOG adopts a more streamlined approach to have universal screening for GBS; with the assumption of compliance to screening, the RCOG seeks to exercise the principle of patient autonomy with the involvement of the patient in the decision for screening, with the option of retesting later in pregnancy if the patient was previously colonised. In retrospect, the perceptive clinician should have proceeded with IAP given the patient’s non¬compliance to screening, and the impracticality of retesting due to medically indicated induction of labour.
Secondly, clinicians should also be aware of the limitations of guidelines when applying them to their patients. CPGs offer suggestions in the management of the conditions they are targeted and written for, but rarely account for other co-morbidities or conditions that patients often present with in daily medical practice. In this case, fetal growth restriction necessitated induction of labor. Existing literature shows that babies that are small for gestational age, or that have severe intrauterine growth restriction, have an increased susceptibility to early infections, and even increased mortality [10,11]. While both guidelines did not necessarily dictate that the patient be given IAP, this was on assumption that it was a normal pregnancy. Given the above, the benefits of giving IAP appear to outweigh the risks of withholding it. A clinician should be acting in his or her patient’s best interest, by managing the different conditions they present with, and with an understanding of guidelines and their limitations, deliver a patient-centric management plan.
Conclusion
The case illustrates the importance of applying guidelines correctly within the appropriate clinical context but serves also as a reminder for clinicians to understand the limitations of them when accounting for other co-conditions patients often present with in daily medical practice.
References
- Lancefield RC (1928) The Antigenic Complex of Streptococcus Haemolyticus. I. Demonstration of a type specific substance in extracts of streptococcus haemolyticus. J Exp Med 47: 91-103.
- Lukacs SL, Schoendorf KC, Schuchat A (2004) Trends in sepsis-related neonatal mortality in the United States, 1985-1998. Pediatr Infect Dis J 23: 599-603.
- Ohlsson A, Shah VS (2014) Intrapartum antibiotics for known maternal Group B streptococcal colonization. Cochrane Pregnancy and Childbirth Group, ed. Cochrane Database Syst Rev CD007467.
- Mackey TK, Liang BA (2011) The Role of Practice Guidelines in Medical Malpractice Litigation. AMA J Ethics 13: 36-41.
- Prevention of Early-onset Neonatal Group B Streptococcal Disease: Green-top Guideline No. 36. BJOG Int J Obstet Gynaecol 2017. 124: e280-e305.
- American College of Obstetrics and Gynecology. Prevention of Early-Onset Group B Streptococcal Disease in Newborns. Committee Opinion No. 485. Obstet Gynecol 2011. 117: 1019-1027.
- Couturier BA, Weight T, Elmer H, Schlaberg R (2014) Antepartum Screening for Group B Streptococcus by Three FDA-Cleared Molecular Tests and Effect of Shortened Enrichment Culture on Molecular Detection Rates. J Clin Microbiol 52: 3429-3432.
- Ku LC, Boggess KA, Cohen-Wolkowiez M (2015) Bacterial meningitis in infants. Clin Perinatol 42: 29-45.
- Grimshaw JM, Russell IT (1993) Effect of clinical guidelines on medical practice: A systematic review of rigorous evaluations. Lancet Lond Engl 342: 1317-1322.
- Singh M, Manerikar S, Malaviya AN, Premawathi null, Gopalan R, et al. (1978) Immune status of low birth weight babies. Indian Pediatr 15: 563-567.
- Ludvigsson JF, Lu D, Hammarström L, Cnattingius S, Fang F (2018) Small for gestational age and risk of childhood mortality: A Swedish population study. PLoS Med 15: e1002717.