
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2017) Volume 2, Issue 2
The Effect of Electronic Medical Record Adaptation on Reported Medication Errors in Peripartum Care Areas
2Department of Grants and Research, Maricopa Integrated Health System, Phoenix, AZ, United States
3Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology, St. Joseph’s Hospital and Medical Center, Creighton University School of Medicine, Phoenix, AZ, United States
Received Date: Dec 06, 2017 / Accepted Date: Dec 14, 2017 / Published Date: Dec 22, 2017
Copyright: ©Joel Barkley, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Study Background: The purpose of this before-and-after study was to evaluate if adopting an electronic medical record affected reported medication errors on peripartum obstetrical wards at one hospital.
Methods: A retrospective study of provider reported errors was conducted over a five-year period which included electronic record implementation. The error rate was calculated as the number of errors/patient days. Relative risk was calculated, and Chi-squared analysis was used to compare the proportion of errors before and after electronic record adoption.
Results: The error rate was the same before and after implementation. After implementation, more errors were reported on the labor and delivery ward and fewer from the ante/postpartum ward; however, this was likely only transient.
Conclusion: Implementation of an electronic medical record did not reduce overall medication error reporting rates.
Keywords
Medication Errors, Obstetrics, Electronic Health Records, Patient Safety
Abbreviations
Adverse Drug Events (ADE), Electronic Medical Records (EMR), Computerized Physician Order Entry (CPOE), Clinical Decision Support Software (CDSS).
Introduction
Medication errors are a significant source of patient morbidity and mortality through adverse drug events (ADE) [1]. Since the 1999 Institute of Medicine report highlighting the problem of healthcare related errors, various methods have been proposed to reduce medication errors and improve patient safety. Amongst the suggested methods of error reduction, Electronic Medical Records (EMR) with Computerized Physician Order Entry (CPOE), Clinical Decision Support Software (CDSS) and barcode administration systems have been touted to reduce the frequency and severity of medication errors [2]. There are a variety of implementations of these systems which may be packaged within an EMR or as standalone programs. CPOE refers to systems which replaces paper ordering. They frequently include common dosing and route information for medications to be prescribed and eliminate abbreviations and legibility issues. CDSS is an error checking system that can review the patient’s medications, allergies, and medical conditions to look for contraindications to therapies at the time they are prescribed. Barcode technology may be used to identify patients and label medications. These barcodes are scanned at various points in the medication process (stocking, dispensing, and administration). Although these systems are designed to reduce known issues in the medication process, the reports of their impact on ADE has been mixed [3].
Obstetrical wards face unique problems with regard to medication safety. Novel drugs, off-label use, a mix of healthy and ill patients, fetal exposure and lactation all contribute to the challenges of prescribing. Large multicenter studies of peripartum medication errors have shown a slightly higher overall rate of error on labor wards, when compared to postpartum units, with the majority of errors occurring during the administration phase [4,5]. The medications most often implicated are oxytocin and magnesium sulfate. Another article has reported on an individual hospital’s peripartum ward experience [6]. In contrast, their institution has higher error rates on the postpartum ward. Interestingly, their rate of drug errors on peripartum wards was half that of the rest of the hospital. The previously cited studies have only reported results from prior to 2005. Since that time, the number of hospitals using EMR has more than doubled [7]. The current data also fails to address how the adoption of an EMR affected provider reported hospital medication errors in peripartum areas. The purpose of our study is to determine the effect of EMR implementation on provider reported medication errors in peripartum areas.
Materials and Methods
We conducted this study in a large public urban tertiary medical center which serves a diverse low-income population. A hospital wide medication error reporting system (MIDAS) for the voluntary reporting of adverse hospital events including medication errors was adopted in January of 2009. The medication error tracking system uses the National Coordinating Council for Medication Error Reporting and Prevention index nomenclature for categorizing medication errors (Table 1) [8]. It allows the provider reporting the error to select the phase of the medication process in which the error occurred, the medication(s) involved, the error type, and to input a brief description of the incident.
