
Archivos de Ciencia e Investigación(ADCI)
ISSN: 3068-014X | DOI: 10.33140/ADCI

Review Article - (2026) Volume 2, Issue 1
The Role and Importance of Women in the History of Medicine since Late Middle Age to the Contemporary Times
Received Date: Mar 17, 2026 / Accepted Date: May 15, 2026 / Published Date: May 25, 2026
Copyright: ©2026 Gustavo Gomez Barbieri. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Barbieri, G. G. (2026). The Role and Importance of Women in the History of Medicine since Late Middle Age to the Contemporary times. Arch Cienc Investig, 2(1), 01-14.
Abstract
Within the history of medicine, women have played a key role in a masculine and patriarchal paradigm, innovating and developing areas of medical knowledge that men had considered limited for ethical, cultural, anthropological or religious reasons. Therefore, the aim of this publication is to explain and describe the role of women into the Medical system and their contribution to the history of medicine, and how their discoveries and innovations have changed the world.
Keywords
Medicine, Woman, History of Medicine, Gender Equity and Social Justice
Introduction
Along the Middle Age the women are considered a secondary person, delimited by the masculine power and the social paradigm based in the longue durée of the male construction of female physiology which aims at reducing its identities, explained by the theories of errands womb and the humidity humours who influenced the fluctuate character of the women and the migration the uterus to the brain, explained the hysteria and the female depression in this theory and the aristotelian theory of humours [1,2].
This phenomena of the marginalization is explained in the middle age by the theories of migration of the uterus to the brain and the extraction of the “Pietra della follia”, where the women are more weak and susceptible like the men in the influence uranics and pneumas who transforming at women a Histérica or stulta, like sinister the extraction of the rock of the madness, In the picture of Hyeronimus Bosch, flamingo painter, the nun are observing the medieval neurosurgeon with the book and the religion awaiting to the surgery cure the stultus, explicit the ignorance and critic the medical model and the church, situating in a position of the unknowledgeable, in the same situation the surgeon with the wears a funnel-shaped headdress, a symbol of stupidity, used here as a harsh criticism of those who claim to know but are ultimately more ignorant than the one they are supposed to cure of “madness. ”This position of the nun is observing a process of marginalization to the sinister site and passive expression of unhumble and apathetic to the medical condition and medical procedure respect to the treatment of mental disease [3].
A starting point for hospitalization and the treatment of diseases lies in the need to bring together in one physical location all those patients who, due to the severity of their illnesses, could not be treated at home or on an outpatient basis. Such facilities require a primitive nosocomial structure. The fulfilment of an organization designed for shelter, classification and order generates a nosocomial structure managed with equipment capable of classifying, treating and resolving, within a given time frame, the situation of those who must be admitted to such a space. From the above derives an administrative and legal structure that provides the physical location, whose space meets the requirements of protection, hygiene, and isolation [4].
The administrative indication rests on the donation of physical buildings donated by the aristocracy at the suggestion of monarchical governments. Thus, in the Elizabethan and Edwardian eras, these premises were adapted from country houses with their respective lands, from whose domains even the food resources necessary for the maintenance of the inmates were obtained. The physical structure was adapted to conditions of ventilation, circulation and lighting that changed the meaning of the hospitable shelter where one went to die, to a place where recovery of health was possible. It is at this point that the workforce necessary for the application of therapy and healthcare initially found support from the monastic orders, whose essentially religious mandate drove them to provide “pious” care for “those humans who suffer in imitation of Christ” [5,6].
Despite the establishment of this modus operandi for the benefit of civility, instigated by the self-interest of those aristocrats who are unable to maintain the high cost of property maintenance and who, through this loan for use, benefit personally, graced by the crown and the Christian mandate to protect their neighbours, it is the sum of the legal, anthropological, medical therapeutic and social factors laid the foundations for the development of a form of medicine that would be valued over time and would mutate into specialized structures for the care of patients with increasingly complex diseases, as well as into centres Training and specialization for those working in the medical field who, through their expertise, lay the foundations for what we know as modern medicine.
The dark atmosphere, certainly where one would die in the Middle Ages under this new conception, benefits from a shift that not only affects those inside, but also those who apply the therapy to the patient’s families and those who govern their subjects with a new sense and maintenance of responsibility. The categorization of the procedures and functioning of primitive hospitals requires ‘specialised personnel’ in each of the functions inherent to their structures and functionality. It is for this reason that religious order and structures, whose functionality is mandated by creed, take on the rationale and purpose of their institutionality from the direction, administration, treatment, and management of patients. The wealth of therapeutic experience flows from the Crusades and the management of the bubonic plague. The first surgeons did not hesitate to use equipment that they did not hesitate to use, and it is for this reason that these primitive nurses learned certain procedures in support of the therapy aimed at curing diseases and injuries, and in whose operation they developed an expertise that allowed them to pass on to other women who, despite being laywomen, recently received this influence and increased the number of personnel who were most in demand, since diseases that were not treated in the past improved in their approach and feasibility of improvement thanks to better study and understanding. Function of the time of the object of greater demand, since diseases that in the past were not treated, at that time improved their approach and feasibility of improvement thanks to a better study and understanding of medicine as a reproducible scientific discipline, and in whose essence is research and the development of knowledge and transmission and advancement for multiple scientific fields of the society of the era [7].
From this point onwards, the establishment and assignment of roles and tasks becomes an integral part of a formal guide on practical and epistemological organization, through which the functionality of medicine as a formal science establishes channels of communication and feedback within the social corpus of the hospital institution. From now on, doctors and nurses will recognize each other as complementary and justified in their joint work. The scope of action of each will be well defined, and neither party will attempt to encroach on the other’s specialisation. From now on, due to scientific advances, each profession will demand greater specialisation and depth in [8]. The acquisition of new knowledge, then, does not rest on specific roles but on the development of science itself; it is episteme and nosology that develop fields of value, building bridges of conversation between different specialities. Over time, this communication converges on the point that the ‘curative issue’ and the well-being of patients guide the work of each of the branches of pro hominem medicine [9].
