
COVID Research: Open Access(CROA)
ISSN: 2995-7826 | DOI: 10.33140/CROA


Review Article - (2023) Volume 1, Issue 1
The Biochemistry and Pathology Characteristics of Coronavirus Disease 2019
2Department of Obstetrics & Gynecology, Faculty of Medicine, University of Saba Region, Marib, P.R, Yemen
3Department of Obstetrics & Gynecology, Faculty of Medicine & Health Sciences, Amran University, Amra, Yemen
Received Date: Oct 03, 2023 / Accepted Date: Nov 05, 2023 / Published Date: Nov 28, 2023
Copyright: ©Â©2023 Hasan A. M. M. Almansoub, et al. This is an openaccess article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Almansoub, H. A. M. M., Sakaf, N. M. A., Almansoob, R. (2023). The Biochemistry and Pathology Characteristics of Coronavirus Disease 2019. COVID Res OA, 1(3), 47-50.
Abstract
Coronavirus Disease 2019 started appeared in December 2019 China’s, Hubei Province, Wuhan. During the following three months, it spread rapidly to numerous provinces in China and transversely the world. The initial bunch was epidemiologically associated with a seafood wholesale market in Wuhan. Many essential aspects of the pathogenesis, pathology, and pathophysiology of SARS- CoV2 have not yet clear. Here, we offer a comprehensive overview of the biochemistry Characteristics and histopathological results present in various organs and cells and the pathophysiology. In this review we found many damage in some organic system, such as pulmonary edema with hyaline membrane formation, desquamation and hyperplasia of pneumocytes, proteinaceous in Respiratory tract, spleen atrophic, degeneration and focal necrosis of hepatocytes, Esophageal, stomach and bowel in digestive tract. Degenerated or necrosed myocardial cells in Heart. Degeneration and shedding of renal tubules epithelial cells, hyaline casts in Kidneys and other organs.
Keywords
SARS- CoV2, Histopathology, Pathophysiology, Biochemistry, Lung.
Introduction
Severe acute respiratory syndrome 2 (SARS- CoV2) started emerged in China’s Hubei Province in December 2019 in Wu- han. During the following three months, it spread rapidly to many provinces in China and across the world. The initial cluster was epidemiologically associated with a seafood wholesale market in Wuhan. However, many of the first 41 cases had later reported having no known exposure to the market [1]. The WHO raised the COVID-19 to pandemic worldwide, March, 2020, it seems to be very contagious and has quickly spread worldwide. This vi- rus COVID-19 belongs to a family of large, enveloped, positive, and single-stranded RNA viruses that cause SARS and MERS [2-4]. It isolated from lower respiratory tract samples of 4 cases [5], COVID-19 infection typically causes severe manifestations related to the lower respiratory tract [6]. COVID-19 has a char- acteristic clinical, where patients had shown like to other coro- navirus symptoms, counting fever, fatigue, muscle ache, cough, and dyspnea, whereas diarrhea, confusion, headache and vomiting were rare [7-10]. The pathological characteristics of SARS - CoV2 closely resemble those detected in MERS and SARS coronavirus infections [11]. The effective pathological outcome in these cases of patients with SARS - CoV2 was diffuse alveolar damage (DAD) [10]. This severe lung injury and others organs such as liver, in cases with COVID-19 is caused by both direct viral effects and immunopathogenic factors [12]. Many essential aspects of the pathogenesis, pathology, and pathophysiology of COVID-19 have not yet clear. Here, we offer a comprehensive overview of the bio- chemistry and histopathological results present in various organs and cells and the pathophysiology.