Table 1: National Coordinating Council for Medication Error Reporting and Prevention index nomenclature
|
Category |
Description |
|
A |
Events that have the potential to cause error |
|
B |
Error did not reach the patient |
|
C |
Error reached patient, but did not cause harm |
|
D |
Error resulted in increased monitoring |
|
E |
Error caused temporary harm or need for intervention |
|
F |
Error resulted in admission or increased length of stay |
|
G |
Error resulted in permanent harm |
|
H |
Error resulted in near-death event |
|
I |
Error resulted in death |
From 2009 to 2012, we used a paper chart with an electronic medication dispensing system. Medication orders were hand written by providers and transmitted to the pharmacy by fax. The pharmacy staff reviewed the orders for accuracy and appropriateness and transcribed them into a computer based system which printed a dispensing schedule that was kept in the chart to be used by the nursing staff. Additions, deletions or modification of orders were hand written onto the chart schedule. Commonly used medications were kept in computerized storage systems on the ward to be used as needed. Medications not stocked were dispensed from pharmacy in individual bags labeled with the patient’s name and order details.
In March of 2012, a hospital wide electronic medical record system (EMR) replaced paper charting (Epic Inpatient Electronic Medical Record). This change modified the medication ordering, dispensing and administrating process, but did not change the policies, procedures and system used to report and track medication errors. Medication orders were entered by the prescribing provider through an integrated Computer Physician Order Entry system (CPOE), available to the pharmacy staff for review. As before, pharmacy staff reviewed the orders for accuracy and appropriateness, but CPOE eliminated the need to fax and transcribe orders. The system also included Clinical Decision Support Software (CDSS) that notifies the ordering provider of potentially harmful drug interactions, allergic reactions and provides default dosage suggestions. The EMR introduced a medication administration system that included reminder prompts when medications were due and a barcode system for tracking dispensing and administration of medications. Commonly used medications were still stocked in ward storage units with the addition of barcodes to confirm accuracy of stocking bins. Medications dispensed by the pharmacy were still printed on labels, but the new labels contained a barcode that could be scanned against manufacturer barcodes to check for medication selection accuracy. The nurse could now scan the patient wristband barcode as well as medication barcode(s) at the time of administration. This required additional step in the administration process would notify the nurse of new information such as if the medication were not yet due to be given or had been canceled.
Our protocol was deemed exempt from review and approved by the hospital institutional review board. We extracted data about medication errors on obstetrical wards from January 2009 through December 2013 using the error reporting system. We polled the hospital census statistics to compare their characteristics during the study period. It was not possible to blind the primary author to the date on which the errors occurred. In addition to compiling summary information, pre and post data were analyzed to determine error rates (e.g., the number of errors per 1000 patient days of care) and were compared using two-tailed, two-proportion tests based on the chi-squared statistic. This method tested for the equality of proportions in errors recorded in each system before and after EMR implementation, with an alpha level of 0.05 for all tests. We used R version 2.15.2 to perform all statistical analyses [9].
Results
One hundred fifty-nine medication errors were reported during the study period, 55 of which occurred after EMR adoption. The study period represented 53378 total days of patient care, 35329 before EMR adoption and 18049 following it. The overall error rate remained stable after the EMR implementation when adjusted for hospital census statistics (3.0 errors per 1000 patient days versus 2.9 errors per 1000 patient days, p>0.05). A significant difference was, however, noted by the ward in which errors occurred, with more errors being reported on the Labor and Delivery ward (Table 2).
Table 2: Locations of reported medication errors as a whole and by record system (*p<0.01, aChi-square test)
|
Location |
Pre-EMR (%) (n=104) |
EMR (%) (n=55) |
p-valuea |
|
Labor and delivery |
47 |
73 |
0.003* |
|
Ante/Postpartum |
53 |
27 |
0.003* |
Records which track the use of barcode scanning during medication administration were reviewed. Compliance during medication administration was consistently greater than 90% and not statistically different between the two wards. The hospital census databases did not reveal any differences in patient characteristics during the study period. Average patient length of stay and the most common admit and discharge diagnoses were similar before and after EMR implementation.
