
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2021) Volume 6, Issue 3
The Diagnostic Dilemma of Ascites in Women
Received Date: Aug 09, 2021 / Accepted Date: Aug 17, 2021 / Published Date: Aug 23, 2021
Copyright: ©Bibi Zainab, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Bibi Zainab, Abdul Rahman, Fatima Moinuddin, Mohammad Moinuddin. (2021). The Diagnostic Dilemma of Ascites in Women. Int J Women's Health Care, 6(3), 199-204.
Abstract
Introduction: Ascites is the pathological accumulation of fluid within the peritoneal cavity. The most common causes of ascites are liver disease, vascular occlusion, congestive heart failure, pericarditis or nephrotic syndrome. We present to you case series of ascites as a common presentation in women, but each case with a different etio-pathogenesis related to gynecological benign disease. This case series highlights the importance, to consider gynecological problems among the potential differential diagnoses in women with ascites for early diagnosis and timely intervention.
Methods: We identified 5 female patients older than 18 years who presented with ascites as a common clinical presentation and we reviewed their medical records to assess demographic data, clinical presentation, imaging findings, co-morbid conditions, histo-pathologic features, pharmacologic therapies and surgical intervention.
Results: In all the five female patients, ascites was clinically diagnosed and confirmed with ultrasound of pelvis and abdomen. One of them noted to have pelvic tuberculosis, which was confirmed with endometrial biopsy and treated with antitubercular medication. One patient was diagnosed with adenomyosis and one other patient was diagnosed with leiomyoma, both patients were treated with total abdominal hysterectomy. One of the patients was diagnosed with endometriosis on laparotomy who was treated with gonadotrophin releasing hormone analogues. One of them was diagnosed with right sided ovarian fibroma, treated with right oophorectomy. All these patients had ascites as a common clinical presentation but with different underlying gynecological etiopathogeneses. The appropriate diagnosis and timely intervention in the above 5 cases resulted in complete resolution of symptoms.
Conclusion: As a healthcare worker, initial evaluation of a female patient with ascites, should rely on a detailed history and physical examination. In women with ascites, gynecologic problems should be considered among the potential differential diagnosis for appropriate management and timely intervention.
Keywords
Ascites, Endometriosis, Peritoneal Tuberculosis, Adenomyosis, Liomyoma, Fibroma
Introduction
Ascites is pathological accumulation of fluid within the peritoneal cavity [1,2]. The most common causes of ascites are liver disease, congestive heart failure, pericarditis, vascular occlusion, nephrotic syndrome and malignancy [3-6]. In women, gynecological benign diseases are one of the predisposing factors for ascites presenta¬tion. As the healthcare worker often gynecological causes for asci¬tes are less frequently considered as a differential diagnosis.
In this article we describe a case series of patients with ascites as a common presentation, but each case with a different etiopathogen- esis related to a gynecological disease.
This case series highlights the importance, to consider benign gynecologic problems such as abdominopelvic tuberculosis, ad¬enomyosis, endometriosis, fibroma and leiomyoma; among the potential differential diagnoses in women with ascites for early management and timely intervention [7-11].
Methods
After getting the verbal and written consent from the patients, we identified female patients older than 18 years between January 2019 to January 2021, who presented with abdominal distention as common clinical presentation. Patients with only underlying be¬nign gynecological conditions were included in the study.
We reviewed their medical records to assess demographic data, comorbidities, clinical presentation, imaging findings, histopathol-ogy findings and management. We then did manual chart review of identified medical records to verify which of these patients, were given the diagnosis of ascites with an underlying benign gyneco¬logical etiology. Once patients were included in the study their data was de-identified and coded using alphabets as (Patient A, B, C, D, E). Then variables like patient’s age, affected organs, associ¬ated conditions, disease course and management were abstracted on to a standardised assessment sheet.
Results
Between January 2019 and January 2021, a total of five female patients were clinically diagnosed with ascites.
Table 1 highlights the demographic data, clinical features, co-mor-bidities, and imaging study of the 5 female cases. The ages varied from 39 to 44 years, and all were Asian. All the five patients pre¬sented with abdominal distension as a common presenting symp¬tom. Patient A presented with fever, abdominal pain, abdominal distension, weight loss and irregular vaginal bleeding. Patient B presented with menorrhagia and abdominal distension. Patient C presented with dysmenorrhea dyspareunia abdominal bloating and abdominal distension. Patient D presented with only abdominal distension and patient E presented with menorrhagia and abdom¬inal distension.
