

Research Article - (2026) Volume 9, Issue 2
The Knox (NOx) Monograph
Received Date: Mar 27, 2026 / Accepted Date: Apr 17, 2026 / Published Date: Apr 28, 2026
Copyright: ©2026 Bruce H. Knox. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Knox, B. H. (2026). The Knox (NOx) Monograph. Adv Neur Sci, 9(2), 01-15.
Abstract
This monograph brings together a sequence of closely related papers and conceptual models developed in response to a persistent problem in autonomic medicine: the absence of a coherent longitudinal framework capable of integrating symptoms, risk, and outcomes across time. Although individual features of dysautonomia are well described, patients and clinicians alike continue to struggle with questions of trajectory, prognostic uncertainty, and interpretive meaning [1-3]. The formal prose is accompanied by a selection of music that communicates the story behind the woods. This can be listened to while the monarchy chapters are read by clicking on the link below and then clicking the bottom right-hand corner of each page to turn the page. The selection of songs will play automatically as you read.
Monograph Text and Background Songs that live out the words
The work presented here does not attempt to eliminate uncertainty. Instead, it seeks to locate uncertainty within a structured system that recognises initiation, stabilisation, divergence, recovery, and progression as natural phases of autonomic illness. The emphasis is therefore on integration rather than reduction, and on clarity rather than premature certainty [2,3]. This work also arises from a practical and interpretive tension encountered repeatedly in clinical and lived experience: the difficulty of holding together partial knowledge without collapsing into premature explanation. Patients frequently inhabit extended periods of uncertainty in which neither recovery nor progression can be confidently asserted. The present monograph therefore seeks not only to model disease, but to model how disease is understood over time. In doing so, it advances a form of structured uncertainty capable of supporting both scientific reasoning and human interpretation.
General Introduction
Autonomic dysfunction occupies a paradoxical position in contemporary medicine. It is common in symptom burden but rare in coherent explanatory structure. Patients frequently present with multisystem complaints that resist stable classification, while clinicians encounter uncertainty not due to insufficient expertise, but due to the absence of models capable of addressing longitudinal, system level disease processes [1,2]. The Knox (NOx) Monograph responds to this deficit by reframing dysautonomia not as a static diagnostic category, but as a trajectory. Autonomic illness is approached here as a process that begins, adapts, stabilises, and may ultimately resolve or progress over time. This shift—from classification to trajectory—forms the organising logic of the work [2,3]. Three empirical observations motivate the framework. First, autonomic dysfunction commonly precedes recognised neurological or systemic disease by many years [4-6]. Second, similar constellations of symptoms may conceal markedly different biological futures [4,5]. Third, uncertainty itself carries significant clinical and psychological consequences, shaping both patient experience and medical decision making [1,3]. Accordingly, this monograph asks a central structural question: how does autonomic vulnerability unfold across time? The response offered is neither purely diagnostic nor purely predictive. Rather, the NOx framework integrates physiology, risk modelling, and narrative meaning to describe not only what a patient has, but where they may be heading [2,3]. A further implication of this reframing is methodological. If autonomic dysfunction is inherently longitudinal, then any attempt to understand it through cross-sectional observation alone will necessarily produce distortion. What appears inconsistent at a single time point may, when viewed across time, reveal patterned progression or recovery. The NOx framework therefore does not reject existing diagnostic categories, but situates them within a broader temporal architecture in which their meaning becomes conditional rather than absolute.
Methodological Note
This work is neither a conventional empirical report nor a systematic review. It occupies a deliberately hybrid methodological position combining longitudinal synthesis of peer reviewed clinical research, formal predictive reasoning drawn from survival analysis, conceptual model building informed by clinical observation, and narrative integration grounded in the medical humanities [1-3]. Source material is drawn primarily from autonomic neurology, movement disorder research, and clinical prediction modelling. Evidence has been selected for relevance to trajectory, hazard accumulation, and pathway divergence rather than exhaustive coverage. No new patient level data are introduced [1,2]. The contribution of this monograph lies in integration. Existing empirical findings are reorganised into a coherent longitudinal architecture capable of accommodating uncertainty without collapsing into vagueness. Mathematical concepts are employed interpretively rather than computationally, with emphasis on hazard, interaction, and time dependence [1-3]. The framework is intended to be generative rather than prescriptive: a lens through which autonomic illness may be interpreted without imposing premature conclusions [2,3].
