
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2020) Volume 5, Issue 1
The Prevalence, Risk Factors, and Bacterial Profile of Cesarean Surgical Site Infections at a University Teaching Hospital in South Western Uganda
2Uganda Martyrs Hospital Ibanda, Uganda
Received Date: Jan 21, 2020 / Accepted Date: Jan 28, 2020 / Published Date: Feb 04, 2020
Copyright: ©Joseph Ngonzi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: The single most important risk factor for post-partum maternal infection is Cesarean section (C/S) with a 5-20-fold greater risk for infection compared to a vaginal delivery. Post Cesarean wound infection is diagnosed in 2.5 to 16 percent of patients. Early wound infections (in the first 24 to 48 hours) are usually due to group A or B beta-hemolytic streptococcus and are characterized by high fever and cellulitis while later infections are likely due to Staphylococcus epidermises or aureus, Escherichia coli, or Proteus species. Objectives: To determine the prevalence, risk factors and bacterial profile of wound sepsis following Cesarean at Mbarara Regional Referral Hospital (MRRH).
Methods: A cross sectional study of mothers who delivered by Cesarean at MRRH was conducted. Mothers were recruited consecutively until the sample size was achieved. The main dependent variable was wound sepsis confirmed by a positive culture for microorganisms.
Results: Of the 359 mothers recruited in the study, 54 (15.5%) developed Cesarean wound sepsis. The risk factors associated with post Cesarean wound sepsis were severe anemia, lack of preoperative antibiotics use, poor antenatal attendance, mothers referred from peripheral health facilities, abnormal Body Mass Index (BMI), diabetes mellitus, more than five vaginal examinations, prolonged rupture of membranes before C/S, and prolonged labour. Staphylococcus aureus was isolated in 48.2% of all the septic cases and most of the bacterial isolates were susceptible to ceftriaxone, ceftazidime, ciprofloxacin and nalidixic acid and resistant to penicillin.
Conclusion: The prevalence of post Cesarean wound sepsis is high with staphylococcus aureus being the most common bacteria isolated in infected wounds. Most of the bacteria were susceptible to third generation cephalosporins and quinolones. Antibiotics use was protective against developing wound sepsis.
Keywords
Uganda, Bacterial Profile, Susceptibility Patterns, Factors
Background
The clinical criteria used to define a primary superficial surgical site infection (SSI) include any of the following: a purulent discharge within 30 days from the superficial surgical site, organism isolated from an aseptically obtained culture of fluid or tissue from the superficial incision, the surgeon’s diagnosis of infection and a surgical site that requires reopening by the Surgeon and is culture positive or not cultured but patient has at least one of the following signs or symptoms; pain or tenderness, localized swelling, redness or heat (CDC, 2013). The rates of Cesarean SSIs in sub-Saharan Africa vary between 9-33% [1-4]. Women giving birth by Cesarean section have a 5- to 20-fold greater risk of postpartum sepsis than women giving birth vaginally [5]. The commonest post-delivery infections are endometritis (puerperal sepsis), surgical site infections (SSIs) and wound infections [6,7]. Postpartum sepsis is the commonest cause of maternal mortality at Mbarara Regional Referral Hospital (MRRH) in Uganda, causing 31% of all maternal deaths [8]. Independent risk factors for post caesarean SSIs include hypertensive disorders of pregnancy, contaminated wound, prolonged duration of operation and an operation performed by an intern or junior doctor [9].
Surgical site infections can be prevented by giving prophylactic antibiotics and strict adherence to antibiotic prophylaxis and infection control guidelines can reduce postpartum sepsis incidence by 70% [5]. Implementation of evidence-based measures such as prophylactic antibiotic administration before Cesarean section significantly reduces surgical site infections and as thus women undergoing Cesarean section should receive the prophylactic antibiotics [10,11]. Intravenous prophylactic antibiotics for Cesarean section given preoperatively compared with administration after cord clamp significantly reduces the incidence of surgical site infections [11]. World Health Organization (WHO) recommends use of pre-Cesarean delivery prophylactic antibiotics 30 to 60 minutes prior to operative skin incision to reduce the risk of postoperative infection [11-14]. We therefore set out to evaluate the prevalence, bacterial profile and risk factors of wound sepsis following caesarean section at Mbarara Regional Referral hospital.
