
Advances in Hematology and Oncology Research(AHOR)
ISSN: 2692-5516 | DOI: 10.33140/AHOR
Impact Factor: 1.2


Case Report - (2024) Volume 7, Issue 2
Successful Conservative Management of Warfarin-Induced Coagulopathy in an Elderly Male with Spontaneous Retroperitoneal Hematoma: A Case Report and Literature Review
22Student Research Committee, Shahrekord University of Medical Sciences, Shahrekord, Iran
Received Date: Sep 14, 2024 / Accepted Date: Oct 09, 2024 / Published Date: Oct 14, 2024
Copyright: ©Â©2024 Amirhossein Ghaedamini Asadabadi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Shams-Ghahfarokhi, S., Ghaedamini-Asadabadi, M., Ghaedamini-Asadabadi, A. (2024). Successful Conservative Management of Warfarin-Induced Coagulopathy in an Elderly Male with Spontaneous Retroperitoneal Hematoma: A Case Report and Literature Review. Adv Hema Onco Res, 7(2), 01-08.
Abstract
Spontaneous retroperitoneal hematoma is a rare complication of anticoagulant therapy that often requires aggressive treatment. We report the case of an elderly male with a history of Pulmonary Thromboembolism (PTE) who presented with cough and dyspnea and was treated for exacerbation of Chronic Obstructive Pulmonary Disease (COPD) and PTE. During his hospital stay, he developed a retroperitoneal hematoma as a complication of warfarin therapy. Despite the high risk of mortality and his advanced age, the patient was managed conservatively without the need for surgical intervention. With appropriate monitoring and supportive care, his hematoma resolved, and he was discharged in stable condition. This case underscores the potential for successful conservative management of warfarin-induced retroperitoneal hematomas in high-risk elderly patients.
Keywords
Anticoagulation, Retroperitoneal Hematoma, Elderly, Case Report, Warfarin, Conservative Therapy, Anticoagulants, Spontaneous Retroperitoneal Hematoma Categories: Pharmacology, Internal Medicine, Hematology
Introduction
Warfarin is an anticoagulant often used for the prevention of venous thromboembolism and its progression [1,2]. In elderly patients on anticoagulant therapy, bleeding complications are estimated to occur in about 5% of cases, with an incidence of Spontaneous Retroperitoneal Hematoma (SRH) at 0.6% [1,3]. Warfarin- induced hemorrhages can include gastrointestinal and intracranial bleeding, as well as renal, sublingual, and retrobulbar hematomas [1]. Patients with SRH typically require aggressive treatment, including blood transfusions, interventional radiological procedures, percutaneous drainage, or surgical evacuation of the hematoma [4]. We report a case of an 84-year-old man with a past medical history of COPD and PTE who was on anticoagulant therapy due to a previous PTE, which induced a retroperitoneal hematoma that spread to other organs. Despite the low rate of successful treatment reported in the literature and our limited therapeutic options, the hematoma resolved after conservative treatment, and the patient was discharged. This case report was prepared following the CARE guidelines [5].
Case Presentation
Narrative
Patient Information
An 84-year-old Iranian male farmer from Shahrekord presented to the emergency department with worsening dyspnea over the past 4 days. The dyspnea had progressively worsened and was exacerbated by physical activity. He also reported a productive cough with yellow to green phlegm and retrosternal chest pain radiating to his arm. His medical history included a 20-year history of COPD, 10 years of hypertension, and a pulmonary thromboembolism 4 years prior to presentation. Additionally, 5 years ago, he was diagnosed with ischemic heart disease, for which he underwent percutaneous coronary intervention with stent placement, leading to the revascularization of two vessels. The patient also has a significant smoking history, with a 30-pack-year smoking habit.
Clinical Findings
Based on physical examination findings, the patient was observed to be slim and cachectic, with a body temperature of 38.5°C. Tachycardia and mild tachypnea were noted, and his blood pressure was 110/70mmHg. Pulmonary auscultation revealed wheezing and coarse crackles at the bases of both lungs, which were more pronounced during expiration. A 2/6 systolic murmur was heard at the apex of the mitral valve. Oxygen saturation on room air was 85%, improving to 92% with supplemental oxygen administered via a nasal cannula. The patient reported mild epigastric pain, although there were no signs of guarding or rigidity. Additionally, no edema or size differences were observed in the extremities.