However, prior to this advent, women had to navigate a more murky than clear zone. For this reason, the first female medical students, after having fought and gained admission to teaching institutions, also had to fight against this ancestral knowledge, which they felt hindered by their own patients’ refusal to be treated by female doctors. This transitional situation was evident in Germany, where this difficulty led to an accommodation mediated by the presence of male medical tutors who accompanied the students at all times [10].
There are now many women who are spearheading the way forward for new generations of female doctors and researchers. Their presence across different specialities dates back to the middle of the last century, with developments in labor and occupational medicine, where they provide cognitive and pedagogical expertise based on research and innovation in these areas. At this point, it is worth asking: what is the medical specialty preferred by women? What is the medical specialty preferred by men? If women opt for internal medicine or obstetrics and gynecology, men will lean towards general surgery and cardiology. Could it be that the old norms still prevail in the diversification and channeling of the ‘activating energy’ that inclines one or the other towards a particular choice? We should not view the division of labour as an area of competition between the two. Rather, we should focus on the complementarity of functions in relation to the personal and particular skills inherent in the individuals in question. Then, certain areas of intervention may be more or less favorable for some than others, without detracting from the real intention of work or love for the profession, but quite the contrary, focusing all that love on doing good to those who are the object of therapy, in any case the patient from now on, and not on the selfish exercise of the profession, in achieving personal professional accomplishments that only contribute to the aggrandizement of the ego, destroying the true meaning of the most Humanistic of professions. In these senses this work proposes an integral vision to explained since a history and anthropological and social vision the role of the medical women in the actual society and the possible role who developed in the contemporary society.
Evidence Acquisition
This literature review aims to illustrate, compare, and discuss the role and the importance of the figure of the woman in the development of the Medical system. To achieve this goal, we adopted the Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA] methodology. First, we defined a list of keywords that express the main aspects of the concepts of (“Female History, Ancient* Humans Medical doctor *She doctor / history* Natural / history Nurse’s Role / history*middle age*medieval history *rinasciment history *Victorian history *Labor and occupational era *Contemporary history. Only articles in languages other than English, Spanish, and Italian were excluded. Once the information was obtained, two independent observers, whose names were concealed, carried out a critical analysis of the referenced documents. The original documentary archives of the Congress Library of USA and Ambrosian Bibliotheque were consulted to obtain primary sources for a more in-depth analysis (You can see box and fig.1 for more information).
|
Question Research |
Mesh terms |
Citation |
|
¿What's the role of women in the medical systems around the history of medicine? |
Medical doctor/woman Health system History, Ancient* Woman in medicine Midwifery / history* Late Middle Age. Renaissance era. Victorian era. Laboral Medicine Occupational medicine Contemporary medicine |
1-10 |
|
¿What are the principal discoveries and supports who developed in the history of medicine? |
Humans Midwifery / history* Natural Childbirth / history Nurse's Role/history Natural Childbirth / history Nurse's Role / history* |
11-35 |
|
¿What are the principal cultural factor who determines the role of the women in the health system? |
History of Medicine anthropology philosophy epistemology |
36-39 |
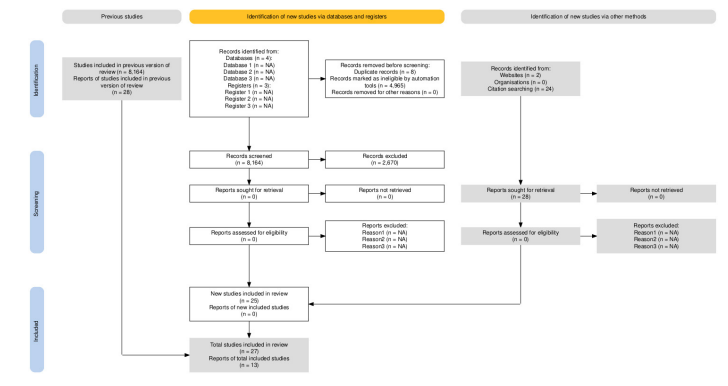
Figure 1: Diagram Flow Chart Selection and Inclusion Articles
Methods
We conducted a scoping review of the literature on the role of the women in the medicine , following the Preferred Reporting Items for Systematic review and Meta-Analysis extension for Scoping Reviews (PRISMA -ScR ) guidelines. A pre-search scoping protocol was designed based on the approach suggested by Arksey and O’Malley and The Joanna Briggs Institute (2015). The PRISMA-ScR checklist and protocol are available in the supplementary materials [11,12].
Eligibility Criteria
Current recommendations are as follows: the inclusion criteria of scoping reviews should be based on the mesh terms that can answer the study questions, the concept to be examined, and the context in which the review takes place. In our review, we applied the following inclusion criteria:
• Primary Historical Studies: Three main questions were structured. What’s the effect of the cultural system in the generation and role of the woman doctor in history? How to influence the organization of the healthy system and the relevance and impact of the envelopments realized by the woman in the medical clerks? We considered the terms of the mesh:
History, Ancient* Woman in medicine Midwifery / history*
Natural Childbirth / history Nurse’s Role / history*
Late Middle Age.
Renaissance era.
Victorian era.
Laboral Medicine Occupational medicine Contemporary medicine
Only articles in languages other than English, Spanish, Latin, Greek, French & Italian . Once the information was obtained, two independent observers, whose names were concealed, carried out a critical analysis (Please review box 1 and 2)
•Secondary historical studies: Autobiographies, historical writings (books and articles/letters) and comments, tributes, photographic archives, legal codes of the time and their translations, study articles, and academic programs following the scoping review methodology with the questions raised were considered among this group.
Anticipating a low number of studies, we kept our review as inclusive as possible; therefore, we have included any type of study design, including qualitative analyses, ethnographies, case studies, and observational and analytical studies.