Methods
Study Setting and Design
The study was a cross-sectional and 341 participants were recruited from Mbarara Regional Referral Hospital (MRRH) in Mbarara, Uganda. MRRH is an approximately 650-bed academic hospital affiliated with Mbarara University of Science and Technology (MUST). The current hospital policy is for women delivering by Cesarean to receive a single dose of pre-operative antibiotics (ampicillin or ceftriaxone), usually given within 30 minutes to one hour of skin incision. In addition, after Cesarean section women are treated with combination intravenous ceftriaxone and metronidazole for three days, followed by five days of oral cefixime. Microbiological evaluation of potential infections is not routine, but when requested, samples are processed at MUST’s teaching lab adjacent to MRRH [15]. For this study, wound sepsis was defined by a positive culture of fluid or tissue from the superficial incision for microorganisms.
Inclusion and Exclusion Criteria
All mothers who delivered by Cesarean and admitted on Maternity ward at MRRH were recruited into the study. Mothers who delivered by Cesarean at MRRH in postnatal ward from 3rd post-operative day till 30 days’ post-surgery and those readmitted on gynecology ward with Cesarean wound complications within one-month post-surgery were included into the study.
Sampling Procedure
Consecutive sampling method was used to enroll all mothers who met the inclusion criteria until the sample size was achieved; this was done daily in postnatal and gynecology wards. Patients were strictly recruited once. To avoid double entry, each participant was assigned a unique identification number and sticker on her medical documents.
Sample Collection
We obtained wound swabs, urine, blood, vaginal discharge swabs for the various laboratory tests from the mothers who were recruited into the study.
Data Collection
A pretested questionnaire was administered to the study participants by the principle investigator or research assistant after obtaining consent to the study. The questionnaire captured information including socio demographic characteristics, medical and obstetric characteristics. Through swabbing the infected wounds, we isolated and identified bacterial pathogens responsible for wound infections through microbiological laboratories. Antimicrobial susceptibility profile of the bacterial isolates was determined by disk diffusion
Laboratory Procedures
This was assessed by collecting exudate from wounds by use of swabs. The swabs were transported at room temperatures to the laboratory as soon as possible. Swabs were inoculated on chocolate, blood and MacConkey agar. Chocolate plate was placed in a candle jar and incubated it with other plates at 35-37°C for 24-48 hours. An additional blood agar plate was inoculated anaerobically at 35-37°C for 48-72 hours. Plates were examined aerobically for potential pathogens like Staphylococcus aureus, beta Hemolytic streptococci, Enterobacteriaceae, Pseudomonas aeruginosa, Acinetobacter species, Haemophilus influenza, and Streptococcus pneumonia. Anaerobes were also investigated from the plates that were prepared anaerobically.
Drug Susceptibility Testing Using Kirby Backer Technique
For antimicrobial sensitivity patterns, agar plates were uniformly seeded with a suspension of fresh isolates of bacteria of the same colony per plate. Antimicrobial discs of the right potency were then aseptically placed on the plate which was then incubated in a suitable growth environment overnight. Zones of inhibitions were measured in millimeters. The sensitivity was interpreted according to the inhibition zone sizes as sensitive, intermediate and resistant.
Study Variables
The dependent variable was wound sepsis following Cesarean at MRRH. The independent variables were maternal age, parity, education level, marital status, occupation, religion, parity, antenatal care attendance, number of vaginal examinations, BMI, Use of pre¬operative antibiotics, duration of rupture of membranes, presence of diabetes mellitus, indication for Cesarean, type of Cesarean, level of surgeon, referral status, presence of urine tract infection, HIV status, district of residence, HIV status, labour duration, surgical technique, indication for Cesarean, diabetes mellitus.
Statistical Analysis
Data was entered an Epi-Info version 7 and analysed using State version 11. A descriptive analysis for mean, median and proportions of the study population was conducted. The proportion of those with wound sepsis was estimated to determine the prevalence of wound sepsis in the study. Pearson chi-square χ², logistic regression analyses were applied to determine associations. Odds ratios were used to determine the strength and direction of association. A p-value of less than 0.05 was considered significant.
Ethical Considerations
Institutional consent was sought from the department of Obstetrics and Gynecology and the Faculty Research Ethical Committee at Mbarara University of Science and Technology.