Clinical Biochemistry Characteristics of Severe acute Re- spiratory Syndrome 2
Life pattern of COVED-19 in host cells starts with the authori- tative of S proteins to cell receptor Angiotensin converting en- zyme 2(ACE2). Subsequent to bound, the adaptation of S protein changed promotes viral envelope combination with cell layer through endocytosis pathway. ACE2 is one of the major receptors for SARS-CoV and SARS-CoV-2 [13,14].The white blood cell contain was lower than ordinary in 9% of patients, and neutro- phil include expanded in 38% of patients. Lymphocytes and he- moglobin in numerous patients were underneath the typical range. Numerous patients similarly created unusual myocardial protein profiles with expanded creatine kinase (CK) and expanded lactate dehydrogenase (LDH). A few patients demonstrated anomalous liver capacity in changing degrees, indicating expanded alanine aminotransferase (ALT) or aspartate aminotransferase (AST). A few patients likewise created differing degrees of renal hindrance, indicating expanded blood urea nitrogen (BUN) or serum creati- nine (Cr) [7]. Of the 9 patients, 5 had lymphopenia (< 1.0×109/L) and 3 had raised ALT and AST, of which 1 had an ALT level of 2093 and a degree of 1263 U/L [13].
Numerous biomarkers have been related with helpless results and speak to a contender for hazard definition models for fore- seeing serious SARS-CoV-2 so as to direct clinical consideration. Among all, lymphopenia, thrombocytopenia, leukocytosis, CRP, PCT, LDH, AST, ALT, D-dimer, cTn represent the most prescient boundaries of extreme SARS-CoV-2 [15].
The pathology and pathophysiology of severe acute respi- ratory syndrome 2 Pathology
There is currently a lack of pathology that has been described since the first epidemic in December 2019 on COVID-19, biopsy, or au- topsy. Although, the coronavirus disinfection in histopathological laboratories. It appears reasonable to refrain from working frozen sections on potential cases of COVID-19 except the laboratory is certain in curbing aerosols in the cryostat; and make confirmed that formalin fixation and paraffin embedding should inactivate COVID-19 [16]. The pathological findings of Certain human or- gans of SARS-CoV-2, such as the Lungs, Liver, Heart and other organs, are imperfectly described. For ease of reference, the pri- mary pathological findings for each organ summarized in Table 1. These pathological characteristics of SARS-CoV 2 show essential similarities to SARS-CoV and MERS-CoV infection [10, 15, 17, 18].
Pathophysiology
Pathophysiology and virulence mechanisms of Coronavirus, and hence also of COVID-19 have connections to the function of the non-structural proteins (nsps) and structural proteins. For example, research underlined that nsps could block the host innate immune response [19] , thus founds immune dysfunction is a common char- acteristic in cases of COVID-19 that might be an essential factor correlated with disease severity and mortality [14]. Early studies on SARS-CoV and MERS-CoV infection there have shown that increased amounts of proinflammatory cytokines in serum SARS patients (e.g., IL1B, IL6, IL12, IFNγ, IP10, and MCP1) [20], and MERS patients (e.g., IFNγ, TNFα, IL15, and IL17) [21], were associated with pulmonary inflammation and general lung damage [20-23]. SARS-CoV2 infection also reported had high amounts of cytokines in patient’s serum (e.g., IL1B, IFNγ, IP10, GCSF, MCP1, MIP1A, and TNFα) [1]. Moreover, patients requiring ICU admission had higher amounts of some cytokines than did those not requiring ICU admission, suggesting that the cytokine storm was associated with disease severity [1]. However, COVID-19 infection, probably leading to activated T-helper-1 (Th1) cell re- sponses, also initiated increased secretion of T-helper-2 (Th2) cytokines (e.g., IL4 and IL10) that repress inflammation, which varies from SARS-CoV infection [1, 20].
