




Research Article - (2025) Volume 4, Issue 2
Telemedicine in Postoperative Follow-Up Care After Major Elective Gynaecological Surgery in Low Resource Setting: A Feasibility Study
2Department of Community Medicine, University College of Medical Science and GTB Hospital, New Delhi, India
Received Date: Apr 21, 2025 / Accepted Date: May 23, 2025 / Published Date: May 30, 2025
Copyright: ©Â©2025 Aastha Chaurasia, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Chaurasia, A., Guleria, K., Maroof, K. A., Sharma, R., Singh, A. (2025). Telemedicine in Postoperative Follow-Up Care After Major Elective Gynaecological Surgery in Low Resource Setting: A Feasibility Study. J Surg Care,4(2), 1-13.
Abstract
Objectives: To assess the feasibility of ‘Tele-health Postoperative follow-up care Model’ in terms of provider, process and service recipient and to identify barriers, facilitators, robustness, safety and acceptability of the model.
Design: Feasibility Study
Setting: UCMS and GTB Hospital, Delhi, India
Population: Patients admitted in gynaecology ward for major elective gynaecological surgery
Methods: Women undergoing major elective gynaecological surgery from May 2023 to November 2024 were enrolled for follow-up using a telehealth model, consisting of virtual visits on days 7, 14, and 30, and a physical visit on day 42. Participants completed Modified Quality of Recovery-15 (QoR-15) forms and satisfaction questionnaires.
Main Outcome Measures: Feasibility of telemedicine follow-up (virtual vs. physical visits), provider and recipient satisfaction scores, technological performance, barriers (connectivity issues, missed appointments), facilitators (time and cost savings), efficacy (successful care delivery, complications), safety, and acceptability (adherence, satisfaction, costs).
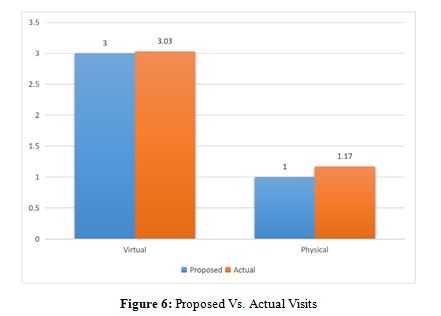
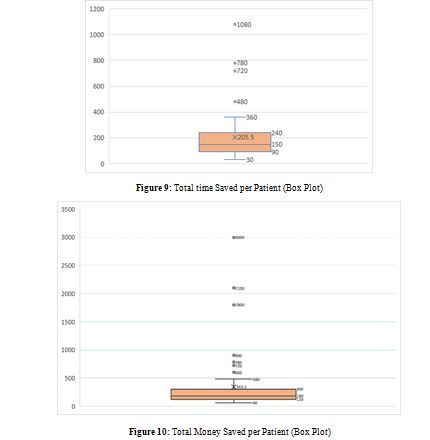
Results: It was feasible to complete the ‘model’ follow-up in 60 patients with average number of 3.03 ± 0.18 virtual visits & 1.17 ± 0.41 physical visits respectively. Patient satisfaction was scored at (4.81/5) while provider satisfaction ranged from 4.73 to 4.95/5 through this model. In addition, patients saved on an average 205 minutes and 343.50 INR. Complications were encountered in 13.3% cases; majority managed successfully. 88.30% patients preferred a similar follow-up telehealth model in future. Modified QoR-15 score progressively increased throughout visits.
Conclusion: Tele-health post-operative follow-up care model can be used as an upgradation to the existing postoperative services, even in low resource settings.
Keywords
Telemedicine, Postoperative Care, Gynaecological Surgeries
Introduction
The CoVID 19 pandemic has resulted in several shifts in the traditional mode of healthcare delivery. The introduction and successful implementation of telemedicine has led to reduction in burden on hospitals & access to timely treatment decreasing the cost of travel and waiting time for patients; thus, improving the overall healthcare experience [1]. Telemedicine, having gained global recognition, is now being actively promoted and integrated into India’s healthcare system. The rapid growth of the internet in India is significantly enhancing telemedicine by increasing accessibility and connectivity. The Indian government has implemented guidelines to standardize and strengthen telemedicine practices and integrate them into the public health framework [2]. Consequently, public hospitals are increasingly adopting telemedicine to improve healthcare access and overcome barriers like distance and limited resources.