This hybrid methodology reflects an intentional departure from disciplinary isolation. Autonomic medicine, prediction science, and the medical humanities are here treated not as separate domains, but as complementary lenses through which complex systems may be understood. The resulting synthesis prioritises coherence over completeness, recognising that in conditions characterised by uncertainty, explanatory integration may be of greater value than exhaustive detail.
Chapter 1
Phenoconversion from Pure Autonomic Failure
• Abstract
Pure autonomic failure occupies an unstable position within the spectrum of autonomic disorders. This chapter examines phenoconversion risk using contemporary longitudinal evidence and reframes pure autonomic failure as a prodromal state rather than a terminal diagnosis [4-6].
• Main
Text Pure autonomic failure (PAF) is defined by neurogenic orthostatic hypotension and widespread autonomic dysfunction in the absence of overt central neurological signs. Historically regarded as a rare peripheral disorder, PAF is now recognised as a prodromal manifestation of α synucleinopathy in a substantial subset of patients [4,7]. Prospective cohort studies demonstrate that approximately one quarter to one third of individuals diagnosed with PAF phenoconvert to Parkinson’s disease, dementia with Lewy bodies, or multiple system atrophy over follow up intervals extending to a decade. Annualised phenoconversion risk has been estimated at approximately 12%, underscoring the cumulative and time dependent nature of risk [4,5]. Importantly, phenoconversion is patterned rather than stochastic. Early urinary or sexual dysfunction, REM sleep behaviour disorder, subtle emerging motor signs, dysphagia, and speech disturbance are each associated with elevated hazard ratios for downstream neurodegeneration.4 5 These findings support a multiplicative rather than additive interpretation of risk, consistent with the original NOx model architecture [1,2].
Neuropathological evidence further reinforces this interpretation. Initial α synuclein deposition in PAF is predominantly peripheral, but subsequent divergence toward Lewy body disease or multiple system atrophy reflects distinct patterns of central and sympathetic involvement [7]. PAF therefore functions as a biological junction point rather than a fixed diagnostic endpoint [6,7]. From a longitudinal perspective, the significance of PAF lies not only in its association with future disease, but in its capacity to reveal early system instability before categorical diagnosis becomes possible. The temporal gap between autonomic onset and neurological consolidation represents a critical observational window in which trajectory remains partially modifiable and incompletely determined. This interval also raises important interpretive challenges. Because phenoconversion unfolds gradually, the distinction between stable disease and early progression is often blurred. Subclinical features may accumulate beneath the threshold of formal diagnosis, creating a phase in which biological direction is shifting but not yet clinically codified. Within the NOx framework, this phase is not treated as diagnostic ambiguity, but as trajectory emergence. Importantly, not all individuals with PAF will phenoconvert. A proportion remain stable over extended periods, suggesting the presence of modifying factors that constrain progression. These may include differences in autonomic reserve, patterns of α-synuclein distribution, or systemic resilience. The existence of such divergence reinforces the necessity of probabilistic rather than deterministic interpretation.

Chapter 2
Phenoconversion from Multifactorial Secondary Dysautonomia
• Abstract
Secondary dysautonomia represents a heterogeneous initiation phase of autonomic disruption. This chapter examines resilience, recovery, and progression following identifiable physiological insult and extends the NOx framework upstream to capture early vulnerability and divergence [1,2,6].
• Main
Text Secondary dysautonomia arises following identifiable systemic stressors, including viral illness, immune activation, cardiovascular compromise, trauma, or surgical intervention. Unlike primary autonomic failure syndromes, these conditions are characterised by marked biological plasticity, with outcomes ranging from full recovery to chronic persistence or downstream progression [6].
From a mechanistic perspective, secondary dysautonomia reflects disruption of autonomic regulation rather than intrinsic neurodegenerative failure. Proposed mechanisms include immune mediated autonomic injury, inflammatory or endothelial dysfunction, altered baroreflex function, and transient disturbance of central autonomic network integration [2,6]. While these processes may be reversible, their persistence creates conditions under which vulnerability may accumulate. Post viral dysautonomia provides a contemporary and illustrative example of this initiation phase. Following SARS CoV 2 infection, a significant proportion of individuals develop sustained autonomic symptoms, including postural orthostatic tachycardia syndrome, orthostatic hypotension, and mixed cardiovascular autonomic instability. These syndromes demonstrate fluctuating severity over time and substantial interindividual variability, underscoring the inadequacy of static diagnostic categorization [6].