Table 1: Demographic and Clinical Features of Female Patients with Ascites (n=5)
|
Pat ient ID |
Age (years) at time of diagn osis |
Ethini city/ Race |
Clinical presentation |
Obstetr ics history |
Co- morbid ities |
Pelvic exami nation |
Imaging |
|
A |
29 |
Asian |
Low grade fever (101F) Weight loss Irregular Vaginal bleeding Lower abdominal pain Abdominal distension |
Primary infertility |
None |
Tender fornic es. Cervical motion tender ness Mass in the left adnex a |
Ultrasound: Abdomen & Pelvis: Loculated intraperitoneal fluid, thickened peritoneum, minute nodules on the parietal peritoneum, thickened/ nodular omentum. Left sided peritubal adhesions with left beaded fallopian tubes. Multiloculated, thick, capsulated, cystic and solid left adnexal masses. |
|
B |
39 |
Asian |
Menorrhagia Abdominal distension |
P4 L4 |
None |
Bulky Uterus |
Ultrasound: Abdomen & Pelvis: Mottled heterogeneous appearing uterus, small myometrial lucent areas, with indistinct endometrial strip and pelvic intraperitoneal Fluid Figure 1. |
|
C |
22 |
Asian |
Dysmenorr hoea Dyspere-uni a Abdominal bloating & distension |
P1 L1 |
None |
Tenderness on deep pelvic exami nation |
Ultrasound: Abdomen & Pelvis: Normal appearing uterus, with obliterated recto-uterine pouch and intraperitoneal fluid with right sided endometrioma. |
|
D |
44 |
Asian |
Abdominal Distension |
P2 L2 |
Hypertension |
Right Adnex al Mass |
Ultrasound: Abdomen & Pelvis: Right adnexal hypoechoic mass with clear border and minimal doppler flow signal with intraperitoneal fluid |
|
E |
38 |
Asian |
Menorrhagia Abdominal distension |
P4 L4 |
Hypot hyroi-di sm |
Irregul ar Shape d Uteru s |
Ultrasound: Abdomen & Pelvis: Well-defined, solid masses in the myometrium with cystic degeneration Figure: 3 |
ID= Identification, P= Parity, A= abortion, L= Live
A few co-morbid conditions were identified, including hyperten-sion (n=1) and hypothyroidism (n=1). None of the patients were diagnosed with an underlying liver disease, kidney disease, vas-cular occlusive disease, congestive heart failure nor pericarditis. None of the patients were diagnosed with a malignancy based on routine age-based cancer screening guidelines at the time this manuscript was written with follow-up ranging from 1 to 2 years. The presence of ascites in all the patients was confirmed with ul¬trasound abdomen and pelvis, later these patients underwent ex-plorative laparotomy. All the patients had significant amount of free fluid in the peritoneal cavity (Table 2). The ascitic fluid analy¬sis in all the patients resulted to be exudate.
Table 2: Different Treatment Modalities Depending On the Diagnosis in Female Patients with Ascites (n=5)
|
Patient ID |
Intraoperati ve Findings |
Histopathol ogy |
Intraperiton eal fluid analysis (Ascitic fluid analysis) |
Diagnosis |
Manageme nt. Outcome. |
|
A |
Free fluid in the peritoneal cavity with multiple yellowish- white nodules on the visceral and parietal peritoneum , with significant peritoneal and visceral adhesions and with left beaded fallopian tubes. |
Endometria l biopsy: Multiple epithelioid cell granulomas scattered in the endometriu m, with Langhan’s giant cells suggestive of granulomat ous disease like tuberculosi s. |
Exudate. |
Pelvic tuberculosis |
Medical Management: Antitubercul ar therapy |
|
B |
Free fluid in the peritoneal cavity with uniformly enlarged uterus. |
Myometrial biopsy: Presence of endometrial stroma and glandular tissue within the smooth muscle of the myometriu m suggestive of adenomyosis. |
Exudate. |
Adenomyosis |
Surgical management: Hysterectomy |
|
C |
Complete obliteration of the pouch of Douglas and bladder was densely adherent to the lower uterus with free fluid in the peritoneal cavity right sided endometrioma |
Cul de sac biopsy: Multiple cuboidal glands , columnar glands of endometrial origin, suggestive of endometrio sis. |
Exudate |
Endometriosis |
Medical managment: Hysterectomy releasing hormone analogues. |
|
D |
Free fluid in the peritoneal cavity with round, oval, lobulated, well-circumscribe d grayish white, right sided ovarian tumor. |
Right ovary biopsy: Epithelioid round cells in vague cords and small nests separated by collagen fibers,sugg estive of fibroma. |
Exudate |
Benign ovarian tumor( Fibroma) |
Surgical management: Right sided Oopherectomy. |
|
E |
Enlarged uterus with multiple subserosal masses with free peritoneal fluid. |
Uterine mass biopsy: Spindle shaped smooth muscle cells suggestive of myoma. |
Exudate |
Leiomyoma |
Surgical management: Hysterectomy. |
Patient A had free fluid in the peritoneal cavity, multiple yellow-ish-white nodules on the visceral and parietal peritoneum, with significant peritoneal and visceral adhesions and left beaded fallo-pian tubes. The histopathology of endometrium biopsy specimen showed multiple epithelioid cell granulomas scattered in the endo-metrium, with Langhan’s giant cells suggestive of granulomatous disease like tuberculosis. After initiating antitubercular treatment patient was noted to have complete resolution of symptoms within 3 months. The patient was treated with antitubercular regimen for a total of nine months.