The role of telemedicine in postoperative care is a promising domain. It helps clinicians in close monitoring of patients and early detection and treatment of postoperative complications as well as leads to decrease patient travel time, distance and cost along with a higher patient satisfaction rate without compromising clinical outcomes [1]. Telemedicine is now being used increasingly in different domains of surgical care to speed up and simplify preoperative imaging, work-up and consultation for patients. Prior to surgery, telemedicine consultations can often assist in identifying and resolving any obstacles to a healthy recovery at home [3].
Despite these advancements, the application of telemedicine in postoperative care- especially elective gynaecological surgeries, remains under researched. Women particularly in underserved and rural areas face unique challenge in accessing quality postoperative care, resulting in significant disparities in health outcomes. We proposed testing the feasibility of this model as an upgrade to our existing postoperative services. It will enable closer follow-up, early detection of complications, and streamlined communication, thereby improving patient outcomes and satisfaction and enhancing the overall postoperative care experience, close gaps in access and quality of care, thereby improving health outcomes and promote equity in healthcare delivery. The aim of this study was to assess the feasibility of Telemedicine in delivery of postoperative follow-up care after major elective gynaecological surgery in a tertiary care hospital of a low resource setting.
Methods
The study was conducted in Department of Obstetrics and Gynaecology at University College of Medical Sciences & Guru Teg Bahadur Hospital, New Delhi between May 2023 to November 2024. The participants were recruited from the gynaecological wards of Guru Teg Bahadur Hospital.
Study Design and Sample Size
This was a feasibility study aimed at exploring the use of telemedicine in postoperative care for women undergoing elective gynaecological surgery for benign conditions in a low-resource setting. A sample size of 60 was chosen based on convenience, as no estimation or hypothesis testing was involved. The study did not account for a dropout rate, considering that dropouts themselves could be indicative of the feasibility of telemedicine in this context.
Inclusion and Exclusion Criteria
The inclusion criteria for the study consisted of women aged over 18 years who were undergoing major elective gynaecological surgery for benign conditions and were willing and able to provide informed consent. Participants were also required to be familiar with smartphones or internet-enabled devices and have access to 24/7 emergency healthcare. Women undergoing surgery for cancer, those requiring extended hospitalization beyond postoperative day 6, and those experiencing significant intra/ postoperative complications (graded 3 or higher by the Clavien- Dindo Classification) were excluded from the study [4].
Tele-health Postoperative Follow-Up Model
Postoperative care in our hospital (post discharge) usually includes an in-person visit for suture removal and overall recovery around day 10 and a more comprehensive follow-up and review of histopathology around four weeks post-surgery. This study aimed to replace these visits with telemedicine, evaluating feasibility, effectiveness, and patient satisfaction. The model consisted for 3 virtual visits at day 7,14 and 30 and 1 physical visit at day 45 postoperatively (Table 1).
|
NO. OF VISITS |
TYPE OF VISIT |
PROCEDURE OF CARE |
|
1. |
Post-Op Day 7 Virtual Visit 1 |
|
|
2. |
Post-Op Day14 Virtual Visit 2 |
|
|
3. |
Post-Op Day 30 Virtual Visit 3 |
|
|
4. |
6week post-Op One Physical Visit |
|
Table 1: Proposed ‘Tele-Health-Postoperative Follow-up Care’ Model
Patients were first screened based on the eligibility criteria. Once they met the criteria and agreed to participate & gave informed consent, their details were recorded in structured Proforma. Each participant received a ‘Patient Information Sheet’ either in physical or virtual form, where they learned about the “Tele-health Postoperative Follow-Up Care Model” and how virtual visits would work. They were also shown how to use the required technology, like taking their vitals, clicking pictures and setting up video calls. Before each visit, patients were asked to measure their pulse, blood pressure, and temperature.
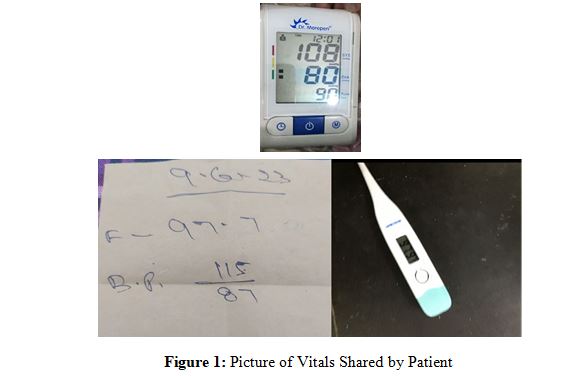
They were encouraged to use a smartphone or computer with a stable internet connection for the consultations.