Results
The overall mean age for the study participants was 24.6 years. Most of the septic cases were in the group of 20-34 years (44) contributing to about 81.7% of all the septic cases. Rural residents contributed most of cases (70.4%) compared to their urban counterparts. The overall HIV prevalence in the study population was 11.7%. Majority of mothers who did not receive preoperative antibiotics had wound sepsis (88.9%) (Table 1). There were four types of micro-organisms isolated in the septic wounds following Cesarean during this study (staph aureus, klebsiella, E. coli and proteus). Staphylococcus aureus was the most prevalent accounting for 48.2% of the isolated microorganisms (Table 2). Amoxicillin, ampicillin, septrin and chloramphenicol did not have therapeutic antibiotic activity on Staphylococcus aureus (Table 3).
Table 1: Participants’ socio-demographic, obstetric and medical characteristics
|
Variable |
Presence of infection, n |
Absence of infection, n |
|
Age |
||
|
<20 |
08 |
50 |
|
20-34 |
44 |
227 |
|
35-49 |
02 |
18 |
|
HIV Positive |
04 |
37 |
|
HIV Negative |
50 |
258 |
|
Urban |
16 |
75 |
|
Rural |
38 |
220 |
|
Married |
23 |
103 |
|
Separated |
02 |
02 |
|
Single |
25 |
190 |
|
Primipara |
22 |
97 |
|
Multiparous |
25 |
25 |
|
Grand multipara |
7 |
34 |
|
No education |
6 |
28 |
|
Primary |
26 |
152 |
|
Secondary |
17 |
93 |
|
Post-secondary |
05 |
22 |
|
More than 4 ANC attendance |
37 |
210 |
|
Less than 4 ANC attendance |
17 |
85 |
|
Referred |
28 |
134 |
|
Not referred |
26 |
161 |
|
No. of vaginal exams before Cesarean |
||
|
<4 times |
23 |
236 |
|
≤4 times |
31 |
59 |
|
Pre-operative antibiotics given |
48 |
243 |
|
Pre-operative antibiotics not given |
6 |
52 |
|
History of PROM |
5 |
8 |
|
No history of PROM |
49 |
287 |
|
Elective Cesarean |
3 |
11 |
|
Emergency Cesarean |
51 |
284 |
|
History of DM |
4 |
2 |
|
No history of DM |
50 |
293 |
|
BMI: Underweight |
0 |
1 |
|
Normal |
08 |
88 |
|
Overweight |
42 |
115 |
|
Obesity |
04 |
91 |
BMI-Body Mass Index; UTI-urinary tract infection; DM-diabetes
mellitus; C/S-Cesarean section; PROM- Prolonged rupture of membranes; ANC-antenatal care; HIV-human immuno-deficiency virus.
Table 2: Microorganisms isolated from the infected wounds
|
Organism isolated |
Frequency n (%) |
|
Staph aureus |
27 (48.2) |
|
Klebsiella |
15 (26.8) |
|
Escherichia coli |
4 (7.1) |
|
Proteus species |
10 (17.9) |
|
Total |
56 (100) |
Table 3: Antimicrobial resistance patterns for (Staphylococcus aureus)
|
Drug tested |
% Resistance |
|
Ampicillin |
100 |
|
Amoxicillin |
100 |
|
Gentamycin |
0.0 |
|
Penicillin G |
77.8 |
|
Chloramphenicol |
100 |
|
Erythromycin |
66.7 |
|
Septrin |
100 |
|
Augmentin |
14.8 |
|
Oxacillin |
77.8 |
|
Ceftriaxone |
7.4 |
|
Ceftazidime |
11.1 |
|
Tetracycline |
85.2 |
|
Cloxacillin |
51.9 |
There was marked resistance of the three isolated gram-negative micro-organisms against the following antibiotics: Chloramphenicol, septrin, tetracycline. Ciprofloxacin is still very potent towards the three micro-organisms (Table 4). After adjusting for cofounders, the factors associated with wound sepsis were the following: severe anemia (aOR 11.64, 95% CI 5.2-26.1, P=<0.001), more than four vaginal exams before Cesarean (aOR 7.39, 95% CI 3.3-16.5, P=<0.001), ruptured membranes for over 24 hours (aOR 9.89, 95% CI 2.1- 47.6, P=<0.001), diabetes mellitus (aOR 8.70, 95% CI 3.9-19.3, P=<0.001), being referred to Mbarara Hospital (aOR 3.98, 95% CI 1.7-9.4, P=<0.001), prolonged labour (>18 hours) (aOR 6.06, 95% CI 2.6-14.3, P=<0.001), antenatal care (ANC) attendance less than 4 times (aOR 2.11, 95% CI 1.1-4.2, P=0.03), abnormal body mass index (aOR 2.45, 95% CI 1.1-5.6, P=0.03). Receiving pre-operative Cesarean antibiotics was found to be protective against wound sepsis (aOR 0.38, 95% CI 0.17- 0.74, P=0.01) (Table 5 and 6).