Crucially, longitudinal observation indicates that recovery remains biologically plausible in this group. When the initiating insult resolves and compensatory autonomic rebalancing occurs, symptom trajectories may improve gradually over months or years. Conversely, failure of stabilisation permits persistence of dysautonomia, allowing downstream risk factors to interact and amplify over time [1,2]. This initiation phase therefore establishes the conceptual necessity of Stage 0 within the Knox Master Framework. Prediction does not begin at symptom persistence, nor at formal diagnosis, but at disruption itself. Secondary dysautonomia serves as the biological substrate upon which later divergence—toward recovery or progression—emerges [2,3]. The variability observed in secondary dysautonomia also highlights the role of threshold phenomena. Initial disruption does not inevitably lead to chronic dysfunction; rather, outcomes depend on whether compensatory mechanisms are sufficient to restore equilibrium. When these mechanisms succeed, recovery trajectories emerge. When they fail, persistent dysregulation creates a platform upon which additional risk factors may accumulate. This distinction introduces an important conceptual refinement within the NOx framework: vulnerability is not a fixed attribute but a dynamic state shaped by interaction between insult, response, and time. Early intervention, whether physiological, behavioural, or supportive, may therefore influence trajectory not by eliminating the initiating event, but by enhancing stabilisation processes. Furthermore, secondary dysautonomia challenges traditional distinctions between “functional” and “organic” illness. The fluctuating and reversible nature of many cases reflects genuine biological plasticity rather than the absence of pathology. Within a longitudinal model, such plasticity becomes intelligible as part of system adaptation rather than diagnostic uncertainty.


Chapter 3
The Knox Master Framework
Abstract
This chapter integrates upstream initiation and downstream phenoconversion processes into a single longitudinal system. The Knox Master Framework reconceptualises autonomic dysfunction as a dynamic trajectory unfolding across time rather than a static diagnostic state [1-3].
Main Text
Autonomic dysfunction is frequently detected long before formal neurological diagnosis and may precede recognised neurodegenerative disease by many years. Longitudinal studies of autonomic disorders demonstrate that symptoms often emerge early, fluctuate over extended periods, and only later consolidate into recognisable syndromic patterns [4-7]. Static classification systems therefore obscure clinically meaningful information about direction, velocity, and hazard accumulation [1,2]. The Knox Master Framework addresses this limitation by organising autonomic illness into a longitudinal structure rather than a categorical taxonomy. Within this model, dysautonomia is understood as a time dependent process shaped by interacting physiological stresses, adaptive responses, and cumulative vulnerability [1,3].
The framework delineates three sequential but permeable stages. Stage 0 — Initiation refers to the onset of autonomic disruption following a definable physiological insult, including post viral illness, immune activation, cardiovascular compromise, trauma, or surgical stress. At this stage, dysfunction reflects regulatory disturbance rather than intrinsic neurodegeneration, and biological outcomes remain indeterminate [6].
Stage 1 — Stabilisation represents a critical adaptive phase during which autonomic systems may either recover equilibrium or fail to compensate. Recovery is characterised by gradual symptom attenuation and restoration of autonomic balance. Persistence, by contrast, reflects failure of stabilisation and creates conditions under which downstream risk factors may interact and amplify [1,2].
Stage 2 — Progression denotes the accumulation of phenoconversion risk. In this phase, persistent autonomic dysfunction interacts with multisystem involvement, temporal duration, and emerging neurological features, increasing the probability of transition toward defined neurodegenerative syndromes such as Parkinson's disease, dementia with Lewy bodies, or multiple system atrophy [4,5,7].