Informed written consent was obtained from all participants, with implied consent for patient-initiated teleconsultations and explicit consent, documented via email, text, audio/video messages, or verbal agreement, for healthcare provider-initiated consultations. In emergency situations, patients were instructed to contact the Tele-health provider, and if unable to do so, were advised to visit the Gynae-casualty of the Department of Obstetrics and Gynaecology at GTB Hospital.
Data Collection
Sociodemographic and clinical data were collected at recruitment using a case record form, while participant satisfaction was assessed through questionnaires with Likert scale responses after both virtual and physical visits. Recovery was evaluated using the Modified QoR-15 scale, adapted to include gynaecological complications, focusing on physical, emotional well-being, and issues like pain, fever, and vaginal bleeding.
Study Outcomes
The primary outcomes of the study assessed the feasibility of the Tele-health postoperative follow-up care model through the number of virtual and physical visits, provider ability to deliver and accept the model, compliance, difficulties faced, and satisfaction after each virtual visit. It also evaluated technological parameters at both ends, the average time taken to assess and manage each case, recipient understanding and satisfaction through feedback surveys, and the model's impact on postoperative care, quality oflife, and future preference.
Secondary outcomes included barriers such as phone/internet connectivity, missed appointments, and the difference between self-assessment and physical examination, while facilitators like psychological/social support, time and money saved in travel were also considered. Robustness was measured by the quality of audio/ video, call drops, time lags, and power supply, while efficacy focused on safe and effective postoperative care, handling minor health issues, Modified QoR-15 scores, and return to physical activity. Safety was assessed by postoperative morbidity (fever, pain, surgical site infections, haemorrhage, unscheduled visits, readmissions), and acceptability was measured by satisfaction with the model, adherence to schedule, and cost of service.
Data Management and Analysis
Data related to primary and secondary outcomes were collected using a structured pretested proforma, with one form used for each virtual session. The data was analysed using SPSS 20.0, with results for primary and secondary outcomes presented in both tabular and graphic formats. Satisfaction scores for both the provider and recipient were assessed using Likert scales and presented as mean, standard deviation, and percentage. Postoperative recovery (Modified QoR-15) scores are also presented in similar formats. Responses to open-ended questions were analysed using thematic analysis.
Results
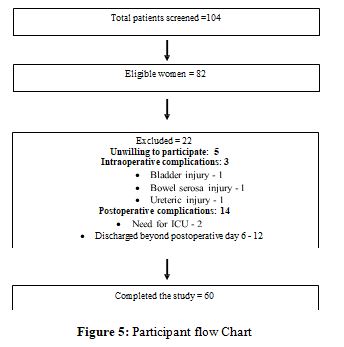
A total of 104 patient undergoing gynaecological surgery were screened for eligibility out of which 82 were found eligible for the study however 22 had to be excluded due to meeting one or more exclusion criteria (unwilling to participate, intra and postoperative complications). Finally, 60 eligible women were recruited and completed the study.
Most participants were urban residents (71.7%), homemakers (90%), with an average age of 39.08 years. The mean BMI was 25.05 kg/m.2, with over 50% classified as overweight. Common procedures included abdominal hysterectomy (21.67%) and vaginal hysterectomy (18.33%). Most patients (78.3%) were discharged within five days post-surgery (Table 2).