As know, Coronaviruses are the envelope, positive-stranded RNA viruses. Between the functions of structural proteins, the envelope has a crucial role in virus pathogenicity as it promotes viral at- tachment and release. Amongst the fundamental components of Coronaviruses, there are the spike glycoproteins composed of two subunits (S1 and S2). Of note, in COVID-19, the S2 subunit, in- cluding a fusion peptide, a transmembrane domain, and cytoplas- mic domain, is highly conserved. The dysfunction results as a re- sult of the dysregulated host response to infection by COVID-19, signs dysfunction include severe dyspnea, low oxygen saturation, impaired renal function, reduced urine output, tachycardia, acute heart injury, hypotension, cold extremities, skin mottling, abnor- mal liver function and altered mentation [1, 8, 24, 25]. Besides, 5% of patients can develop severe disease with features of respiratory failure, cardiac injury, septic shock, Raetia, or multiple organ dys- function [24, 26].
|
Organs |
Pathology changes |
References |
|
Respiratory tract |
Diffuse alveolar damage showed pulmonary edema with hyaline membrane for- mation, desquamation and hyperplasia of pneumocytes, proteinaceous, Interstitial mononuclear inflammatory infiltrates, dominated by lymphocytes, multinucleated syncytial cells with atypical enlarged pneumocytes characterized by large nuclei, amphophilic granular cytoplasm, and prominent nucleoli were identified in the intra-alveolar spaces, showing viral cytopathic-like changes. |
[6, 25, 27] |
|
Immune System |
Spleen: Spleen atrophic, Macrophage’s proliferation and phagocytosis, Focal hem- orrhage and necrosis. lymph nodes: decreased number of lymphocytes and focal necrosis. Decreases of CD4+ and CD8+ T-cell levels, and abnormal cytokine levels in the spleen and lymph nodes. Bone marrow: Myelopoiesis is decreased in bone marrow. |
[14] |
|
Digestive tract |
Liver: Micro vesicular steatosis and mild lobular and portal activity, a few inter- stitial mononuclear inflammatory infiltrates, degeneration and focal necrosis of hepatocytes. Esophageal, stomach and bowel: Degeneration, necrosis and desqua- mation of epithelium mucosae of variable degree. The gallbladder is prominently distended. |
[6, 14, 27, 28] |
|
Heart and blood vessels |
Heart: A few interstitial mononuclear inflammatory infiltrates, Degenerated or ne- crosed myocardial cells. Blood vessels: Shedding of endothelial cells, end vasculitis and thrombi. |
[10, 27] |
|
Central nervous system |
Degeneration of some neurons, neurological manifestations, Cerebral hyperemia and edema, SARS-CoV-2 causes neuroinflammation & induces Lewy body forma- tion in the brains of macaques. |
[29, 30] |
|
Kidneys |
Kidneys: Degeneration and shedding of renal tubules epithelial cells, and hyaline casts. Microthrombi and fibrotic foci are found in the kidney interstitium. |
[27] |
|
Glands |
Necrotic foci are noted in the adrenal glands. |
[27] |
Table 1: The pathological changes in different organs and tissue
COVID-19 is a systemic disease that can move beyond the lungs by blood-based dissemination to affect multiple organs. These organs include the kidney, liver, muscles, nervous system, and spleen. The early cell-based portal for viral entry is through the angiotensin-con- verting enzyme 2 receptor.
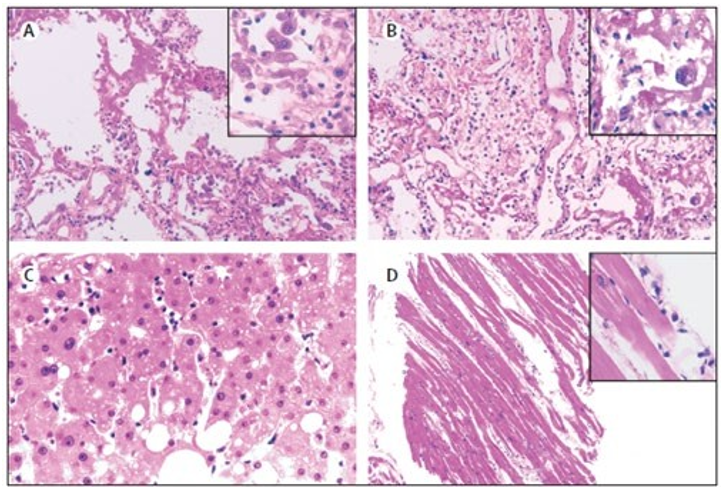
Figure 1: Pathological Manifestations of Right (A) And Left (B) Lung Tissue, Liver Tissue (C), And Heart Tissue (D) In A Patient With Severe Pneumonia Caused By Sars-Cov-2[6].