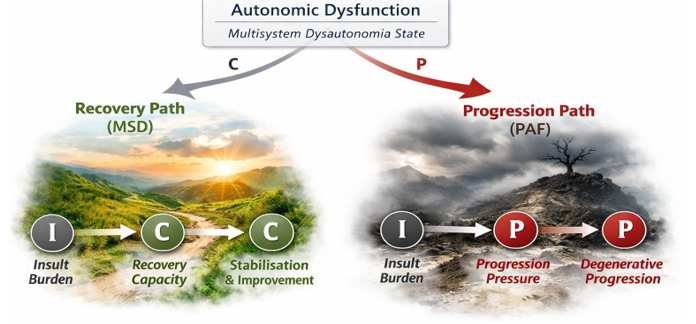
An additional dimension of the Master Framework is the concept of trajectory velocity. Not all patients move through stages at the same rate. Some experience rapid stabilisation or progression, while others remain within intermediate states for prolonged periods. Velocity, therefore, becomes an informative variable, reflecting underlying biological dynamics and influencing predictive interpretation. Central to the Master Framework is the Dual Pathway Hypothesis. From a shared multisystem presentation at Stage 1, two biologically plausible futures emerge. Pathway A (Recovery) involves resolution of the initiating insult, restoration of autonomic balance, and gradual symptom improvement. Pathway B (Progression) involves persistence of dysfunction, expansion across regulatory systems, and increased likelihood of phenoconversion [1-3]. Critically, identical clinical presentations may occupy different positions within this structure. Apparent diagnostic ambiguity is therefore reframed as biological indeterminacy rather than clinical failure. The framework shifts uncertainty from a problem to be eliminated into a signal to be interpreted longitudinally [2,3].
By integrating initiation, stabilisation, and progression into a single system, the Knox Master Framework provides a conceptual map that accommodates recovery and decline without contradiction. It aligns predictive reasoning with biological complexity and reorients clinical interpretation toward trajectory rather than label [1-2]. The framework also accommodates partial reversibility. Movement between stages is not strictly unidirectional; patients may demonstrate periods of improvement followed by relapse, or stabilisation followed by renewed progression. These oscillations do not invalidate the model; rather, they reflect the adaptive and non-linear nature of autonomic regulation. By incorporating both direction and reversibility, the Master Framework captures a key feature of autonomic illness: it is not simply a path toward decline, but a dynamic process in which multiple futures remain possible until the trajectory becomes progressively constrained.


Figure 1: Longitudinal Trajectory Structure (conceptual)

Chapter 4
Mathematical Architecture of the NOx Model
Abstract
This chapter formalises the mathematical reasoning underlying the NOx model. Drawing on principles from survival analysis and clinical prediction modelling, the model frames phenoconversion as a time dependent, probabilistic process shaped by interacting risk factors rather than a deterministic outcome [1-3].
Main Text
The NOx model is grounded conceptually in hazard-based survival analysis, a class of methods designed to model time-to-event phenomena when outcomes may or may not occur within an observed interval. Such methods are particularly well suited to autonomic disorders, in which phenoconversion represents a conditional and censored event rather than a fixed endpoint [1-3]. Within this framework, phenoconversion is not treated as a binary diagnostic transition but as a probability distribution that evolves. The fundamental quantity of interest is hazard: the instantaneous risk of transition at a given time point, conditional on having remained event free up to that point [1]. This allows risk to be conceptualised dynamically rather than categorically. The mathematical logic of the NOx model aligns most closely with the structure of Cox proportional hazards modelling. In this approach, baseline risk is modified by the presence and interaction of covariates without requiring specification of an underlying hazard function [1-3]. This structure permits integration of heterogeneous clinical variables while preserving interpretability. Crucially, risk within the NOx architecture is multiplicative rather than additive. Individual contributors—such as severity of autonomic dysfunction, multisystem involvement, temporal persistence, and emerging neurological features—do not simply accumulate linearly. Instead, their interaction amplifies hazard disproportionately, reflecting biological complexity observed in longitudinal autonomic disorders [2,3].