Discussion
Our data suggests that the introduction of the EMR had no effect on the reported rate of errors during the study period. Although a significant difference was observed between the error distributions between the two wards, the data plot suggests that this trend preceded the EMR introduction and was due only to transient variation (Figure 1). There were too few data points to reach valid conclusions about changes in error type or the medications involved. The overall error rate remained stable before and after EMR introduction, and was similar to a previously published single institution analysis [6]. There was no observed change in reported errors by operator (prescriber, dispenser, or medication administrator) which suggests that the observed differences were consistent across the phases of care and not due to other changes in hospital staffing and patient care. Likewise, the hospital admission and discharge diagnoses suggest that patient characteristics did not change during the study period.
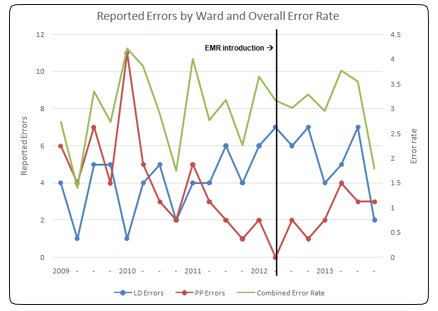
Figure 1: Plot of errors during study period Labor and Delivery Ward (LD), Ante/postpartum Ward (PP)
To our knowledge, this study represents the most recent analysis of medication errors on labor and delivery wards and the first since the wide-spread initiative to adopt EMR. Although larger scale, multicenter studies of self-reported medication errors have previously been published, they are limited in their ability to account for the variation in medication administration practices that exist between institutions. This is also the first attempt to relate changes in medication administration processes to error reporting statistics on peripartum wards.
Our study has several limitations. Although analysis of the hospital census and staffing statistics did not reveal any concurrent systemic changes that could account for the variation observed, the possibility exists. The transition from paper charting to computer based charting does put providers in more consistent contact with the computer based error reporting system and represents a steep learning curve, which may have increase the percentage of errors that were reported. Likewise, the addition of clinical decision support software may have increased awareness of potential medication errors, which has been shown to lead to increases in error reporting [10,11]. All of these effects could have contributed to the constant overall error rate through increased reporting, despite fewer errors resulting from EMR use overall.
Our study is limited to the experience of a single institution and a single type of EMR. It would be important to know the results of such a study at other institutions that differ from ours in terms of setting (urban vs. rural, academic vs. community, large vs. small) and type of EMR. Other institutions may have different experiences and other types of EMR may be more effective in preventing error. Furthermore, we were also limited by reliance on the self-reporting system for our data collection. Admittedly, self-reported errors make up a small fraction of all medication errors, but they serve as a benchmark in this case.
The 1999 report by the IOM brought attention to the magnitude of heath care related errors [1]. Medication errors rank amongst the most common source of errors associated with patient harm. A variety of changes have been proposed to improve health care practices and medication safety. After the IOM report, a task force was developed to advise healthcare providers about best practices for reducing medical errors. First published in 2001 and updated in 2013, the report recommended computerized physician order entry, barcode medication administration and clinical decision support software systems as methods to improve medication safety [3,12]. All three were listed as moderate level recommendation in the initial report and that status was maintained after the 2013 update. The reason cited was that the studies conducted during the intervening 11-year period did not show a sufficient reduction in errors that resulted in patient harm (adverse drug events) to strengthen the recommendation, despite an overall reduction in medication errors and an improvement in provider prescribing practices. The cost of adopting such systems presents a significant barrier to their use [13]. The true impact of implementing this technology may continue to be unclear as it is difficult and costly to design prospective randomized trials to assess their efficacy.