|
Characteristics |
Study population (n=60) No. (%) |
|
|
Maternal Age (years) mean±SD |
39.08 ± 10.31 |
|
|
Maternal Age |
|
|
|
<20 |
01 |
01.70 |
|
20-30 |
12 |
20.00 |
|
31-50 |
42 |
70.00 |
|
>50 |
05 |
08.30 |
|
Religion |
||
|
Hindu |
41 |
68.30 |
|
Muslim |
17 |
28.30 |
|
Others |
02 |
03.40 |
|
Residence |
||
|
Rural |
17 |
28.30 |
|
Urban |
43 |
71.70 |
|
Socio-economic status |
||
|
Upper Lower |
04 |
06.70 |
|
Lower Middle |
23 |
38.30 |
|
Upper Middle |
33 |
55.00 |
|
Education |
||
|
Illiterate |
12 |
20.00 |
|
Primary |
08 |
13.30 |
|
Secondary |
29 |
48.30 |
|
Higher Secondary |
06 |
10.00 |
|
Graduate & Beyond |
05 |
08.40 |
|
Occupation |
||
|
Homemaker |
54 |
90.00 |
|
Others |
06 |
10.00 |
|
Distance from health facility (Kilometres) |
||
|
<5 |
19 |
31.67 |
|
5-10 |
25 |
41.67 |
|
10-50 |
12 |
20.00 |
|
>50 |
04 |
06.66 |
|
Mode of transport |
||
|
Public |
48 |
80.00 |
|
Private |
12 |
20.00 |
|
BMI (kg/m2) Mean±SD) |
25.05 ±3.16 |
|
|
BMI |
||
|
<18.5 |
04 |
06.67 |
|
18.5-24.9 |
21 |
35.00 |
|
25-29.9 |
32 |
53.33 |
|
30-34.9 |
03 |
05.00 |
|
35-39.9 |
00 |
00.00 |
|
Cyst Excision with Vaginal Cyst Excision |
||
|
Diagnostic Hystero- laparoscopy |
09 |
15.00 |
|
Exploratory Laparotomy |
02 |
03.33 |
|
Hysteroscopy |
05 |
08.33 |
|
Hysterectomy with or without salpingectomy
|
13 04 11 |
21.67 06.67 18.33 |
|
Cystectomy-
|
06 02 |
10.00 03.33 |
|
Abdominal Myomectomy |
07 |
11.67 |
|
Cyst excision |
01 |
01.67 |
|
Type of Anaesthesia |
||
|
General |
14 |
23.30 |
|
Spinal |
10 |
16.70 |
|
Combined spinal-epidural |
34 |
56.70 |
|
Saddle |
02 |
03.30 |
|
Postoperative day of discharge |
||
|
<3 |
18 |
30.00 |
|
3-5 |
29 |
48.30 |
|
6 |
13 |
21.70 |
Table 2: Sociodemographic, Clinical and Surgical Characteristics of the Study Population (n=60)
Patients successfully completed an average of 3 virtual visits (mean time: 7.2 minutes for the first visit, reducing to 4.16 minutes by the third) and 1 physical visit.
There were no unscheduled visits. Providers rated their satisfaction with telehealth highly, with mean scores across visits for effective clinical decision-making (4.90/5), safety of virtual visits (4.93/5), and satisfaction with the technology (4.78/5). Overall satisfaction for physical visits was (4.81/5) (Table 3).
|
S. No. |
Question |
Satisfaction score (out of 5) |
||
|
Virtual Visit I |
II |
III |
||
|
Mean± SD |
Mean± SD |
Mean± SD |
||
|
1 |
The telemedicine technology was adequate to conduct today’s visit. |
4.73 ± 0.44 |
4.95 ± 0.22 |
4.78 ± 0.42 |
|
2 |
Clinical decision making was successfully accomplished in virtual visit. |
4.82 ± 0.39 |
4.90 ± 0.30 |
4.93 ± 0.25 |
|
3 |
I am satisfied with today’s virtual visit. |
4.75 ± 0.47 |
4.85 ± 0.36 |
4.82 ± 0.39 |
|
4 |
I had technical issues with virtual visits. |
0.65 ± 0.88 |
0.65 ± 0.73 |
0.47 ± 0.77 |
|
5 |
Virtual visits improve access to health services. |
4.73 ± 0.44 |
4.82 ± 0.39 |
4.93 ± 0.25 |
|
6 |
It is easy to do virtual visits. |
4.92 ± 0.27 |
4.78 ± 0.42 |
4.85 ± 0.36 |
|
7 |
I think the virtual visits are safe for patients. |
4.87 ± 0.34 |
4.57 ± 0.50 |
4.93 ± 0.25 |
|
8 |
I think virtual visits are a positive change for patients. |
4.95 ± 0.22 |
4.48 ± 0.50 |
4.87 ± 0.34 |
|
Physical visit |
||||
|
S. No. |
Question |
Satisfaction score (out of 5) |
||
|
Mean±SD |
||||
|
1 |
Clinical decision making was successfully accomplished in physical visit |
4.81±0.39 |
||
|
2 |
I am satisfied with today’s physical visit. |
4.81±0.39 |
||
|
3 |
I think the virtual visits are safe for patients. |
4.81±0.39 |
||
|
4 |
It is easier than virtual visits. |
4.78±0.41 |
||
|
5 |
I would like to follow up patients through virtual visit in future. |
4.83±0.37 |
||
Table 3: Healthcare Provider’s Perspective - Satisfaction Scores after Virtual Visits & Physical visit at end of Follow-up
Patient satisfaction steadily increased across virtual visits, with overall satisfaction scores of (4.48/5), (4.75/5), and (4.80/5) for the first, second, and third visits, respectively. Comfort in connecting with the doctor improved from (4.37/5) to (4.75/5), and understanding of the telehealth model rose from (4.45/5) to (4.98/5). After the physical visit, overall satisfaction was (4.81/5). 13.33% of patients experienced complications, all of which were successfully managed.