Patient B had free fluid in the peritoneal cavity with uniformly enlarged uterus. The histopathology of myometrium biopsy spec-imen showed endometrial stroma and glandular tissue within the smooth muscle of the myometrium suggestive of adenomyosis. Patient underwent total abdominal hysterectomy. There was com¬plete resolution of symptoms in 3 weeks.
Patient C had complete obliteration of the pouch of Douglas and bladder was densely adherent to the lower uterus right sided en-dometrioma with free fluid in the peritoneal cavity. The histopa-thology of Cul de sac biopsy showed multiple cuboidal glands and columnar glands with endometrial origin suggestive of endome-triosis. The patient treated with gonadotrophin releasing hormone analogues and there was complete resolution of symptoms in 6 months.
Patient D had large amount of free fluid in the peritoneal cavity with round, oval, lobulated, well-circumscribed, grayish white, right sided ovarian solid tumor. The right ovarian biopsy showed epithelioid round cells in vague cords and small nests separated by collagen fibers suggestive of fibroma. Patient underwent right sided oophorectomy with complete resolution of symptoms in 3 weeks.
Patient E had enlarged uterus with multiple subserosal masses with free peritoneal fluid. The uterine mass biopsy showed spin-dle shaped smooth muscle cells suggestive of leiomyoma. Patient underwent total abdominal hysterectomy. There was complete res¬olution of symptoms in 3 weeks
All the patients had different gynecological etiopathogeneses but with common clinical presentation as ascites. A detailed history and appropriate physical examination helps to consider benign gy-necological diseases as a potential etiology for ascites in women [12].
Discussion
Ascites is the excessive fluid collection in the abdominopelvic cavity, as a response to an underlying pathology [1,2]. The most common etiopathogenesis for ascites is related to hepato-renal diseases, cardiac disease and malignant diseases [3-6]. There is limited literature about benign gynaecological conditions causing ascites. This case series highlights the importance of considering benign gynaecological diseases like abdominopelvic tuberculosis, adenomyosis, endometriosis, fibroma and lieomyoma, as a differ¬ential diagnosis in women presenting with ascites [7-11].
Tuberculosis is a mycobacterial infection that most commonly manifests as pulmonary disease, but may affect multiple extra pulmonary sites, including abdominopelvic region [7]. The ab-dominopelvic tuberculosis is usually manifested in women of reproductive age [13-15]. These patients with abdomino-pelvic tuberculosis usually present with vague pelvic pain, abdominal distension, weight loss, fever and infertility [13-16]. On diagnostic imaging, pelvic tuberculosis may appear as ascites, peritoneal nod¬ules, omental or peritoneal thickening, or adnexal masses [15,16]. In this case series, patient A had similar signs and symptoms and radiological presentation which were confirmed on laparotomy. Patient A had a satisfactory response to anti-tuberculosis therapy and ascites resolved after anti-tuberculosis treatment [14,15].
Adenomyosis is a benign gynaecological disease characterised by the presence of ectopic endometrium within the myometrium [8]. The diffuse nature of the disease, makes it very difficult to clinical¬ly diagnose patients with adenomyosis [17-19]. It typically affects multiparous women over 30 years of age and may cause dysmen¬orrhea, menorrhagia, and abnormal vaginal bleeding [17,18]. In our case series, patient B was multiparous 39-year-old female with similar clinical presentation. noted to have adenomyosis, on ultra¬sound image. (Figure 1) She underwent total abdominal hysterec-tomy with complete resolution of symptoms. Till date, hysterecto¬my remains the standard of care [8,17-29].