Table 4: Antimicrobial resistance patterns for gram negative organisms
|
Drug |
% Resistance for Klebsiella |
% Resistance for E. coli |
% Resistance for proteus species |
|
Gentamicin |
26.7 |
0.0 |
10.0 |
|
Chloramphenicol |
86.7 |
100 |
100 |
|
Septrin |
93.3 |
100 |
90.0 |
|
Augmentin |
13.7 |
0.0 |
0.0 |
|
Ceftriaxone |
6.7 |
0.0 |
20.0 |
|
Ceftazidime |
20.0 |
0.0 |
20.0 |
|
Tetracycline |
100 |
100 |
100 |
|
Ciprofloxacillin |
0.0 |
7.4 |
0.0 |
|
Nalidixic acid |
13.7 |
25.0 |
30.0 |
Table 5: Bivariate analysis of socio-demographic, obstetric and medical profiles of participants
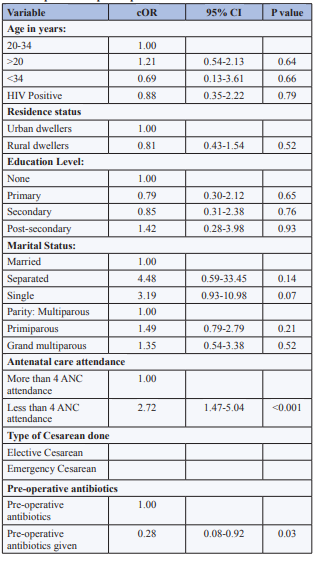
ANC-Antenatal Care; Hb-Hemoglobin; cOR-crude odds ratio; CI-confidence interval; C/S-Cesarean section.
Table 6: Factors associated with post Cesarean wound sepsis (Multivariate analysis)
|
Variable |
aOR |
95% CI |
P-value |
|
Abnormal body mass index |
2.45 |
1.08-5.57 |
0.03 |
|
Diabetes mellitus |
8.70 |
3.93-19.25 |
<0.001 |
|
ANC attendance less than 4 times |
2.11 |
1.05-4.20 |
0.03 |
|
Above four vaginal exams before Cesarean |
7.39 |
3.32-16.52 |
<0.001 |
|
Pre-operative antibiotics use |
0.38 |
0.17- 0.74 |
0.01 |
|
Referred to MRRH |
3.98 |
1.69-9.38 |
<0.001 |
|
Severe Anemia (Hb below 7g/dl) |
11.64 |
5.19-26.08 |
<0.001 |
|
Prolonged labour (>18 hours) |
6.06 |
2.58-14.27 |
<0.001 |
|
Prolonged rupture of membranes (>24 hours) |
9.89 |
2.05- 47.61 |
<0.001 |
ANC-Antenatal Care; MRRH-Mbarara Regional Referral Hospital; Hb-Hemoglobin; aOR-adjusted odds ratio; CI-confidence interval; C/S-Cesarean section.
Discussion
Prevalence
The prevalence of Post-Cesarean wound sepsis in our study was 15.5%. Other studies have found prevalence in the ranges of 2.5-33.3% [3,4,16,17]. The prevalence found in our study lies within the ranges like studies done elsewhere in sub-Saharan Africa because of similarities in population characteristics. The differences in the proportion figures arises from the differences in the study designs. Whereas our study was a cross-sectional study, some other studies such as the one by Koigi and colleagues were longitudinal studies that determined incidence of wound sepsis [3].
Bacterial Isolates and Microbial Sensitivity Pattern
The commonest micro-organisms isolated in our study were Staphylococcus aureus, Klebsiella pneumoniae, Escherichia coli and proteus species. Other studies done in sub-Saharan Africa also isolated similar micro-organisms such as S. aureus, E. coli, Klebsiella pneumoniae, coagulase negative staphylococcus. S. aureus has been isolated as the most prevalent micro-organism [2,15,18,19]. In our study, there is high sensitivity to cephalosporins and quinolones and wide spread resistance to penicillin such as ampicillin. This is comparable to other study findings [18]. This may be attributed to the irrational use of commonly available antibiotics within the low resource settings. The populations studied are similar in their characteristics, hence the near similarities in the micro-organisms isolated and the antimicrobial susceptibility patterns.