Information Sources
Our research included standard databases as well as other sources of information. The standard databases included PubMed, Epistemonikos, Lilacs, Scopus, and Google Scholar Review. A Scoping Review has been conducted over the past 70 years. We also search Memories, the National Archives, the Library of the Congress Library with unpublished books and documents, and Sky. Finally, we established direct contact with local mental health stakeholders, including policymakers, clinicians, and service users via email.
Search Strategy
To make our search as complete as possible, we include terms with no language or time restrictions. We use diverse terms like (“Story/Medicine” AND “Woman”) OR (“Medieval history” AND “Medical doctor”) reporting the strategy of search with another time epochs (Figure 1).
Selection Process
Two assessors independently reviewed the titles and abstracts and compared them to the inclusion criteria. Disagreements were settled by consensus or by a discussion with a third reviewer if no consensus was reached.
Data Extraction and Management
An extract of data was developed from the Implementation Studies Checklist for Reporting Standards and the framework developed by Proctor et al.. Accordingly, for each included study we extracted general characteristics, such as study type, country, and participants, as well as implementation methods and outcomes, such as acceptability, feasibility, fidelity measures, effectiveness, profitability, and sustainability. A detailed taxonomy is included in the supplemental documents. The data were extracted by one team member and verified by another writer.
Body of Evidence
Role of the Medical Woman in the Late Middle Ages
Women were prominent in daily care because health care was largely a preventive activity that took place in domestic and domestic settings. Medical knowledge was as dynamic and fluid then as now, but therapeutic ideas in the Middle Ages were often transmitted orally and through informal, apprenticeship training. The human body was commonly believed to consist of four fluid humors-blood, phlegm, black bile and yellow bile-that fluctuated in relation and proportion to various internal and external factors. Since health and disease depended largely on humoral excesses or deficiencies, the physicians’ task was to moderate the humors in search of balance. They manipulated the humoral flow through bloodletting, emetics, purges and other manipulations of the body.
In the same year the Universitas studiorum of Paris created the obligation to obtain a licenciature and official certification of the university to work and exercise the profession. In this way the legal process Against Felicia di Barbone marked a high in the history of medicine condemned at not exercising the profesión of women doctor in Europe. The principal entity certificated was the Paris University [13].
However, this did not wipe them entirely from existence or from the practice, given that a reasonable number of names can be found in the Italian records alone. These include Monna Neccia, mentioned in the Estimo tax register in 1359, and Monna Iacopa, who treated plague victims in 1374. Both were from Florence, as were the ten women enrolled between 1320 and 1444 in the city’s guild of doctors, the Arte dei Medici e degli Speziali. In records from Siena, Tuscany, we find mention of Agnese and Mita, who were remunerated by the city for their services in 1390 [14].
All the same, it had become very dangerous for women to practise medicine, particularly due to the ever-mounting suspicions of witchcraft. There is an unfortunate lack of data about these women in the official sources, given that they practised at a time when society permitted only men to access more senior positions. The women provide a structure of healing and cure working in unofficial structures, practicing the medicine in houses and in the convents. Second Genieves Dumas, of the 34 cases involving health recorded in the Register of Pleas of the Parliament of Paris 1364-1427, eight cases concern women. Two of these cases are particularly interesting because they provide us with extensive information on certain aspects of women’s medical practice in the Middle Ages. The first is that of Perette la Petone, a surgeon, who was brought to justice by the Parisian surgeons’ guild for the illicit practice of surgery, and the second is that of Jeanne Pouquelin, a barber, who was prosecuted by the Parisian barbers’ community for the illicit practice of barbering.
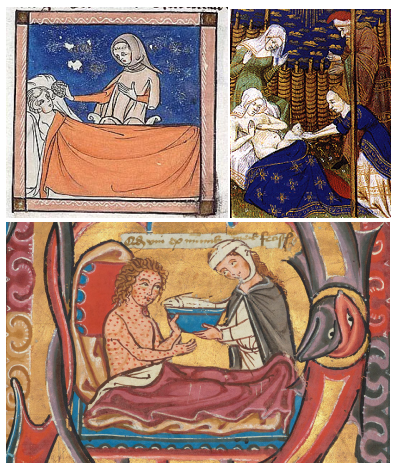
Figure 2: a.) A woman feeding a leper, from the 13th-century, b.) the midwives and nurseries in the birth of a child, and the c.) nursery’s activities in the middle age era. Benedictine psalter, Switzerland. Courtesy the Getty Museum LA
In closing, we must list some of the elements that this study has brought to light. Regarding barbering, the pleadings indicate quite precisely the terms of the sufficiency check. Applicant barbers must spend an eight-day training period with each of the four master-jurors of the trade; they must make suitable lancets, must know how to bleed and shave, and know everything related to the veins of the human body. Female barbers, as in many Parisian trades, can inherit the business, but they must not perform surgery and cannot train their apprentices themselves.
Regarding surgery, a rereading of the legislation shows us that surgeons not only must be literate, but it is very likely that some of them must read Latin. The abundance of legislation in Latin concerning them would otherwise make no sense. While this fact brings them considerably closer to masters of medicine, it does not make them clerics. Their social status is therefore quite precarious since they fit poorly into the Parisian hierarchical structure.
Can this help explain the abundant legislation concerning them and their attempt to equate the apprenticeship of surgery with university teaching? In this case, it seems that surgeons have every interest in keeping women away from the practice. Because the hierarchy structure of the church and eclesial order, explained a social phenomenon of the emergency of the new millennia and the universal judgement, coincidence with the crusader and the epidemics waves of lepper and the pest obligate the professionalization and the regulation in the medical education and the acknowledge in materia medica, in consequences to the emergency of healers , curandera and barbers who hasn’t been a ufficiale and certificates education who is the case of the women Barber Pouquelin, who likes another barber don’t understand the Latin language and the official medical treatise of the era, and only known the French in a book of remedies.
This difference between the medical doctors versus barber surgeons are noted by the difference between vernacular knowledge who is deprecated against the academic knowledge ricoverated by all wisdoms men’s to the city of Constantinople and the Arabs in the Grecian tratados of medicine and transcript by benedictinean monks in the scriptorium. This difference marked a clear separation between the official medical surgeons and the vernacular or popular medical doctors.