|
S. No. |
Question |
Satisfaction score (out of 5) |
||
|
Virtual Visit I |
II |
III |
||
|
Mean± SD |
Mean± SD |
Mean± SD |
||
|
1 |
I am satisfied with the care I have received. |
4.48 ± 0.50 |
4.75 ± 0.43 |
4.80 ± 0.40 |
|
2 |
I will recommend this service to my friends. |
4.43 ± 0.50 |
4.73 ± 0.44 |
4.73 ± 0.44 |
|
3 |
I feel comfortable connecting with the doctor. |
4.37 ± 0.49 |
4.70 ± 0.49 |
4.75 ± 0.43 |
|
4 |
I had technical issues with virtual visits. |
0.70 ± 0.72 |
0.75 ± 0.77 |
0.92 ± 0.94 |
|
5 |
I am getting the postoperative care that I need. |
4.52 ± 0.50 |
4.68 ± 0.46 |
4.85 ± 0.36 |
|
6 |
I was able to express myself effectively. |
4.60± 0.49 |
4.55 ± 0.50 |
4.45 ± 0.67 |
|
7 |
I feel comfortable sharing my data with my healthcare provider during virtual visits. |
4.48 ± 0.50 |
4.52 ± 0.50 |
4.62 ± 0.55 |
|
8 |
I am able to contact my healthcare provider in case of need and emergency. |
4.63 ± 0.49 |
4.77 ± 0.42 |
4.90 ± 0.30 |
|
9 |
I am able to understand the Tele Postop care model. |
4.45 ± 0.5 |
4.83 ± 0.37 |
4.98 ± 0.12 |
|
Physical visit |
||||
|
S. No. |
Question |
Mean±SD (Out of 5) |
||
|
1 |
I am satisfied with the care I have received. |
4.81 ± 0.43 |
||
|
2 |
I will recommend this service to my friends. |
4.76 ± 0.53 |
||
|
3 |
I feel comfortable connecting with the doctor. |
4.61 ± 0.49 |
||
|
4 |
I am getting the postoperative care that I need. |
4.75 ± 0.47 |
||
|
5 |
I was able to express myself effectively. |
4.70 ± 0.61 |
||
|
6 |
I am able to understand the tele post op care model. |
4.90 ± 0.30 |
||
|
7 |
I would opt Tele postop care model in future. |
4.48 ± 0.74 |
||
Table 4: Patient Satisfaction Scores after Virtual Visits and Physical visit at end of Follow-up
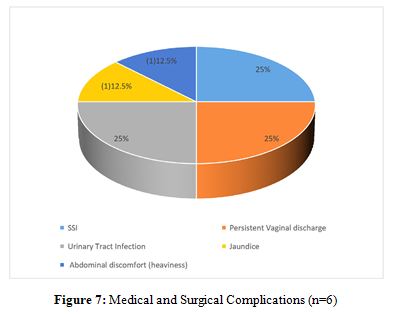
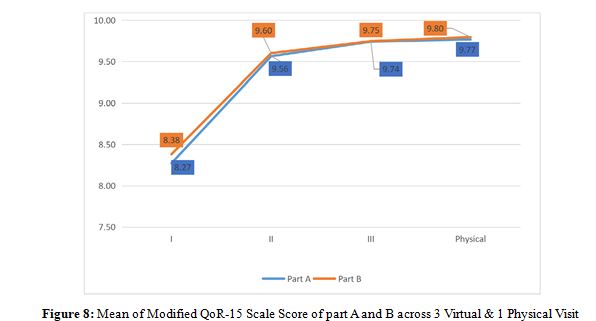
Only two patients required readmission for management of urinary tract infection and jaundice. Scores improved significantly across visits. These scores reflect enhanced physical and emotional recovery through telehealth follow-ups. Average score across part A and B of questionnaire increased from (8.38/10,8.27/10) for first virtual visit to (9.80/10,9.77/10) at physical visit.