This multiplicative structure also allows for interaction effects that are not immediately apparent at the clinical level. For example, modest impairments across several systems may combine to produce a level of risk disproportionate to any single deficit. Such interactions mirror biological systems in which network behaviour emerges from interdependence rather than isolated function. Time plays a central role in this architecture. Risk is not static at diagnosis, nor does the initial presentation fix it. Persistence of dysfunction across months or years modifies subsequent hazard, such that duration itself becomes a biologically meaningful variable. This temporal dependence distinguishes the NOx model from cross sectional diagnostic schemas [1,2]. The model also resists reduction to single predictive thresholds. Rather than defining cut points beyond which progression is assumed, NOx reflects evolving risk across a continuum. This approach reflects best practice in clinical prediction modelling, where calibration, discrimination, and uncertainty must be preserved rather than collapsed into binary outcomes [2,3]. Uncertainty is thus intrinsic to the model rather than an artefact of measurement error. By design, NOx quantifies uncertainty across time, allowing prediction to coexist with indeterminacy. This is consistent both with the probabilistic nature of survival models and with the biological realities of autonomic disease trajectories [1-3].
Mathematically, the NOx model therefore functions as an interpretive architecture rather than a computational algorithm. It provides structure for understanding how risk evolves, interacts, and diverges, without enforcing premature determinism. Prediction is reframed as informed estimation across time rather than categorical judgement [2,3]. Importantly, the NOx model does not seek to replace formal statistical modelling but to provide an interpretive scaffold through which such models may be understood. In this sense, it operates at the interface between quantitative reasoning and clinical judgement, enabling practitioners to conceptualise risk even in the absence of precise numerical estimation. This distinction preserves the integrity of prediction science while extending its accessibility, allowing hazard-based reasoning to inform interpretation without requiring full computational implementation in every clinical context.



Chapter 5
Plain Language Interpretation
Abstract
This chapter translates the NOx framework into accessible explanatory language without sacrificing conceptual or scientific integrity. Reframing autonomic illness as a trajectory rather than a diagnosis supports shared understanding among clinicians, patients, and interdisciplinary audiences [1-3].
Main Text
Despite advances in autonomic medicine, many patients experience dysautonomia as an unintelligible and destabilising condition. Symptoms are often invisible, fluctuating, and poorly aligned with conventional diagnostic narratives. As a result, patients may struggle not only with illness itself but also with uncertainty about explanations, prognosis, and meaning [1,6]. The NOx framework addresses this problem by shifting emphasis away from labels and toward the direction of travel. In plain terms, autonomic illness is not defined solely by the symptoms present, but by how the system behaves over time. Some nervous systems are gradually stabilising and recovering balance; others are failing to compensate and becoming increasingly dysregulated [1-3]. This distinction helps explain why identical symptom patterns can lead to very different outcomes. Two individuals with similar degrees of orthostatic intolerance, fatigue, or gastrointestinal disturbance may, in fact, be on divergent trajectories—one recovering, the other accumulating risk. Longitudinal interpretation, therefore, carries greater explanatory power than isolated clinical snapshots [2,3]. Time is central to this interpretation. Symptoms that improve gradually suggest adaptive rebalancing, whereas symptoms that persist or expand across systems indicate increasing vulnerability. Duration itself becomes meaningful, not as a diagnostic threshold, but as part of a developing pattern [1,2].
Uncertainty, within this framework, is not treated as failure or ignorance. Instead, it reflects a branch point. At early stages, outcomes remain indeterminate because biological systems retain flexibility. As time passes and interactions accumulate, trajectories become more legible. The NOx framework locates uncertainty within the structure of illness rather than outside it [2,3]. This approach aligns with evidence from clinical prediction modelling, which consistently demonstrates that risk exists along a continuum and cannot be reduced responsibly to binary categories. Identification of trajectory, therefore, supports more honest communication and avoids false reassurance or premature pessimism [1-3]. Importantly, plain language explanation does not simplify biology; it clarifies it. By naming initiation, stabilisation, recovery, and progression as observable phases, the framework allows patients to understand not only what is happening but also why timing and patterns matter. This shared understanding supports engagement, adaptive decision making, and psychological containment in the face of uncertainty [2,6]. In this sense, the NOx model functions not only as a predictive or conceptual tool but as a communicative bridge. It translates complex longitudinal reasoning into language that can be shared across clinical, personal, and interdisciplinary contexts—without abandoning rigour [1-3].