Risk Factors
The risk factors found in our study were severe anemia, more than four vaginal exams before Cesarean, and ruptured membranes for over 24 hours, diabetes mellitus, being referred to Mbarara Hospital, prolonged labour, antenatal care (ANC) attendance less than 4 times, and abnormal body mass index. Some studies have also found the following as risk factors wound sepsis: abnormal body mass index (BMI), hypertensive disorders, premature rupture of membranes, diabetes mellitus, emergency Cesarean delivery [2,4,20,21]. Mothers with anemia were more likely to have wound sepsis because a higher concentration of Hemoglobin helps in the oxygen carrying capacity of blood and thus severe anemia therefore hinders wound healing and immunity because of poor oxygen carrying capacity. Prolonged rupture of membranes predisposes to wound infection because when there is prolonged rupture of membranes, there is a chance of ascending infection and chorioamnionitis and wound infection may supervene following Cesarean.
Mothers with diabetes mellitus are more prone to development of wound compared to their normal counterparts because hyperglycemia impairs neutrophil function there by reducing the immunity of the mothers. The reduced immunity will predispose mothers to secondary infections. Also due to peripheral arterial disease caused by diabetes mellitus, reduced blood supply to the wound will impair healing and immunity there by predisposing the wound infections [22]. Mothers who were in labour for over eighteen hours were more likely to develop wound sepsis due to factors such as early rupture of membranes and multiple vaginal examinations which could lead to ascending infections leading to chorioamnionitis which in turn leads to infection of the post Cesarean wounds [2]. The mothers who had more than four vaginal examinations in labour were more likely to develop wound sepsis due to enterococci contamination from the anorectal region leading to ascending infection of liquor [23].
Pre-operative antibiotics use for Cesarean was found to be protective against development of post Cesarean wound sepsis. Administration of pre-operative antibiotics within 30 to 60 minutes of skin incision reduces risk of postoperative infection by almost 70% and maximizes concentrations at the surgical site [5,11-14].
Conclusions
The prevalence of wound sepsis at MRRH is high and most of the bacterial isolates were susceptible to 3rd generation cephalosporin and quinolones but resistant to most penicillins. Severe anaemia, prolonged rupture of membranes, diabetes mellitus, multiple vaginal examinations (over four times), prolonged labour (over 18 hours), patients referred from peripheral health facilities, preoperative and postoperative antibiotic use, abnormal BMI and less than four times antenatal attendance were factors associated with development of post Cesarean wound sepsis.
What is already known on this topic?
1. Administration of pre-operative antibiotics within 30 to 60 minutes of skin incision reduces risk of postoperative infection by almost 70%.
2. Women giving birth by Cesarean section have a 5- to 20-fold greater risk of postpartum sepsis than women giving birth vaginally.
What this study adds
1. Prolonged rupture of membranes predisposes to wound infection.
2. The mothers who had more than four vaginal examinations in labour were more likely to develop wound sepsis.
Competing Interests
The authors declare no competing interests.
Authors Contributions
Joseph Isanga conceptualized the research idea, collected and analyzed data, drafted the manuscript and participated in critical revisions; Joseph Ngonzi conceptualized the research idea, analyzed data, drafted the manuscript and participated in critical revisions; Kayondo Musa participated in critical revisions; Julius Mugisha participated in critical revisions; Ronald Mayanja participated in data analysis and critical manuscript revisions; Leevan Tibaijuka participated in critical manuscript revisions and Emmanuel Byaruhanga participated in data analysis and critical manuscript revisions. All the authors have read and agreed to the final manuscript.
Acknowledgments
We acknowledge the department of obstetrics and Gynecology at Mbarara University and the study participants for their participation in the study and allowing us to carry out the study. The Hospital director’s office at Mbarara Hospital was also very supportive
References
- Ikeako L, Nwajiaku L, Ezegwui H (2009) Caesarean section in a secondary health hospital in Awka, Nigeria. Nigerian Medical Journal 50: 64-67.
- Jido T, Garba I (2012) Surgical-site infection following Cesarean section in Kano, Nigeria. Annals of medical and health sciences research 2: 33-36.
- Koigi-Kamau R, Kabare L, Wanyoike-Gichuhi J (2005) Incidence of wound infection after caesarean delivery in a district hospital in central Kenya. East African medical journal 82: 357-361.