|
Part A (Scored out of 10) 0 to 10, where: 0 = none of the time [excellent] and 10 = all of the time [poor] |
||||
|
Question |
Virtual Visit I |
II |
III |
Physical Visit |
|
Mean±SD |
Mean±SD |
Mean±SD |
Mean±SD |
|
|
1. Able to breathe easily |
8.74 ± 0.45 |
9.67 ± 0.48 |
9.87 ± 0.35 |
9.89 ± 0.33 |
|
2. Able to enjoy food |
8.14 ± 0.84 |
9.50 ± 0.51 |
9.64 ± 0.49 |
9.70 ± 0.47 |
|
3. Feeling rested |
7.92 ± 0.75 |
9.47 ± 0.51 |
9.74 ± 0.45 |
9.79 ± 0.42 |
|
4. Have had a good sleep |
7.92 ± 0.79 |
9.37 ± 0.49 |
9.57 ± 0.5 |
9.54 ± 0.51 |
|
5. Able to look after personal toilet and hygiene unaided |
8.24 ± 0.79 |
9.65 ± 0.49 |
9.84 ± 0.38 |
9.87 ± 0.35 |
|
6. Able to communicate with family or friends |
8.79 ± 0.83 |
9.62 ± 0.5 |
9.74 ± 0.45 |
9.75 ± 0.44 |
|
7. Getting support from hospital doctors and nurses |
8.90 ± 0.88 |
9.64 ± 0.49 |
9.74 ± 0.45 |
9.74 ± 0.45 |
|
8. Able to return to work or usual home activities |
8.04 ± 0.89 |
9.55 ± 0.51 |
9.87 ± 0.35 |
9.89 ± 0.33 |
|
9. Feeling comfortable and in control |
8.05 ± 0.77 |
9.60 ± 0.50 |
9.75 ± 0.44 |
9.82 ± 0.4 |
|
10. Having a feeling of general well-being |
8.04 ± 0.79 |
9.59 ± 0.50 |
9.70 ± 0.47 |
9.72 ± 0.46 |
|
Part B (Scored out of 10) 10 to 0, where: 10 = none of the time [excellent] and 0 = all of the time [poor] |
||||
|
Question |
I |
II |
III |
Physical |
|
Mean |
Mean |
Mean |
Mean |
|
|
11. Moderate pain |
7.84 ± 0.77 |
9.50 ± 0.51 |
9.80 ± 0.41 |
9.95 ± 0.22 |
|
12. Severe pain |
8.42 ± 0.68 |
9.65 ± 0.49 |
9.92 ± 0.28 |
9.90± 0.31 |
|
13. Nausea or vomiting |
8.90 ± 0.71 |
9.64 ± 0.49 |
9.87 ± 0.35 |
9.77 ± 0.43 |
|
14. Feeling worried or anxious |
7.99 ± 0.80 |
9.59 ± 0.5 |
9.64 ± 0.49 |
9.67 ± 0.48 |
|
15. Feeling sad or depressed |
8.15 ± 0.78 |
9.45 ± 0.51 |
9.44 ± 0.5 |
9.54 ± 0.51 |
|
16. Fever |
9.37 ± 0.79 |
9.80 ± 0.41 |
9.72 ± 0.46 |
9.85 ± 0.37 |
|
17. Bleeding per vaginum |
8.02 ± 0.80 |
9.60 ± 0.5 |
9.85 ± 0.37 |
9.90± 0.31 |
Table 5: Modified QoR-15 Scale Score After I,II,III ( Virtual Visit ) & Physical Visit
Adherence to scheduled visits was excellent (93.3%), with high-quality audio/video reported in 88.3% of cases.
|
Phone/Internet Connectivity |
No. |
Percentage |
|
Excellent |
56 |
93.30 |
|
Average |
04 |
06.70 |
|
Missed appointments |
||
|
None |
57 |
95.00 |
|
1 |
03 |
05.00 |
|
Adherence to schedule |
||
|
Excellent |
56 |
93.30 |
|
Poor |
04 |
06.70 |
Table 6: Facilitators and Barriers to Implementation of Tele-Health Postoperative Follow-up Care Model. (n=60) Psychological and social support at home was universally present (100%).
|
Psychological and social support |
No. |
Percentage |
|
Present |
60 |
100 |
Table 7: Psychological and Social Support at Home (n=60)
Minor issues included call drops (6.7%) and time lags (13.3%), which were infrequent and did not significantly affect satisfaction.