SARS-CoV-2=severe acute respiratory syndrome corona virus 2.
Conclusion
In conclusion, COVID-19 epidemics can occur anywhere and the indication designated that this novel Coronavirus has an etiologic role in severe acute respiratory syndrome. This new virus appears to be very transmissible and has quickly spread worldwide. SARS- CoV-2 has been shown to infect human respiratory epithelial cells and lung tissue, also damage Liver, stomach, duodenum, and rectal mucosa in patients. Furthermore, the Immunopathology may also play a pertinent role in the development of disease harshness.
References
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., ... & Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet, 395(10223), 497-506.
- Gu, J., & Korteweg, C. (2007). Pathology and pathogenesis of severe acute respiratory syndrome. The American journal of pathology, 170(4), 1136-1147.
- Ng, D. L., Al Hosani, F., Keating, M. K., Gerber, S. I., Jones,T. L., Metcalfe, M. G., ... & Zaki, S. R. (2016). Clinicopath- ologic, immunohistochemical, and ultrastructural findings of a fatal case of Middle East respiratory syndrome coronavirus infection in the United Arab Emirates, April 2014. The Amer- ican journal of pathology, 186(3), 652-658.
- Marra, M. A., Jones, S. J., Astell, C. R., Holt, R. A., Brooks-Wil-son, A., Butterfield, Y. S., ... & Roper, R. L. (2003). The ge- nome sequence of the SARS-associated coronavirus. Science, 300(5624), 1399-1404.
- Zhu, N., Zhang, D., Wang, W., Li, X., Yang, B., Song, J., ... & Tan, W. (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England journal of medicine, 382(8), 727-733.
- Xu, Z., Shi, L., Wang, Y., Zhang, J., Huang, L., Zhang, C., ... & Wang, F. S. (2020). Pathological findings of COVID-19 as- sociated with acute respiratory distress syndrome. The Lancet respiratory medicine, 8(4), 420-422.
- Chen, N. Epidemiological and Clinical Characteristics of 99 Cases of 2019-Novel Coronavirus (2019-nCoV) Pneumonia in Wuhan, China.
- Wang, D., Hu, B., Hu, C., Zhu, F., Liu, X., Zhang, J., ... & Peng, Z. (2020). Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. jama, 323(11), 1061-1069.
- Zhu, J., Zhong, Z., Ji, P., Li, H., Li, B., Pang, J., ... & Zhao,C. (2020). Clinicopathological characteristics of 8697 patients with COVID-19 in China: a meta-analysis. Family medicine and community health, 8(2).
- Guan, W. J., Ni, Z. Y., Hu, Y., Liang, W. H., Ou, C. Q., He,J. X., ... & Zhong, N. S. (2020). Clinical characteristics of coronavirus disease 2019 in China. New England journal of medicine, 382(18), 1708-1720.
- Ding, Y., Wang, H., Shen, H., Li, Z., Geng, J., Han, H., ... & Yao, K. (2003). The clinical pathology of severe acute respi- ratory syndrome (SARS): a report from China. The Journal of Pathology: A Journal of the Pathological Society of Great Britain and Ireland, 200(3), 282-289.
- Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., ... &Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The lancet, 395(10223), 497-506.
- Alqahtani, S. A., & Schattenberg, J. M. (2020). Liver injury in COVID-19: The current evidence. United European gastroen- terology journal, 8(5), 509-519.
- Zhang, C., Shi, L., & Wang, F. S. (2020). Liver injury in COVID-19: management and challenges. The lancet Gastro- enterology & hepatology, 5(5), 428-430.