- Amenu D, Belachew T, Araya F (2011) Surgical site infection rate and risk factors among obstetric cases of Jimma University Specialized Hospital, Southwest Ethiopia. Ethiopian journal of health sciences 21: 91-100.
- Smaill FM, Grivell RM (2014) Antibiotic prophylaxis versus no prophylaxis for preventing infection after Cesarean section. Cochrane Database Syst Rev 10: CD007482.
- Van Dillen J, Zwart J, Schutte J, Van Roosmalen J (2010) Maternal sepsis: epidemiology, etiology and outcome. Curr Opin Infect Dis 23: 249-254.
- Lapinsky SE (2013) Obstetric infections. Critical care cliniCesarean 29: 509-520.
- Ngonzi J, Tornes YF, Mukasa PK, Salongo W, Kabakyenga J, et al. (2016) Puerperal sepsis, the leading cause of maternal deaths at a Tertiary University Teaching Hospital in Uganda. BMC pregnancy and childbirth 16: 207.
- Mpogoro FJ, Mshana SE, Mirambo MM, Kidenya BR, Gumodoka B, et al. (2014) Incidence and predictors of surgical site infections following caesarean sections at Bugando Medical Centre, Mwanza, Tanzania. Antimicrobial resistance and infection control 3: 25.
- Temming LA, Raghuraman N, Carter EB, Stout MJ, Rampersad RM, et al. (2017) Impact of evidence-based interventions on wound complications after Cesarean delivery. American Journal of ObstetriCesarean & Gynecology 217: 449.e1-449.e9.
- Dlamini LD, Sekikubo M, Tumukunde J, Kojjo C, Ocen D, et al. (2015) Antibiotic prophylaxis for caesarean section at a Ugandan hospital: a randomised clinical trial evaluating the effect of administration time on the incidence of postoperative infections. BMC pregnancy and childbirth 15: 91.
- Tita AT, Rouse DJ, Blackwell S, Saade GR, Spong CY, et al. (2009) Evolving concepts in antibiotic prophylaxis for Cesarean delivery: A systematic review. ObstetriCesarean and gynecology 113: 675-682.
- Alfirevic Z, Gyte GM, Dou L (2010) Different classes of antibiotiCesarean given to women routinely for preventing infection at caesarean section. The Cochrane Library.
- Shetty J, Rajshekhar S, Kamath A (2008) Short term antibiotic prophylaxis for emergency Cesarean delivery: Is there a difference? The internet journal of gynecology and obstetriCesarean 11: 1-7.
- Bebell LM, Ngonzi J, Bazira J, Fajardo Y, Boatin AA, et al. (2017) Antimicrobial-resistant infections among postpartum women at a Ugandan referral hospital. PLoS One 12: e0175456.
- Owen J, Andrews WW (1994) Wound complications after Cesarean sections. Clinical obstetriCesarean and gynecology 37: 842-855.
- Awad SS (2012) Adherence to surgical care improvement project measures and post-operative surgical site infections. Surgical infections 13: 234-237.
- Bitew Kifilie A, Dagnew M, Tegenie B, Yeshitela B, Howe R, et al. (2018) Bacterial Profile, Antibacterial Resistance Pattern, and Associated Factors from Women Attending Postnatal Health Service at University of Gondar Teaching Hospital, Northwest Ethiopia. Int J Microbiol 3165391.
- Henman K, Gordon CL, Gardiner T, Thorn J, Spain B, et al. (2012) Surgical site infections following caesarean section at Royal Darwin Hospital, Northern Territory. Healthcare infection 17: 47-51.
- Schneid-Kofman N, Sheiner E, Levy A, Holcberg G (2005) Risk factors for wound infection following Cesarean deliveries. International Journal of Gynecology & ObstetriCesarean 90: 10-15.
- Wloch C, Wilson J, Lamagni T, Harrington P, Charlett A, et al. (2012) Risk factors for surgical site infection following caesarean section in England: results from a multicenter cohort study. BJOG: An International Journal of ObstetriCesarean & Gynecology 119: 1324-1333.
- Takoudes TC, Weitzen S, Slocum J, Malee M (2004) Risk of Cesarean wound complications in diabetic gestations. American Journal of ObstetriCesarean & Gynecology 191: 958-963.
- Ezechi OC, Edet A, Akinlade H, Gab-Okafor CV, Herbertson E (2009) Incidence and risk factors for caesarean wound infection in Lagos Nigeria. BMC research notes 2: 186.