Obstetrical wards have previously been reported to have roughly half the error rates of other hospital wards in similar analyses [6]. Factors that may contribute to this include younger healthier patients who do not require multiple medications. However, there has been an increase in obstetrical patients with co-morbidities such as diabetes, obesity, hypertension, and advanced maternal age which will undoubtedly increase the complexities of care and risk of intrapartum complications. Preterm labor affects at least 12% of patients, and is typically treated with multiple medications [14]. These high risk obstetrical patients will most certainly require more medications including those, such as insulin, anticoagulation, magnesium sulfate and tocolysis, with a narrow therapeutic index, setting the stage for more potential error. Laboring patients are likewise more often treated with oxytocin and magnesium sulfate, both of which are associated with ADE.5EMR implementation has also been demonstrated to be associated with unintended changes in patient care and workflow [15].
EMR have been promoted as a method to reduce, if not eliminate, medication errors. Unfortunately, it is costly and difficult to implement well controlled trials to assess the impact of EMR on adverse drug events. One encouraging observation was of fewer errors reported as reaching the patients (Category C or higher) during the EMR phase of the study. This has previously been described with the adoption of barcode administration systems, and is attributable to the automation of tracking active medications and administration timing [16]. We were disappointed to see that the implementation of an EMR did not substantially affect the reported error rate or type. It may be with further experience with EMR and refinement of programs, the error rate will decrease. It will be important for others to report their experiences to determine if some types of EMR are more effective at reducing error than others.
Conclusion
Implementation of an electronic medical record did not reduce overall medication error reporting rates.
References
- Institute of Medicine. Committee on Quality of Health Care in America: To Err Is Human: Building a Safer Health System. Washington, DC: National Academy Press; (2000).
- Leape LL, Berwick DM, Bates DW 2002 What Practices Will Most Improve Safety? JAMA. July 288: 501-507.
- Shojania KG, Duncan BW, McDonald KM, Wachter RM, Markowitz AJ (2001) Making Health Care Safer. A Critical Analysis of Patient Safety Practices.
- Kfuri TA, Morlock L, Hicks RW (2008) Shore AD. Medication Errors in Obstetrics. Clin Perinatol 35: 101-117.
- Beyea SC, Kobokovich LJ, Becker SC, Hicks RW (2004) Medication Errors in the LDRP. AWHONN Lifelines 8: 130-140.
- Little JA, Velazquez MB, Rayburn WF (2003) Reported Medication Errors in Obstetric Inpatients in One Hospital. Journal of Reproductive Medicine 48: 818-820.
- Charles D, Furukawa M, Hufstader M (2012) Electronic Health Record Systems and Intent to Attest to Meaningful Use Among Non-federal Acute Care Hospitals in the US.
- Hartwig SC, Denger SD, Schneider PJ (1991) Severity-indexed, incident report-based medication error-reporting program. Am J Hosp Pharm 48: 2611-2616.
- Erdfelder E, Faul F, Buchner A (1996) GPOWER: a general power analysis program. Behavior Research Methods,Instruments, and Computers 28: 1-11.
- Boyer R, McPherson ML, Deshpande G, Smith SW (2009) Improving Medication Error Reporting in Hospice Care. Am J Hosp Palliat Care 26: 361-367.
- Hritz RW, Everly JL (2002) Care SA (2002) A Performance Improvement Approach. J Health Qual. Medication Error Identification is a Key to Prevention 24: 10-17.
- Shekelle PG, Wachter RM, Provonost PJ, Schoelles K, McDonald KM, et al. (2013) Making Health Care Safer II: An Updated Critical Analysis of the Evidence for Patient Safety Practices 211: 1-945.
- Blumenthal D, Glaser JP (2007) Information Technology Comes to Medicine. N Engl J Med 356: 2527-2534.
- Martin JA, Osterman MJK (2010) Sutton PD. Are Preterm Births on the Decline in the US? Recent Data from the National Vital Statistics System 39: 1-8.
- Campbell EM, Sittig DF, Ash JS, Kenneth P. Guappone, RichardH. Dykstra (2006) Types of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc 13: 547-56.
- Poon EG, Keohane CA, Yoon CS, Ditmore M, Bane A, et al. (2010) Effect of Bar-Code Technology on the Safety of Medication Administration. N Engl J Med 362: 1698-1707.