A further benefit of this approach is its capacity to reduce cognitive and emotional burden. When patients are provided only with diagnostic labels, uncertainty is often experienced as the absence of knowledge. By contrast, when illness is explained as a trajectory, uncertainty becomes contextualised within a broader pattern, allowing individuals to situate their experience within a meaningful structure. This reframing also supports more adaptive clinical conversations. Rather than focusing solely on what cannot yet be known, clinicians can discuss observable indicators of direction—improvement, persistence, or expansion—thereby grounding uncertainty in shared observation rather than abstraction. In this way, plain-language interpretation becomes not merely a translation of technical concepts, but an essential component of care.


Chapter 6
Case Based Integration and Synthesis
Abstract
This chapter applies the Knox Master Framework to case derived trajectories in autonomic dysfunction. By integrating longitudinal observation with predictive structure, it demonstrates how heterogeneous outcomes can be interpreted coherently without resorting to rigid classification [1-3].
Main Text
Case based observation has long been central to understanding autonomic disorders. However, in the absence of a longitudinal framework, individual cases are often interpreted retrospectively or in isolation, limiting their explanatory power. When viewed cross sectionally, heterogeneity appears anomalous; when viewed longitudinally, it becomes informative [4-6]. Across autonomic medicine, case series consistently demonstrate profound variability in outcome. Patients presenting with broadly similar symptoms— orthostatic hypotension, cardiovascular instability, gastrointestinal dysmotility, fatigue, or sleep disturbance—may follow markedly different trajectories. Some recover gradually, others stabilise with chronic impairment, and others progress toward defined neurodegenerative syndromes [4,5]. The Knox Master Framework provides a structure within which such divergence can be interpreted. Rather than asking why outcomes differ despite similar presentations, the framework redirects attention to the phases of illness patients occupy. Initiation, stabilisation, and progression are not inferred retrospectively but observed dynamically across time [1,2]. At the level of individual cases, this distinction is critical. A patient whose autonomic symptoms arise following a viral or surgical insult and gradually attenuate over subsequent months occupies a fundamentally different biological position from a patient whose symptoms persist, expand across systems, and accumulate additional neurological features. Both cases may appear similar at a single time point, but their trajectories diverge meaningfully [6].
In phenoconversion research, this pattern is well documented. Longitudinal cohorts of pure autonomic failure reveal that while many individuals remain stable for extended periods, a substantial subset transitions toward Parkinson's disease, dementia with Lewy bodies, or multiple system atrophy. Importantly, this transition is rarely abrupt. Instead, it is preceded by subtle but progressive changes in autonomic, motor, and non motor domains [4,5,7]. By mapping cases onto the Master Framework, clinicians can interpret these changes as signals of pathway commitment rather than diagnostic surprises. Progression is no longer framed as sudden deterioration, but as the cumulative outcome of persistent instability and interacting vulnerabilities [1-3]. Equally important, the framework preserves the legitimacy of recovery. Case based trajectories that demonstrate gradual improvement are not dismissed as benign variants or diagnostic errors; they are recognised as valid expressions of adaptive rebalancing. This acknowledgment is essential for both clinical reasoning and patient communication [2,6]. Synthesis across cases thus reveals a central insight: heterogeneity in autonomic illness does not imply conceptual failure. Rather, it reflects the operation of a dynamic system under stress. The Master Framework renders this variability intelligible by situating each case within a shared longitudinal architecture [1,2].
In this way, case based integration completes the NOx model. Prediction, trajectory, and narrative interpretation converge, allowing individual experiences to be understood as expressions of underlying system dynamics rather than isolated anomalies [3]. Case-based synthesis also reveals the importance of temporal layering. Early features that appear nonspecific or transient may acquire significance only when viewed retrospectively within a longer trajectory. The framework, therefore, encourages prospective attention to subtle change, recognising that small deviations may signal emerging pathway commitment.
Additionally, mapping cases longitudinally enables comparison across individuals without reducing them to uniform categories. Each case retains its specificity while contributing to a broader pattern of system behaviour. This balance between individuality and generalisability is central to the explanatory strength of the NOx model. Ultimately, case integration demonstrates that prediction is not imposed externally on patient experience but arises from careful observation of how that experience unfolds over time.