The Role of the Woman Doctor in the Renaissance
The creation of academies and Gilda’s of workers argued on ‘Gremios’ transforming the mentality and the concept of Artisanal work, workers in liberal association of workers with laws and rules. After all the Black death and the plagues the women in medicine suffered a hard persecution occurring during the 13th to 18th century. Women are delegated a second plane and edge out the formal medical education in England and France. The law reforming is stable in prohibiting the women to practice medicine. After all, the influence of the ecclesiale order in the organization of the University modulated the Formation and the medical school.

Figure 3: The therapeutic and the cure of patients are in the hand of nuns nurseries administered and prepared in the monastery extension in the xenodochyum and hostess
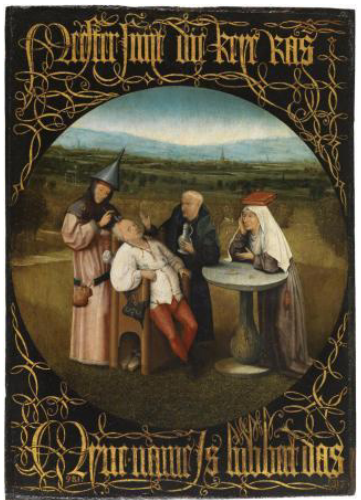
Figure 4: The extraction of madness stone. Hieronymus Bosch. Museo del Prado.
The role of the nuns’ nursery like apothecaries in the pharmacy church has transformed the concept of erbaristic and plant houses where. The medical doctors and the patients had been obtaining his medicines, a difference of the Middle age was the curandero or the errant barber treated in situ her pathology. In the newborns are the midwives and nurses who dispense the medicines. An Example of this practice was Christina Hatesko-Fortuna (1698_1771) who studied medicine and treated eye disease, without giving importance to social classes in a wide area. The colirios and the medicines are effective by young and old witnesses.
In Italy the medical revolution and the academy showed important advances in the anatomopathology and embryology with the works of Anna Morandi Manzolini (1714–1774) married the Bolognese artist and anatomist Giovanni Manzolini and became not just his spouse and mother of their children, but also his colleague. The couple worked on the production of anatomical wax models, first in collaboration with the artist Ercole Lelli on a papal commission for the University of Bologna’s Anatomy Museum. After a disagreement between Lelli and Manzolini, Morandi and her husband pursued anatomical dissections and wax model production in their home laboratory. Over time they had legal access to more than a thousand unclaimed bodies delivered from the public hospitals of Bologna, finally she transformed the history of medicine created the first anatomic cabinet who transformed the medical education integrated the manual artist abilities with the anatomical and medical knowledge with the work in wax re-laborating the medical practice with the anatomy wisdom.
The role of the woman doctor in the Victorian Era
After all the deep reform of the church and the emergencias of absolutista monarchy accelerated the conversión the all leprosaries and monastery and church in the medical hospitals administered by the crown. In América the discovery of news dispense like the syphilis and cólera accelerate the institution of Protomedicate rigged by Royal audience in the Colonial America incorporated the all nuns and monks in the medical attention with a cultural syncretism and the emergency of francmassonery in France and England , transform the society current of intellectualism and illuminism in the XVII to XVIII sicle, explained by the transformation of rural society to the Urban society, with the envelopment in the wealth and living conditions of farmers, the growing of metropolis provocated epidemies and pest for the antihigienic conditions, the latrines área verted directly in the street, in the middle of the street the black waters flew in canals Open to the population and the saddleries verted directly their caustic waters with foam and hair of animals, with extreme cases to throw away the corps of death animals and the animals living into the houses.
In Elizabethan times, women could not exercise their rights independently; they had to be represented by their husband, father, or brother, and any decision they made regarding their destiny had to be approved by one of these actors. Their economic and intellectual rights were restricted by limitations that seem unacceptable to us today. It can be deduced from the above that the presence of women in medical training centers was an expression of the conformity of many social actors, with mores and ancestral knowledge that had to break down barriers that shifted in tandem with psychosocial thinking and a clinging to Puritan institutions that blended rationalist intellectuality with religious sociocultural knowledge, adding to the difficulty of acquiring knowledge, sociological barriers rooted in the popular consciousness.
