



Case Report - (2025) Volume 10, Issue 3
Surgery of Cardiac Papillary Fibroelastoma: Case Report
Received Date: Oct 27, 2025 / Accepted Date: Dec 01, 2025 / Published Date: Dec 10, 2025
Copyright: ©©2025 Lakehal Redha. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Redha, L. (2025). Surgery of Cardiac Papillary Fibroelastoma: Case Report. Cardio Open, 10(3), 01-05.
Abstract
Cardiac papillary fibroelastoma is very rare and benign primitive tumor, usually involving heart valves. It becomes serious illnesses when associated with clinical events, as systemic embolism. Currently, the diagnosis is easily evoked by echocardiography. Surgical excision of this tumor is a safe and effective treatment to prevent the risks of embolic repetition. We report on a 69 year-old woman suffering from a non-coronary aortic cusp fibroelastoma attached to the non-coronary aortic discovered by chance. Echocardiography detected tumor, sessile and mobile, attached to the non-coronary aortic cusp. The tumor was surgically excised. The histological examination confirmed the diagnosis of aortic papillary fibroelastoma. The clinical course was uneventful and no recurrence was observed.
Keywords
Papillary Fibroelastoma, Echocardiography, Cardiac Surgery
Introduction
Cardiac papillary fibroelastoma is a very rare benign cardiac tumor, predominantly located in the valvular region (80% of cases) and representing less than 10% of cardiac neoplasms. Sometimes asymptomatic, it can cause serious embolic events. Currently, the diagnosis is easily established by echocardiography. The most frequently reported clinical manifestation in the literature is the occurrence of ischemic strokes. Cardiac imaging provides easier access to diagnosis. Surgical excision remains the standard treatment with a low operative risk. The aim of this study is to present a case of aortic valve fibroelastoma.
Case Report
We report the case of a 69-year-old woman with no prior history of cardiac tumors discovered incidentally following chest pain. Functionally, she had NYHA stage I dyspnea. Chest X-ray revealed a cardiothoracic index (CTI) of 0.52.

Figure 1: Frontal Chest X-Ray
Electrocardiogram Showed Regular Sinus Rhythm
Transthoracic echocardiography (TTE) revealed a 10 mm mass attached to the aortic side of the non-coronary aortic cusp, highly mobile, suggesting aortic fibroblastoma. The left ventricle (LV) measured 45/29 mm + the ejection fraction was 66%.

Figure 2: Transthoracic Cardiac Ultrasound Appearance: Presence of an Echogenic, Pedunculated Tumor Mass, 10mm in Long Axis, Attached to the Non-Coronary Cusp (Arrow)
Transesophageal echocardiography (TEE) was performed to look for embolic heart disease. It confirmed the presence of a rounded, pedunculated, highly mobile formation, measuring 10 mm in diameter, attached to the aortic surface of the non-coronary aortic cusp (Figure 3). The examination was otherwise unremarkable, and the auricle was free of thrombus. The diagnosis of fibroelastoma was considered, and it was decided to perform preoperative coronary angiography to ensure the absence of significant coronary stenosis, which was the case. The image was highly suggestive of papillary aortic valve fibroelastoma, with an indication for surgery.

Figure 3: Transesophageal Echocardioraphy: Presence of a Tumor Mass Hanging on the Aortic Side of the Non-Coronary Aortic Cusp (Arrow)
The patient underwent surgery under cardiopulmonary bypass with the heart stopped after a vertical median sternotomy with left ventricular discharge via the right superior pulmonary vein. Intraoperative exploration revealed a yellowish mass measuring 1 cm long axis at the level of the non-coronary cusp with a macroscopic appearance (Figure 4) of a soft, translucent, vegetative tumor with a gelatinous appearance resembling, when in a liquid medium, a sea anemone.