Endometriosis is a gynaecological condition characterized by the presence of endometrial glands and stroma outside the endometrial cavity [9]. Patients usually present with dysmenorrhea, dyspareu¬nia and dyschezia [20]. The ectopic nature of the endometrial tis¬sue makes it difficult to diagnose endometriosis [9,20]. The pres¬ence of ascitic fluid in endometriosis is usually due to irritation on the serosal surfaces caused by free blood in the peritoneal cavi¬ty during the menstruation [20-22].
Gonadotropin analogues are widely used as a way to induce hypoestrogenism, causing regres¬sion of the ectopic endometrial tissue [9,20-22]. In our case series, the patient C was diagnosed with endometriosis and right sided endometrioma.( Figure:2) She was treated with gonadotropin re¬leasing hormone analogues, which resulted in complete resolution of symptoms in 6 months [20-22]. Ovarian fibromas are benign ovarian tumors [10]. These tumors are composed of spindle, oval, or round cells forming variable amounts of collagen [23-25]. The patients usually present with as¬cites pleural effusion and abdominal pain [10,23,24]. In this case series patient D presented with abdominal distension, secondary to ascites. After confirming the diagnosis, she underwent right sided oopherectomy with complete resolution of symptoms [23-25].
Uterine leiomyoma is the benign tumor of uterine smooth mus-cle [11]. Patients usually present with dysmenorrhea, menorrhagia and abdominal distension [26]. An ultrasonography is the initial diagnostic tool for the confirmation of the diagnosis [11,26]. The current management strategies involve mainly surgical interven¬tions which include total hysterectomy versus partial myomecto-my depending on the patient’s age and her desire to preserve fer-tility [27]. In this case series patient E is a 38-year-old female who had completed her family with four children, she presented with menorrhagia and abdominal distension. Uterine leiomyoma was noted on the ultrasound imaging.(Figure:3) As she did not desire any further children she opted for total abdominal hysterectomy.
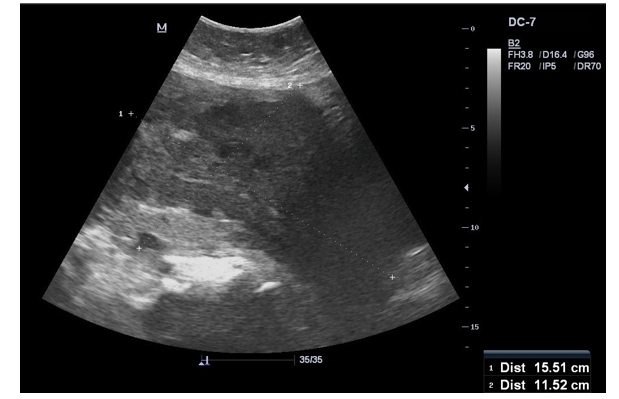
Figure 1: Adenomyosis

Figure 2: Anterior Wall Leiomyoma
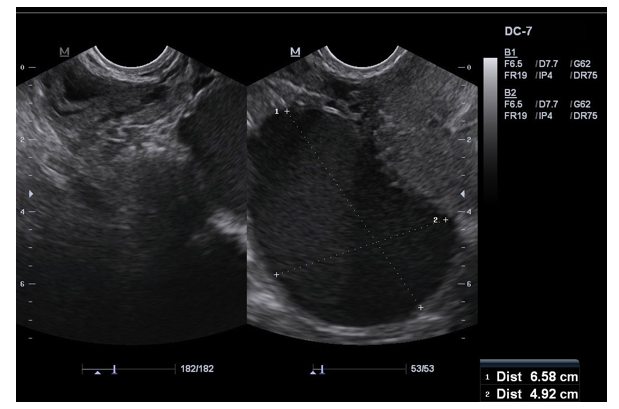
Figure 3: Endometriosis with Right Sided Endometrioma
Conclusion
As a healthcare worker, initial evaluation of a female patient with ascites, should rely on a detailed history and physical examination [12]. In women with ascites, gynaecologic problems such as ab¬dominopelvic tuberculosis, adenomyosis, endometriosis, fibroth-ecoma and leiomyoma should be considered among the potential differential for appropriate diagnosis and timely intervention.
References
- Arroyo V (2002) Pathophysiology, diagnosis and treatment ofascites in cirrhosis. Ann Hepatol. 1: 72-79.
- JC, Canawati HN, Sapico FL, Hopkins RR, Weiner J, et al. (1982) Spontaneous bacterial peritonitis. Hepatology 2: 399- 407.
- Runyon BA (2009) Management of adult patients with ascites due to cirrhosis: an update. Hepatology 49: 2087-2107.