|
Medical women |
Contribution |
Cite |
|
Felicia di Barbone |
Demonstrate the legal possibility to exercise medicine in France. She defeats the medical society and traditional system explained the medical practice and barber surgery exercises in the late middle age explained in vernacular language and not Latin her practice. |
8.Dumas G. Les femmes et les pratiques de la santé dans le “Registre des plaidoiries du Parlement de Paris, 1364-1427” [Women and the practice of health in the “Register of counsels’ speeches in the Parlement of Paris, 1346-1427”]. Can Bull Med Hist. 1996;13(1):3-27. French. doi: 10.3138/cbmh.13.1.3. PMID: 11613340. |
|
Christina Hatesko-Fortuna |
Barbro Christina Hastesko-Fortuna treated eye diseases in all social classes in a wide area. Her function was examined in 1769 by request of her son at a session of the Porvoo District Court. The Court issued a laudatory statement. The medicines prepared by her were effective as testified by both young and old witnesses, particularly when they were used according to her instructions. |
Makela-Alitalo A. Barbro Christina Hästesko-Fortuna (1698-1771) kartanonrouva, kansanparantaja [Barbro Christina Hästesko-Fortuna (1698-1771), lady of a manor and physician]. Hippokrates (Helsinki). 1998;(15):136-8. Finnish. PMID: 11625415. |
|
Anna Morandi Manzolini |
Anna Morandi Manzolini (1716–1774) was an Italian woman from Bologna who became famous for her anatomic wax models that were used for teaching anatomy. The embriology, replicas of organs and organ systems. These included the muscles of the pharynx, and such minutiae as the extrinsic ocular muscles and the parts of the external, middle, and internal ear. These last were much enlarged compared to the original, and could be disassembled. |
Rosito P, Mancini AF, Ruggeri F, Paolucci G. Anna Morandi Manzolini (1716-1774) master sculptress of anatomic wax models. Pediatr Blood Cancer. 2004 Apr;42(4):388-9. doi: 10.1002/pbc.10011. PMID: 14966839. |
|
Maria Colinet of Bern |
She was a famous historical Swiss midwife-surgeon active in the late 16th and early 17th centuries, notably known for assisting her husband in his surgical practice in Bern and performing the first successful Cesarean section in Switzerland in 1603. She is recognized for her skills in obstetrics and surgery, treating fractures, and performing C-sections. |
Zuskin E, Pucarin-Cvetkovic J, Schachter, et al. E. Women in medicine through the ages / Le donne in medicina attraverso i secoli. Med Lav [Internet]. 2008 Nov. 1 [cited 2025 Sep. 10];99(6):407-14. Available from: https://www.mattioli1885journals. com/index.php/lamedicinadellavoro/article/ view/1593 |
|
Lady Mary WortleyMontagu |
Lady Mary Pierrepont—her maiden name— was born in London in 1689. She was the daughter of Evelyn Pierrepont, Herald of Kingston, a member of Parliament and a member of the Reform Party. After a responsible aristocratic upbringing, her brother died of smallpox at an early age, and she survived two years later, with a severe illness. No one expected her to take up the diplomatic mission in Constantinople, Turkey, where she revived the technique of grafting, the first vaccination with scabs from infected cattle pustules, applied with a needle into a wound in the arm. This first medical demonstration with two medical observers in a group of prisoners and orphan children demonstrates the efficacy of the first documented vaccination in history. |
Gallanti, L. (2021, August 26). Mary Wortley Montagu, pioniera contro il vaiolo. National Geographic Storica. https://www.storicang. it/a/mary-wortley-montagu-pioniera-contro-il-vaiolo_15301 |
|
Marie Margherita Beheron |
Marie Marguerite Bihéron (November 17, 1719 – June 18, 1795) was a French anatomist, known for her medical illustrations and wax anatomical models. The daughter of an apothecary, she studied drawing at the Jardin Royal and with Madeleine Basseporte, of whom several anatomical representations survive. Support the work of Velloisin and John Hunter in anatomy. |
Boulinier G. Une femme anatomiste au siècle des Lumières: Marie Marguerite Biheron (1719-1795) [A female anatomist of the enlightenment: Marie Marguerite Biheron (1719-1795)]. Hist Sci Med. 2001 Oct-Dec;35(4):411-23. French. PMID: 11917918. |
|
Mary Walker Harriet Kezia Dorothy Reed Margaret Kennard Frances Morgan Elizabeth Walker Louisa Atkins Elizabeth Blackwell Elizabeth Garret Nadesha Prokofevna Suslova |
In the victoria era Blackwell and Garret created training schools for women in America and England.Established a Dispensary in a poor area of Marylebone in London for treatment of women and children of the lower classes beginning the period of social medicina. Elizabeth Garrett Anderson wasthe first woman in Britain to obtain the title ofM.D. but not the first in Europe. Nadesha Prokofevna Suslova was the first woman to obtain the title of M.D. in Russia in 1867. Margaret Kennard also took in the aspirant medical women Frances Morgan, Eliza Walker and Louisa Atkins. Garrett Anderson, Jex Blake and Blackwell worked together to set up the London Medical School for women in 1874 |
Zuskin E, Pucarin-Cvetkovic J, Schachter, et al. E. Women in medicine through the ages / Le donne in medicina attraverso i secoli. Med Lav [Internet]. 2008 Nov. 1 [cited 2025 Sep. 25];99(6):407-14. Available from: https://www.mattioli1885journals. com/index.php/lamedicinadellavoro/article/ view/1593 |
|
Florence Nightingale Kate Hurt Mead |
Florence Nightingale is the most famous medical nursery who created the first cure and preventive system to care for the patients in the battlefield of Crimea beginning the statistical analysis of diseases. Dr. Kate Campbell Hurd-Mead was a health care pioneer and an advocate for women in the medical profession. She was born in Danville, Quebec, in 1867 and grew up in Newburyport, Massachusetts. She decided to study medicine out of respect for her father and on the advice of the well-respected woman physician, Dr. Mary Putnam Jacobi. |
Appel TA. Writing women into medical history in the 1930s: Kate Campbell Hurd-Mead and “medical women” of the past and present. Bull Hist Med. 2014 Fall;88(3):457-92. doi: 10.1353/bhm.2014.0050. PMID: 25345770. Turkowski Y, Turkowski V. Florence Nightingale (1820-1910): The Founder of Modern Nursing. Cureus. 2024 Aug 5;16(8):e66192. doi: 10.7759/ cureus.66192. PMID: 39233972; PMCID: PMC11373583. |
|
Maude Abbot |
Canadian-born Maude Elizabeth Seymour Abbott (1869–1940), a physician and student of the great physician William Osler, produced her most important book in 1936, “Atlas of Congenital Cardiac Disease,” one of the foundational works of modern cardiology. The atlas examined 1,000 cases she personally studied and included an analysis of the development and comparative anatomy of the hearts of reptiles, amphibians, and mammals. Kathleen Smith quotes Abbott as saying that the atlas “appeared as a preliminary to an even larger volume that was in preparation.” |
Wright JR Jr. Maude Abbott: “A Feminine Misfit in an Exclusive Male Environment” and Her Strategies for Success. Pediatr Dev Pathol. 2024 Nov-Dec;27(6):513-529. doi: 10.1177/10935266241281786. Epub 2024 Oct 1. PMID: 39351994; PMCID: PMC11568640. |