|
Robustness of the process |
No. |
Percentage |
|
Quality of Audio/Video Calls |
||
|
Excellent |
53 |
88.30 |
|
Poor |
07 |
11.70 |
|
Time Lag |
||
|
Present |
08 |
13.30 |
|
Absent |
52 |
86.70 |
|
Power supply |
||
|
Uninterrupted |
55 |
91.70 |
|
Interrupted |
05 |
08.30 |
|
No. of call drops (Mean ± SD) |
1.8 ± 1.2 |
|
|
No. of call drops |
||
|
None |
55 |
91.60 |
|
1 |
04 |
06.70 |
|
2 |
01 |
01.70 |
Table 8: Components of the Robustness of Process. (n=60)
88.3% of patients expressed a preference for telehealth in future follow-ups. Most participants reported high levels of trust and ease in sharing their data (4.62/5) and felt confident accessing healthcare in emergencies (4.90/5). The model was characterized by high patient and provider satisfaction, improved accessibility, and significant time and cost savings, making it a promising approach to postoperative care in low resource setting.
Discussion
This single-centre, prospective study examined the feasibility of using telemedicine for postoperative follow-up care after major elective gynaecological surgery in a low-resource tertiary care hospital. The tele-health model was effective in providing timely, cost-efficient, and accessible care without compromising clinical outcomes. While many studies have explored telemedicine in various surgical fields like gastrointestinal, cardiothoracic, urology, oncology, and orthopaedics, its application in postoperative gynaecology remains underexplored, especially in low- and middle-income countries (LMICs) like India [5-9].
Our findings are consistent with previous research. Van Noordegraaf et al. showed that eHealth interventions enhanced recovery and reduced time to return to work following gynaecological surgeries [10]. Similarly, Sharmila V et al., Sharma B et al. reported that mobile-based tele-consultation effectively reduced in-person visits while ensuring high patient satisfaction [10,11]. In this study, telemedicine saved an average of 205 minutes and â?¹343 per patient, in line with findings from Gunter et al. and Sorwar et al [12,13].
The duration of virtual consultations decreased over time, from an average of 7.2 minutes in the first session to 4.16 minutes in the third, reflecting improved efficiency and familiarity with telemedicine among both patients and providers. This aligns with Radtke et al. and Mezes et al., who reported similar efficiency improvements in telemedicine interactions [14,15]. Additionally, no increase in postoperative morbidity or readmissions was observed, supporting findings that telemedicine outcomes are comparable to traditional care [16].
Despite low resource setting, only 7% of participants reported issues like call drops or time lags, demonstrating the robustness of the tele-health model. Moreover, nearly all patients had adequate psychological and social support at home, further reinforcing the suitability of telemedicine as a complementary approach to in-person care. Patient understanding and satisfaction with the tele-health model increased significantly, with 98% expressing confidence in the process by the third visit. Over 85% of participants were satisfied with their care and endorsed telemedicine as a preferred option for future follow-ups.
Strength and Limitations
This study confirms that telemedicine can be a feasible and effective model for postoperative gynaecological care in low-resource settings. Future research should focus on expanding the model to other types of gynaecological surgeries, addressing technical challenges, and enhancing digital infrastructure and literacy in LMICs to optimize the benefits of telemedicine in postoperative surgical care.
Conclusion
This study demonstrates the potential of telemedicine to reduce health inequities in women’s and reproductive health, particularly in low-resource settings. By evaluating its feasibility for postoperative follow-up care after major gynaecological surgeries, the research highlights telemedicine’s ability to overcome barriers such as limited access, financial constraints, and logistical challenges. The study confirms that telemedicine is a safe, effective, and scalable solution, offering reduced costs, early detection of complications, and enhanced patient satisfaction. It provides a foundation for future research and standardized protocols. In conclusion, telemedicine offers a transformative, equitable, and patient-centred approach to improving women’s health outcomes
Disclosure of Interest
The authors declare no conflicts of interest related to this study.
Contribution to Authorship
AC and KG conceptualized the study, designed the methodology, and led the data collection process, data analysis and drafted the manuscript. AMK supervised the entire research process, ensuring adherence to scientific & ethical standards and provided critical revisions. RS and AS helped in data collection. All authors have read and approved the final manuscript and take responsibility for its accuracy and integrity.
Details of Ethics Approval
Approval was obtained from the Institutional Ethics Committee- Human Resource (IEC-HR) (Ethics approval number- IECHR-2023-59-88) of University College of Medical Sciences, India.
References
1. Williams, A. M., Bhatti, U. F., Alam, H. B., & Nikolian, V. C. (2018). The role of telemedicine in postoperative care. Mhealth, 4, 11.