- Nassar, M., Bakhrebah, M. A., Meo, S. A., Alsuabeyl, M. S., & Zaher, W. A. (2018). Middle East Respiratory Syndrome Coronavirus (MERS-CoV) infection: epidemiology, patho- genesis and clinical characteristics. Eur Rev Med Pharmacol Sci, 22(15), 4956-4961.
- Henwood, A. F. (2020). Coronavirus disinfection in histopa- thology. Journal of histotechnology, 43(2), 102-104
- Hui, D. S., & Zumla, A. (2019). Severe acute respiratory syn- drome: historical, epidemiologic, and clinical features. Infec- tious Disease Clinics, 33(4), 869-889.
- van den Brand, J. M., Smits, S. L., & Haagmans, B. L. (2015). Pathogenesis of Middle East respiratory syndrome coronavi- rus. The Journal of pathology, 235(2), 175-184.
- Lei, J., Kusov, Y., & Hilgenfeld, R. (2018). Nsp3 of corona- viruses: Structures and functions of a large multi-domain pro- tein. Antiviral research, 149, 58-74.
- Wong, C. K., Lam, C. W. K., Wu, A. K. L., Ip, W. K., Lee, N.L. S., Chan, I. H. S., ... & Sung, J. J. Y. (2004). Plasma inflam- matory cytokines and chemokines in severe acute respiratory syndrome. Clinical & Experimental Immunology, 136(1), 95- 103.
- Mahallawi, W. H., Khabour, O. F., Zhang, Q., Makhdoum, H. M., & Suliman, B. A. (2018). MERS-CoV infection in hu- mans is associated with a pro-inflammatory Th1 and Th17 cytokine profile. Cytokine, 104, 8-13.
- He, L., Ding, Y., Zhang, Q., Che, X., He, Y., Shen, H., ... & Ji-ang, S. (2006). Expression of elevated levels of pro-inflamma- tory cytokines in SARS-CoV-infected ACE2+ cells in SARS patients: relation to the acute lung injury and pathogenesis of SARS. The Journal of Pathology: A Journal of the Pathologi- cal Society of Great Britain and Ireland, 210(3), 288-297.
- Faure, E., Poissy, J., Goffard, A., Fournier, C., Kipnis, E., Ti- tecat, M., ... & Guery, B. (2014). Distinct immune response in two MERS-CoV-infected patients: can we go from bench to bedside?. PloS one, 9(2), e88716.
- Cascella, M., Rajnik, M., Aleem, A., Dulebohn, S. C., & Di Napoli, R. (2020). Features, evaluation, and treatment of coronavirus (COVID-19).
- Tian, S., Hu, W., Niu, L., Liu, H., Xu, H., & Xiao, S. Y. (2020).Pulmonary pathology of early-phase 2019 novel coronavirus (COVID-19) pneumonia in two patients with lung cancer. Journal of thoracic oncology, 15(5), 700-704
- Wang, Y., Wang, Y., Chen, Y., & Qin, Q. (2020). Unique epi- demiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special con- trol measures. Journal of medical virology, 92(6), 568-576.
- Wei, P. F. (2020). Diagnosis and treatment protocol for nov- el coronavirus pneumonia (trial version 7). Chinese medical journal, 133(9), 1087-1095.
- Xiao, F., Tang, M., Zheng, X., Liu, Y., Li, X., & Shan, H. (2020). Evidence for gastrointestinal infection of SARS- CoV-2. Gastroenterology, 158(6), 1831-1833.
- Mao, L., Wang, M., Chen, S., He, Q., Chang, J., Hong, C., ... & Hu, B. (2020). Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. MedRxiv, 2020-02.
- Philippens, I. H., Böszörményi, K. P., Wubben, J. A., Fagrouch, Z. C., van Driel, N., Mayenburg, A. Q., ... & Verschoor, E. J. (2021). SARS-CoV-2 causes brain inflammation and induces Lewy body formation in macaques. bioRxiv, 2021-02.