|
Sylvia Agnes Sophia Tait (8 gennaio 1917 – 28 febbraio 2003) |
This she medical doctor discovered the role and isolated the extract of aldosterona, named electrocortin since the compounds of 500 kidneys of bovines over to the exposition a diet high in potassium and low in sodium. |
Loriaux, D. L. (2003). Sylvia Agnes Sophia Tait 1917–2003. The Endocrinologist. https://doi. org/10.1097/TEN.0b013e31818b5d8a |
|
Julia Gwyneth Boamer Maria Gomirato Sandrici |
Geo-microbiologist at the University of California, Berkeley. She founded metagenomics, an approach based on sequencing the genomes of microorganisms directly in their natural environment, and invented metaCRISPR, a way to edit entire microbial communities. |
Cojazzi, L. (2021, May 2). Alice Augusta Ball, una chimica contro la lebbra. National Geographic Storica. https://www.storicang.it/a/alice-augusta-ball-chimica-contro-lebbra_15186 |
|
Jennifer Doudna Emmanuelle Charpentier |
Winners of the 2020 Nobel Prize in Chemistry for their work on CRISPR/Cas9 technology, are shining examples of women pursuing science. Actually the application in the genica therapy in Huntington disease and falciform anemia transforming the pronostici of the disease replacement the e on risponsable to the synthesis of anomalous malfor mated like the huntingtin protein or the synthesis of valine in replacement to the glutamic acid. |
Press release: The Nobel prize in chemistry 2020. (2020.). Nobelprize.org. Retrieved September 28, 2025, from https://www.nobelprize.org/prizes/ chemistry/2020/press-release/ |
|
Flaminia Cattericcia Jayme Locke |
Italian infectious disease specialist Flaminia Catteruccia at the Harvard T.H. Chan School of Public Health (Boston, Massachusetts) has conducted research on the reproductive behavior of Anopheles gambiae mosquitoes, demonstrating that the semen deposited by male mosquitoes after mating is essential for efficient reproduction. Knocking out a male enzyme involved in reproduction through RNAi (a mechanism by which certain RNA fragments can interfere with and shut down gene expression) can have a significant impact on mosquito populations, such as the release of sterile males. American surgeon Jayme Locke of the University of Alabama at Birmingham (USA) has pioneered xenotransplantation. Locke has transplanted the kidneys of a pig edited with ten key genetic modifications (10-gene pig) for the first time in a pathogen-free facility into a brain-dead human, keeping him artificially alive for a few days for research purposes with family consent. These exciting results demonstrate how xenotransplantation could address the global organ shortage crisis.1 |
Peng, D., Marrogi, E., Nelson, E., Liu, Q., Rinvee, T. A., de Vries, L. E., Thornburg, K., Singh, N., Shaw, W. R., & Catteruccia, F. (2025). OocystMeter, a machine-learning algorithm to count and measure Plasmodium oocysts, reveals clustering patterns in the Anopheles midgut. In bioRxivorg. https://doi. org/10.1101/2025.06.28.662088 |
|
Maria Teresa Ti |
Lepetit employees isolate the bacterial strain that produces rifampicin. Thanks to collaboration with Vladimir Prelog and mass spectrometry analysis, they manage to modify the molecule’s original structure and improve its antibacterial efficacy, making it a cure for two serious diseases: leprosy and tuberculosis. |
Attidellaaccademialancisiana.it Alpigno, M. (n.d.). Atti della Accademia Lancisiana -Numeri della Rivista. Attidellaaccademialancisiana. it. Retrieved September 28, 2025, from http:// www.attidellaaccademialancisiana.it/476/19/ articolo/Il-Morbo-di-Hansen-nella-storia-della-Dermatovenereologia |
|
Alice A. Ball |
Note for the invention of the CRISPR Chip, a biosensor that uses the nanoelectronic system to detect mutations in DNA samples and which could be used to diagnose genetic diseases, detect infections, and evaluate the efficiency of genome editing techniques. |
Cojazzi, L. (2021, May 2). Alice Augusta Ball, una chimica contro la lebbra. National Geographic Storica. https://www.storicang.it/a/alice-augusta-ball-chimica-contro-lebbra_15186 |
Role of the Medical Women in the Occupational and Labor ( XVIII and XIX Sicle)
By the mid-19th century, the dehumanizing influence of the materialistic period had led to the utilitarian conditions of human beings as instruments for the development of a capitalist policy that based its further development on the industrial foundations created by ‘developers’ with a purely functional interest in the existence of men and their exploitation, in order to increase wealth and capital goods.
The institutionalization of organizational labour, no longer confined to male castes but extending to the female workforce and the exploitation of minors, is changing the social and cultural environment to such an extent that normal conditions for human development are being damaged and destroyed by slavery labour. It is at this time that the hidden demand for particular interests urges civility to find an escape valve for painful situations that undermine the human condition. It is within this territory that the first social and trade union movements emerge, focused on improving working conditions for actors - producers.
The Role of the Medical Women in the XX Sicle
Well into the 20th century and after the Second World War, women have gained their place through mechanized work and in different productive areas. They are no longer seen as the weaker sex, as they have amply demonstrated their ability to tackle tasks that were previously “reserved” for men. Due to the shortage of male labour caused by the global conflict, they had to step in as a replacement workforce to make up for the loss of lives on the front line and to take on productive tasks related to the metalworking and arms industries. This ‘new deal’ led to the realization that no task should be off-limits to anyone, and it was from then on that women recognized themselves as capable of tackling any challenge, especially when the sacrifice of male lives as a result of the armed conflict demanded it. Now the medical profession is no longer taboo for anyone. Medical schools open their doors so that anyone with a vocation and, in many cases, money, can attend and demand medical instruction. Some specialties remain largely ‘reserved’ for male applicants, but the space gained with great effort over centuries is bearing fruit with the presence of women in many areas where they demonstrate great vocation and expertise [15-18].
Discussion
This Scoping review article showed the greatest difference between the masculine production history article and the female production article. The majority of articles written focus on the technical and research advances and achievements of male doctors compared to female achievements. Of the 8,164 articles reviewed, only 529 (9.6%) articles that responded to our research question in a generic way, and only 35 (6.6%) articles responded fully, focusing on technical and scientific achievements and gender differences observed in different historical periods. We must expand our search to unofficial sources of information such as bibliographic seminars and conferences where their contributions are recognized and discussed.