- Marcus RG, Messana J, Swartz R (1992) Peritoneal dialysis in end-stage renal disease patients with preexisting chronic liver disease and ascites. Am J Med 93: 35-40.
- Runyon BA (1988) Cardiac ascites: a characterization. J ClinGastroenterol 10: 410-412.
- Garrison RN, Kaelin LD, Galloway RH, Heuser LS (1986) Malignant ascites. Clinical and experimental observations. Ann Surg 203: 644-651.
- Wang PH, Yuan CC (2001) Tuberculous peritonitis. Am J Obstet Gynecol 184: 250-251.
- Matalliotakis IM, Kourtis AI, Panidis DK (2003) Adenomyosis. Obstet Gynecol Clin North Am 30: 63-82.
- Spaczynski RZ, Duleba AJ (2003) Diagnosis of endometriosis. Semin Reprod Med 21:193-208.
- Loué VAS, Gbary E, Koui S (2013) Bilateral ovarian fibroth-ecoma associated with ascites, bilateral pleural effusion, and marked elevated serum CA-125. Case Rep Obst Gynecol 2013: 189072.
- Commandeur AE, Styer AK, Teixeira JM (2015) Epidemiological and genetic clues for molecular mechanisms involved in uterineleiomyoma development and growth[J]. Hum Reprod Update.
- Cattau EL, Benjamin SB, Knuff TE, Castell DO (1982) The accuracy of the physical examination in the diagnosis of suspected ascites. JAMA 247: 1164-1166.
- Huang YJ, Wei LH, Hsieh CY (2004) Clinical presentation of pelvic tuberculosis imitating ovarian malignancy. Taiwan J Obstet Gynecol 43: 29-34.
- Sharma JB, Roy KK, Pushparaj M, Kumar S, Malhotra N, et al. (2008) Laparoscopic findings in female genital tuberculosis. Arch Gynecol Obstet 278: 359-364.
- Bilgin T, Karabay A, Dolar E, Develiog Ì? lu OH (2001) Peritoneal tuberculosis with pelvic abdominal mass, ascites and elevated CA 125 mimicking advanced ovarian carcinoma: a series of 10 cases. Int J Gynecol Cancer 11: 290-294.
- Koc S, Beydilli G, Tulunay G (2006) Peritoneal tuberculosis mimicking advanced ovarian cancer: a retrospective review of 22 cases. Gynecol Oncol 103: 565-569.
- Taran FA, Stewart EA, Brucker S (2013) Adenomyosis: epidemiology, risk factors, clinical phenotype and surgical and interventional alternatives to hysterectomy. Geburtshilfe Frauenheilkd 73: 924-931
- Radzinsky VE, Khamoshina MB, Nosenko EN (2016) Treatment strategies for pelvic pain associated with adenomyosis. Gynecol Endocrinol 32: 19-22.
- Habiba M, Benagiano G, Brosens I (2016) The pathophysiology of adenomyosis. In: Habiba M, Benagiano G, editors. Uterine adenomyosis. Cham: Springer 45-70.
- Missmer SA, Hankinson SE, Spiegelman D (2004) Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol 160: 784-796.
- Jenks JE, Artman LE, Hoskins WJ, Miremadi AK (1984) Endometriosis with ascites. Obstet Gynecol 63: 755-775.
- Dmowski WP, Lesniewicz R, Rana N, Pepping P, Noursalehi M (1997) Changing trends in the diagnosis of endometriosis: a comparative study of women with pelvic endometriosis presenting with chronic pelvic pain or infertility. Fertil Steril 67: 238-243.
- Takeshita T, Shima H, Oishi S (2005) Ovarian fibroma (fi-brothecoma) with extensive cystic degeneration: unusual MR imaging findings in two cases. Radiat Med 23: 70-74.
- Meigs JV (1954) Fibroma of the ovary with ascites and hydro-thorax-Meigs syndrome. Am J Obstet Gynecol 67: 962-985.
- Athey PA, Malone RS (1987) Sonography of ovarian theco-mas. J Ultrasound Med 6: 431-436.
- Yi-Wei Wang, Qiong Fan, Zhao-Xia Qian, Jin-Jin Wang, Yu-Hong Li, et al. (2021) Abdominopelvic leiomyoma with large ascites: A case report and review of the literature. World Journal of Clinical Cases 9: 1424-1432.
- Bibi Z, Fatima M, Cavity saving surgery in Large Fibroid in nulliparous women: A case report. RJMS Vol: 11 Issue: 3eISSN: 2231-1947pISSN 2231-1947.