2. Board of Governors - In supersession of the Medical Council of India. Telemedicine Practice Guidelines: Enabling Registered Medical Practitioners to Provide Healthcare Using Telemedicine. 2020. Available from https://www.mohfw.gov. in/pdf/Telemedicine.pdf. Accessed on 14th February 2025.
3. Ferrari-Light, D., Geraci, T. C., Chang, S. H., & Cerfolio, R. J. (2020). Novel pre-and postoperative care using telemedicine. Frontiers in Surgery, 7, 596970.
4. Clavien, P. A., Barkun, J., De Oliveira, M. L., Vauthey, J. N., Dindo, D., Schulick, R. D., ... & Makuuchi, M. (2009). The Clavien-Dindo classification of surgical complications: five- year experience. Annals of surgery, 250(2), 187-196.
5. Wang, H., Hu, W., Ma, L., & Zhang, Y. (2019). Digital chest drainage system versus traditional chest drainage system after pulmonary resection: a systematic review and meta- analysis. Journal of cardiothoracic surgery, 14, 1-6.
6. Socarrás, M. R., Loeb, S., Teoh, J. Y. C., Ribal, M. J., Bloemberg, J., Catto, J., ... & Rivas, J. G. (2020). Telemedicine and smart working: recommendations of the European Association of Urology. European urology, 78(6), 812-819.
7. Deo, S. V., Pramanik, R., Chaturvedi, M., Nath, A., Ghosh, J., Das Majumdar, S. K., ... & Mathur, P. (2022). Telemedicine and cancer care in India: promises, opportunities and caveats. Future Science OA, 8(9), FSO821.
8. Fahey, E., Elsheikh, M. F., Davey, M. S., Rowan, F., Cassidy, J. T., & Cleary, M. S. (2022). Telemedicine in orthopedic surgery: a systematic review of current evidence. Telemedicine and e-Health, 28(5), 613-635.
9. Vonk Noordegraaf, A., Anema, J. R., Van Mechelen, W., Knol, D. L., Van Baal, W. M., Van Kesteren, P. J. M., ... & Huirne, J. A. F. (2014). A personalised e H ealth programme reduces the duration until return to work after gynaecological surgery: results of a multicentre randomised trial. BJOG: An International Journal of Obstetrics & Gynaecology, 121(9), 1127-1136.
10. Sharmila, V., Yedla, D., Babu, T. A., Tripathi, M., & Kalidoss, V. K. (2023). Utility of telemedicine for providing Obstetrics and Gynecology services during the COVID-19 pandemic—A single center experience from a tertiary care teaching hospital located in South India. Journal of Education and Health Promotion, 12(1), 406.
11. Sharma, B., Rohilla, M., Suri, V., Jain, V., Prasad, G. R. V., Kalra, J., & Pandey, N. (2023). Obstetric teleconsultation by using mobile phone technology in COVID pandemic. Indian Journal of Community Medicine, 48(1), 190-195.
12. Gunter, R. L., Fernandes-Taylor, S., Rahman, S., Awoyinka, L., Bennett, K. M., Weber, S. M., ... & Kent, K. C. (2018).
Feasibility of an image-based mobile health protocol for postoperative wound monitoring. Journal of the American College of Surgeons, 226(3), 277-286.
13. Sorwar, G., Rahamn, M. M., Uddin, R., & Hoque, M. R. (2016). Cost and time effectiveness analysis of a telemedicine service in Bangladesh. In The promise of new technologies in an age of new health challenges (pp. 127-134). IOS Press.
14. Radtke, S., Umeh, R., Chavez, M., Curiel, Z., & Mendez, K. (2021). Utilizing telemedicine for delivery of postoperative care following minimally invasive gynecologic surgery: a randomized controlled trial. Gynecology and Minimally Invasive Therapy, 10(3), 148-153.
15. Mezes, C., Klebanoff, J. S., Grebenyuk, E., Gobern, J., Meske, S. W., Amdur, R., & Moawad, G. N. (2022). Virtual postoperative visits following robotic gynecologic surgery: a study of patient satisfaction, safety, and feasibility. Journal of robotic surgery, 16(5), 1193-1198.
16. Bouwsma, E. V., Bosmans, J. E., van Dongen, J. M., Brölmann, H. A., Anema, J. R., & Huirne, J. A. (2018). Cost-effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: economic evaluation alongside a stepped-wedge cluster-randomised trial. BMJ open, 8(1), e017782.