The quality of the evidence found was not high. In most cases, 20% of cases had a level of evidence of type ' [narrative review and meta-analysis] and 68.57% had type B [cross-sectional and case-control studies, analysis of clinical trials] and Type C and D, which included newspaper articles, bibliographic seminar proceedings, editorials, and opinion articles, as well as grey literature (2 cases), accounting for 11.42% of the total articles screened.
This results concording with the study of Flaminio Squazzoni et al and Xuang Go et al who demonstrate that the women who are listed as authors of published scientific articles are significantly fewer than men, particularly when looking at the number of first authors, who account for only 36.9% - a figure that indicates that far fewer women than men advance to senior positions, compared to the overall number of female scientists. Furthermore, women are called upon by publishers to be reviewers in much smaller numbers than their male colleagues, accounting for only 24.5% [19,20].
The last inform of UNESCO the Gap gender its must be reduced in the approximately decades because the emergency of new jobs transforming the mentality and the access of the women in the STEM work, gender inequality through a more utilitarian lens, focusing on the economic contribution of women in what we might call the Fourth Industrial Revolution. Of the children currently entering school, 60% will do jobs that do not yet exist. In this scenario, focusing on greater inclusiveness and equality is essential in order to keep pace with the times and ensure technological progress.
A 2017 study found that closing the gender gap in STEM education would have a positive impact on economic growth in the EU, contributing to an increase in GDP per capita of 0.7–0.9% across the bloc by 2030 and of 2.2–3.0% by 2050. The study predicted a closure of the gender pay gap4 by 2050,by which time 6.3–10.5 million jobs should have been added to the European economy, about 70% of these occupied by women.
This evidence demonstrates second our narrative synthesis that the women in the Late Medieval transition to the Renaissance transforming the Artisanal and barber work, to the institution to the medical and profession allied in Gilda's and Gremios with a strong opposition of the Universities, in 16th to 17th era the women recovery the fields works with the creation of schools and anatomist cabinet where the manual works and the arts permit the dialogue between the women and men. This female power are transition in Victorian Era transforming the nuns to the first medical doctors, products the industrialization and industrial revolution the women winner laboral field position in England and United Kingdom where Elizabeth Blackwell and Garret were coinvolted in the creation of first Schools for women's permit diversificate in different specializations had been diversified in different areas of the medicine, conquest the areas of genetics, pediatric malformations, endocrinology, infectology and Public health, transforming the vision and the paradigm of the knowledge and the learning in science in medicine marked a continuing evolution between the roles of the women in the engagement to rights in social justice and gender equality. The social crisis provocated by famines, wars and pest development the social organization and includes the women in works and task were the men are hegemony.
Conclusions
The women in medicine marked a continuing evolution between the roles of the women in the engagement to rights in social justice and gender equality, developing new innovations and techniques that would not have been possible without the male and female complement. The patriarchal system has tended to prevent these innovations from flourishing, but women’s capacity for adaptation and resilience has allowed them to conquer these spaces that humanity needs. It is necessary to understand that the working environment must be collaborative among the different actors. The presence of men and women in different areas of development must be justified by an increase in the possibilities of obtaining different perspectives on the same problem. The approach to tasks aimed at resolving the problem should not be determined by the genderization of the strata, but should respond to purely academic and scientific criteria, whose goal should always be directed towards the implementation and development of tactics that are beneficial to patients. Cognitive or brain-hand interface skills should be analyzed in accordance with the personal skills of each of the practitioners involved in the clinic. Undergraduate practice will enable automatic responses to certain challenges.
It is necessary to understand that the work environment must be collaborative among the various stakeholders. The presence of men and women in the different development areas must be justified by an increased chance of obtaining different perspectives on the same problem. The approach to tasks aimed at solving the problem should not be determined by the gendered nature of the departments, but rather should respond to purely academic and scientific criteria, always focused on the implementation and development of beneficial tactics for patients. Cognitive skills, or those related to the brain-hand interface, should be analyzed in accordance with the personal abilities of each of the physicians involved in the clinic.
Practical experience gained during undergraduate studies will enable automatic responses to certain challenges. For this reason, it will be essential to have ‘teachers’ in each pillar of medical education, in order to correct any shortcomings early on and thus be able to categorise teams with maximum efficiency in continuous laboratory and operating theatre practice. Work teams should use disagreements as a source of improvement in the personal skills of each member, strictly adhering to abilities and not gender identification.
Understanding the above will lead to the stabilization of a work environment conducive to personal development with a non-competitive humanistic vision, focused on the patient and not on personal fixation. With clear and progressive academic goals and with students’ awareness of a thorough understanding of the ‘targets’ to be achieved, for a balanced development between academic training and personal development, with cultivation in the professional and inner world of the human being as a multidimensional being and not restricted to limited, non-transcendent planes.
The significance of medical applications to human reality, rather than to a dissociative structuralist view between patient and person, or between science and anthropology, will ensure that medicine endures as a sign of humanity and goodwill, rather than as a disposable instrument that can be surpassed over time and become obsolete and useless. but rather as an entity complementary to the condition of ‘permanent health’ that will lead to healthy and self-reliant longevity, productive and with valuable historical awareness, with method and validity in a generous subsistence capable of showing a possible future to new generations and in whose cardinal symptom true love between life and systemic human ecology can be found. Rationalization in the anthroposophical field will block the forced and competitive division between women and men and will propel change on a higher plane of human essence [21-36].
References
- Cilione, M., Iorio, S., & Gazzaniga, V. (2025). The medical origins of a gender stigma: the underestimation of women’s pain. Cogent Arts & Humanities, 12(1), 2469456.
- Lippi, D., Bianucci, R., & Donell, S. (2020). Gender medicine: its historical roots. Postgraduate medical journal, 96(1138), 480-486.