Figure 4: Intraoperative Image before Resection of the Non-Coronary Cusp Mass
The procedure consisted of resection of this mass, which was sent for pathological study (Figure 5) with histological confirmation of the diagnosis of aortic non coronary cusp papillary fibroelastoma.
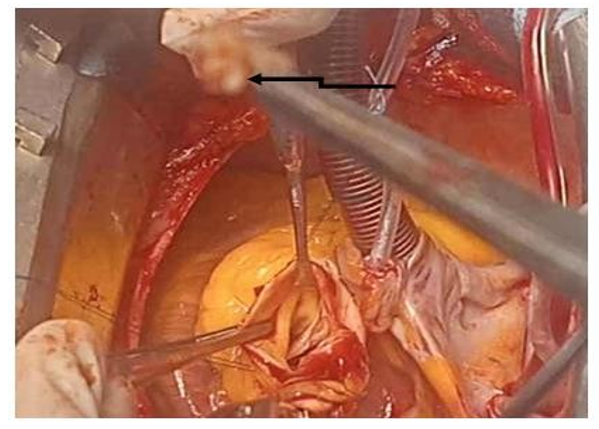
Figure 5: Intraoperative Image after Resection of the Non-Coronary Cusp Mass
Results
The durations of cardiopulmonary bypass, aortic cross-clamping, and circulatory support were 36, 22, and 6 minutes, respectively. The durations of ventilation, intensive care unit stay, and postoperative stay were 6 hours, 48 hours, and 8 days, respectively. The postoperative course was relatively uneventful. She was discharged on the 8th postoperative day with regular echocardiographic monitoring. Follow-up echocardiograms performed at the 1st, 3rd, 6th, and 9th months, and at one year, showed no recurrence of the cardiac mass.
Discussions
Primary valvular cardiac tumors are rare, representing 5 to 10% of cardiac tumors. In the general population, their incidence is 0.02%. Papillary fibroelastomas (PF) are the most common primary valvular tumors, constituting 70 to 90% of them [1]. Cardiac papillary fibroelastoma is a rare benign tumor, most often valvular, primarily aortic, as in our patient’s case, and mitral, occurring in middle-aged adults with a peak between 70 and 80 years of age. The sex ratio is approximately 1:1 [2]. Its usual size is around 10 mm but can vary between 2 and 70 mm (3.5). It is usually single, but multiple locations occur in 10% of cases (3.4). The possible locations of fibroelastomas are numerous and are typically located in the middle of the valve body, on both sides of the ventriculo- arterial and atrioventricular valves, on the chordae and the atrial and ventricular endocardium [3,4]. It readily inserts itself into the endocardium via a more or less long pedicle.
The pathogenesis is unknown, the cancerous, embryological or inflammatory origin has never been demonstrated, nor that of their development from mural thrombi [3]. There is no recognized risk factor for the occurrence of papillary fibroelastoma. The symptomatology linked to the embolic risk or the obstructive nature makes it serious: stroke (50%), acute coronary syndrome (20%) and more rarely mesenteric ischemia, pulmonary embolism for tumors located on the right, syncope, heart failure, sudden death [2,3,5,6]. However, it is asymptomatic in a third of cases as is the case in our patient [5]. In echocardiography, it presents as a mobile, rounded, irregular, pedunculated mass. Transesophageal echocardiography (TEE) is more sensitive and allows a precise analysis of the relationships of the tumor to adjacent cardiac structures [7].
The emboligenic potential is the clinical seriousness of this cardiac tumor: mainly cerebral embolism, but also coronary and systemic embolism; there is also a risk of heart failure, syncope, pulmonary embolism for tumors located on the right, and sudden death. Diagnosis is most often made during transthoracic and/or transesophageal echocardiography. CT angiography and cardiac MRI can also be useful examinations for a better diagnostic approach and for precise evaluation of the various anatomical relationships [8]. The positive diagnosis is pathological. The differential diagnoses of cardiac fibroelastoma are intracardiac thrombi, other tumors, benign or more rarely malignant, and vegetations. The clinical context, the evolution under anticoagulant and/or antibiotic treatment, and imaging data are necessary to suggest the diagnosis [5]. Surgical treatment must be prompt and routine in symptomatic forms to prevent embolic recurrences and, in the vast majority of cases, consists of simple tumor resection [9-11]. In its typical form, this cardiac tumor has a raspberry-like appearance, but the presence of multiple papillary extensions is at its origin in a liquid medium, reminiscent of a sea anemone [11]. The prognosis is excellent, and no subsequent recurrence has been described.