Conclusion
Autonomic dysfunction challenges conventional medical reasoning because it unfolds across time, crosses physiological boundaries, and resists stable categorisation. Symptoms may precede formal diagnosis by years, fluctuate unpredictably, and diverge toward recovery or progression despite similar initial presentations. Static diagnostic frameworks are therefore poorly suited to capture the lived and biological reality of autonomic illness [1-3]. This monograph has advanced an alternative approach. Rather than treating dysautonomia as a fixed condition, the Knox (NOx) framework conceptualises autonomic illness as a trajectory shaped by initiation, stabilisation, interaction, and time. Within this structure, uncertainty is neither dismissed nor pathologised, but recognised as an intrinsic feature of biological systems under stress [1,2]. By integrating downstream phenoconversion modelling with upstream initiation dynamics, the NOx framework provides a unified longitudinal architecture that accommodates both recovery and progression. Pure autonomic failure is reframed as a junction point rather than a terminal diagnosis. At the same time, secondary dysautonomia is recognised as a biologically indeterminate initiation phase with genuine potential for resolution or escalation [4-7].
The mathematical architecture of the model aligns with contemporary survival analysis and clinical prediction theory, privileging hazard, interaction, and temporal persistence over binary thresholds. Risk is expressed as probabilistic and cumulative, reflecting biological complexity rather than enforcing premature determinism [1-3]. This approach supports more honest clinical reasoning and a more accurate representation of uncertainty. Equally important is the framework's translational dimension. Plain language interpretation demonstrates that conceptual clarity need not require simplification of biology. By reframing prognosis as a direction of travel rather than a categorical outcome, the NOx model supports a shared understanding between clinicians and patients while preserving scientific integrity [2,3,7]. Case based integration completes the picture. When individual trajectories are mapped onto the Master Framework, heterogeneity becomes intelligible. Divergent outcomes are no longer viewed as anomalies but as expressions of system dynamics operating across time. This reframing restores coherence to clinical observation and offers a meaningful structure for interpreting lived experience [3-6].
Taken together, the NOx framework advances a longitudinal understanding of autonomic dysfunction that bridges physiology, prediction science, and narrative meaning. It does not seek to replace diagnosis, but to contextualise it within time dependent processes that govern vulnerability, adaptation, and collapse. In doing so, it shifts the interpretive centre of gravity from static labels to evolving trajectories. Autonomic illness, within this framework, is understood not as a failure of classification, but as a system under stress—capable of repair, compensation, or decline. Time, interaction, and trajectory emerge as the central axes of interpretation, offering a more faithful account of both biology and experience [1-3]. The implications of this work extend beyond autonomic medicine. Any condition characterised by delayed expression, fluctuating symptoms, and uncertain outcomes may benefit from a trajectory-based framework. By foregrounding time, interaction, and probability, the NOx model offers a generalisable approach to understanding complex, evolving systems within medicine.

References
- Cox, D. R. (1972). Regression models and life-tables. Journal of the royal statistical society: Series B (methodological), 34(2), 187-202.
- Steyerberg, E. W. (2019). Study design for prediction modeling. In Clinical prediction models: a practical approach to development, validation, and updating (pp. 37-58). Cham:Springer International Publishing.
- Harrell FE (2015). Regression Modelling Strategies. New York: Springer.
- Coon, E. A., Mandrekar, J. N., Berini, S. E., Benarroch, E. E., Sandroni, P., Low, P. A., & Singer, W. (2020). Predicting phenoconversion in pure autonomic failure. Neurology, 95(7), e889-e897.
- Millar Vernetti, P., Norcliffe-Kaufmann, L., Palma, J. A.,Biaggioni, I., Shibao, C. A., Peltier, A., ... & Kaufmann,H. (2024). Phenoconversion in pure autonomic failure: a multicentre prospective longitudinal cohort study. Brain,147(7), 2440-2448.
- Palma, J. A., Norcliffe-Kaufmann, L., Fuente-Mora, C., Percival, L., Spalink, C. L., & Kaufmann, H. (2017). 154-Disorders of the autonomic nervous system: autonomic dysfunction in pediatric practice. Swaiman’s pediatric neurology. 6th ed. Elsevier, 1173-83.
- Goldstein, D. S., Isonaka, R., Lamotte, G., & Kaufmann,H. (2021). Different phenoconversion pathways in pure autonomic failure with versus without Lewy bodies. Clinical Autonomic Research, 31(6), 677-684.