- Gazzaniga, V., & Cilione, M. (2016). Maschile e femminile nella trasmissione dei caratteri ereditari. Da Atene a Sparta. Medicina Nei Secoli, 28(3), 901-920.
- Bianchi, F. (2020). Dal xenodochium all’hospitale. Origini e sviluppi delle istituzioni ospedaliere nel medioevo. LA SOCIETÀ MODERNA E CONTEMPORANEA, 11-54.
- Szwach, A. (2017). “Doctor She”: Women Practicing Medicine in Renaissance England and Their Representation in the Drama of Shakespeare. Acta Philologica, 29.
- Bianchi F. View of healthcare and medicine in medieval western hospitals [Internet].
- Foucault, M. (2014). History of Madness in the Classical Age. Gallimard.
- Zuskin, E., Pucarin-Cvetkovic, J., Schachter, E. N., Mustajbegovic, J., Vitale, K., Deckovic-Vukres, V., ... & Jelinic, J. D. (2008). Women in medicine through the ages. La Medicina del Lavoro, 99(6), 407-414.
- Sabatini, S. (1994). Women, medicine and life in the middle ages (500-1500 AD). American Journal of Nephrology, 14(4-6), 391-398.
- Hege, I., Schüttpelz-Brauns, K., & Kiessling, C. (2022). How is the situation of women in leadership positions in medical education in Germany?. GMS Journal for Medical Education, 39(3), Doc36.
- Bello, A., Blowers, T., Schneegans, S., & Straza, T. (2021). 3. To be smart, the digital revolution will need. UNESCO Science Report: The race against time for smarter development, 2021, 109.
- Morais Maceira, H. (2017). Economic benefits of gender equality in the EU. Intereconomics, 52(3), 178-183.
- üller-Schubert, A., & Kox, W. (1999). Rahel Hirsch (1870–1953): The first Prussian woman medical professor. Zentralblatt für Chirurgie, 124(8), 756–761.
- Kaiser, W., & Völker, A. (1989). History of the Halle Ars medica Judaica. Zeitschrift für die gesamte Innere Medizin, 44(8), 241–246.
- Zielonka, V., Forsbach, R., Hofer, H. G., & Foelsch, U. R. (2022). Against oblivion: Remembering the first Jewish women doctors of the German Society for Internal Medicine. Deutsche Medizinische Wochenschrift (1946), 147(24-25),1596-1604.
- Squazzoni, F., Bravo, G., Farjam, M., Marusic, A., Mehmani, B., Willis, M., ... & Grimaldo, F. (2021). Peer review and gender bias: a study on 145 scholarly journals. Sci Adv 7 (2): eabd0299.
- Luo, X., Liang, B., Wang, Q., Li, J., Cambria, E., Zhang, X., ... & Xu, R. (2025). A literature survey on multimodal and multilingual sexism detection. IEEE Transactions on Computational Social Systems.
- Wynn, R. (2000). Saints and sinners: women and the practice of medicine throughout the ages. JAMA, 283(5), 668-669.
- Gagliardi, I. (2023). Anima e corpo: Donne e fedi nel mondo mediterraneo (Secoli XI–XVI). Garrocci.
- Dumas G. Women and health practices in medieval Paris. Can Bull Med Hist. 1996;13(1):3–27.
- i Pairet, M. C., & Muniz, F. S. (1999). Academic power versus feminine authority: the Paris Medical School against Jacoba Felicie (1322). Dynamis (Granada, Spain), 19, 55-78.
- Hildebrandt, S. (2011). The lady anatomist: The life and work of Anna Morandi Manzolini. The Journal of Clinical Investigation, 121(7), 2532-2532.
- Wright Jr, J. R. (2024). Maude Abbott:“A Feminine Misfit in an Exclusive Male Environment” and Her Strategies for Success. Pediatric and Developmental Pathology, 27(6), 513-529.
- Haddaway, N. R., Page, M. J., Pritchard, C. C., & McGuinness,L. A. (2022). PRISMA2020: An R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimised digital transparency and Open Synthesis. Campbell systematic reviews, 18(2), e1230.
- Dmytriw, A. A. (2015). Gender and sex manifestations in hysteria across medicine and the arts. European neurology, 73(1-2), 44-50.
- Werner, W. (2005). Witch trials in the Salem as a medical error. Witch hunts in the XVII century and the medical art. Medycyna Nowozytna: Studia nad Historia Medycyny, 12(1-2), 5-17.
- Cojazzi, L. (2021, May 2). Alice Augusta Ball, una chimica contro la lebbra. National Geographic Storica.
- Alpigno, M. (2018). Il morbo di Hansen nella storia della dermatovenereologia. Atti della Accademia Lancisiana.
- Peng, D., et al. (2025). OocystMeter: A machine-learning algorithm. bioRxiv.
- Hulst, R. V. (2024). The future of scCRISPR-seq (Doctoral dissertation).
- Loriaux, D. L. (2016). A biographical history of endocrinology. John Wiley & Sons.
- Appel, T. A. (2014). Writing women into medical history in the 1930s: Kate Campbell Hurd-Mead and” medical women” of the past and present. Bulletin of the History of Medicine, 88(3), 457-492.
- Turkowski, Y., & Turkowski, V. (2024). Florence nightingale (1820-1910): the founder of modern nursing. Cureus, 16(8).
- Rosito, P., Mancini, A. F., Ruggeri, F., & Paolucci, G. (2004). Anna Morandi Manzolini (1716-1774) master sculptress of anatomic wax models. Pediatric Blood & Cancer, 42(4), 388-389.
- Makela-Alitalo, A. (1998). Barbro Christina Hästesko-Fortuna (1698-1771), lady of a manor and physician. Hippokrates (Helsinki, Finland), (15), 136-138.
- OUVERTES, R. S. E. T. R., & DA COMPLETARE, P. E.T. R. Antiquity and the Shaping of the Future in the Age of Enlightenment L’Antiquité et la construction de l’avenir à l’âge des Lumières L’Antichità e la costruzione del futuro nel secolo dei Lumi.