Conclusion
Cardiac fibroelastoma is a benign tumor that can cause serious and recurrent embolic complications. It is most often asymptomatic. A TEE is necessary for any unexplained embolic event in a patient in good general condition. Surgery allows for definitive cure. The postoperative prognosis is excellent.
References
- Gowda, R. M., Khan, I. A., Nair, C. K., Mehta, N. J., Vasavada,B. C., & Sacchi, T. J. (2003). Cardiac papillary fibroelastoma: A comprehensive analysis of 725 cases. American heart journal, 146(3), 404-410.
- Vagefi, P. A., Bates, N. R., Ptaszek, L. M., Adams, M. S., & Walker, J. D. (2006). Valve-sparing excision of aortic valve papillary fibroelastoma. The Journal of Thoracic and Cardiovascular Surgery, 131(5), 1177-1178.
- Ngaage, D. L., Mullany, C. J., Daly, R. C., Dearani, J. A.,Edwards, W. D., Tazelaar, H. D., ... & Zehr, K. J. (2005). Surgical treatment of cardiac papillary fibroelastoma: a single center experience with eighty-eight patients. The Annals of thoracic surgery, 80(5), 1712-1718.
- Rbaibi, A., BONNEVIE, L., GUIRAUDET, O., GODREUIL,C., MARTIN, D., & HAURET, L. (2002). Intérêt del’échocardiographie transœsophagienne et du scanner multicoupes dans la démarche diagnostique d’un cas de fibroélastome papillaire révélé par un accident neurologique. Archives des maladies du coeur et des vaisseaux, 95(6), 601- 605.
- Bottio, T., Pittarello, D., Bonato, R., Thiene, G., Gerosa, G., Casarotto, D., & Basso, C. (2004). Echocardiographic diagnosis of aortic valve papillary fibroelastoma. Texas Heart Institute Journal, 31(3), 322.
- Sun, J. P., Asher, C. R., Yang, X. S., Cheng, G. G., Scalia, G.M., Massed, A. G., ... & Thomas, J. D. (2001). Clinical and echocardiographic characteristics of papillary fibroelastomas: A retrospective and prospective study in 162 patients. Circulation, 103(22), 2687-2693.
- Rbaibi, A., Bonnevie, L., Guiraudet, O., Godreuil, C., Martin, D., Hauret, L., ... & Larroque, P. (2002). Importance of transesophageal echocardiography and computed tomography in the differential diagnosis of a case of papillary fibroelastomarevealed by a neurologic accident. Archives des Maladies du Coeur et des Vaisseaux, 95(6), 601-605.
- Arenaza, D. P. D., Pietrani, M., Moon, J. C., Rivello, H.G., Coccaro, N., Krauss, J., ... & Monaco, R. G. (2007). Cardiac fibroelastoma: cardiovascular magnetic resonance characteristics. Journal of Cardiovascular Magnetic Resonance, 9(3), 621-621.
- Grinda, J. M., Couetil, J. P., Chauvaud, S., D’Attellis, N., Berrebi, A., Fabiani, J. N., ... & Carpentier, A. (1999). Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization. The Journal of thoracic andcardiovascular surgery, 117(1), 106-110.
- TAZELAAR, H. D., LOCKE, T. J., & McGREGOR, C. G.(1992, October). Pathology of surgically excised primary cardiac tumors. In Mayo Clinic Proceedings (Vol. 67, No. 10, pp. 957-965). Elsevier.
- Grinda, J. M., Latremouille, C. H., Berrebi, A., Couetil, J. P., Chauvaud, S., Fabiani, J. N., ... & Carpentier, A. (2000). Cardiac fibroelastoma. Six operated cases and review of the literature. Archives des Maladies du Coeur et des Vaisseaux, 93(6), 727-732.