Diagnostic Assessment
Diagnostic Methods
In the laboratory evaluation, tests were conducted including Complete Blood Count (CBC), Blood Urea Nitrogen (BUN), creatinine, sodium, potassium, Prothrombin Time (PT), Partial Thromboplastin Time (PTT), International Normalized Ratio (INR), C-Reactive Protein (CRP), Erythrocyte Sedimentation Rate (ESR), troponin, White Blood Cell Differential (WBC diff), platelet count, urinalysis, and urine culture. The INR was 1.4. In the imaging evaluation, a High-Resolution Computed Tomography (HRCT) scan of the lungs was performed, revealing centrilobular emphysema in both lungs, consolidation at the base of the right lung, and ground-glass opacity at the base of the left lung (Figures 1 and 2).

HRCT: High-Resolution Computed Tomography
Figure 1: The HRCT Scan Shows Multiple Emphysematous Bullae, which are Air-Filled Spaces Resulting from the Destruction of Alveolar Walls, commonly seen in Emphysema
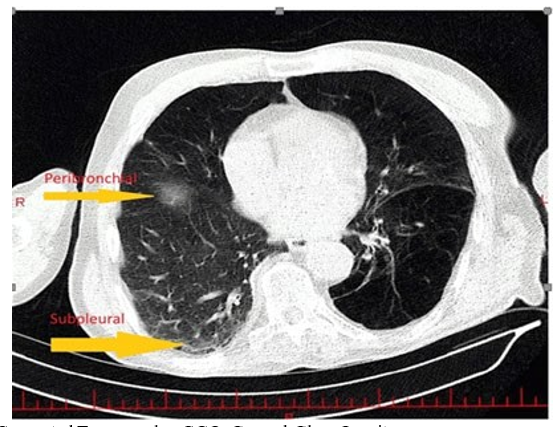
HRCT: High-Resolution Computed Tomography, GGO: Ground-Glass OpacityFigure 2: The HRCT Scan Shows Areas of GGO Located in the Subpleural and Peribronchial Regions. These GGOs indicate hazy areas of increased lung attenuation that may suggest inflammation, infection, or early fibrosis in these specific Lung Zones
Echocardiography (echo) revealed an ejection fraction of 50%, a pulmonary artery pressure of 40 mm Hg, and moderate mitral regurgitation, with no evidence of pericardial effusion (Table 1).
|
Type |
Value |
Unit |
Reference Range |
|
BUN |
30 |
mg/dl |
7-20 mg/dl |
|
Creatinine |
1.4 |
mg/dl |
0.6-1.2 mg/dl |
|
CRP |
30 |
mg/g |
<1 mg/dl |
|
D-dimer |
500 |
µg/L |
<500 µg/L |
|
ESR |
25 |
mm/1st hour |
0-20 mm/1st hour (men) |
|
Hb |
14 |
mg/dl |
13.8-17.2 mg/dl (men) |
|
Hct |
45 |
% |
40.7-50.3% (men) |
|
Neutrophils |
80 |
% |
40-60% |
|
Platelet count |
147,000 |
cells/mm³ |
150,000-450,000 cells/mm³ |
|
Troponin T |
0.2 |
ng/ml |
<0.01 ng/ml |
|
WBC |
12,000 |
cells/mm³ |
4,000-11,000 cells/mm³ |
|
BUN: Blood Urea Nitrogen, CRP: C-reactive Protein, ESR: Erythrocyte Sedimentation Rate, Hb: Hemoglobin, Hct: Hematocrit, WBC: Total White Blood Cells |
|||
Table 1: Diagnostics the Data were Collected when Patient was Admitted First Time
Diagnostic Reasoning
Based on the patient's history of smoking and a prior diagnosis of COPD with pneumonia, exacerbation of COPD remains the primary diagnosis. Differential diagnoses such as pulmonary thromboembolism was ruled out by negative D-dimer levels and the absence of characteristic findings on imaging. Additionally, Coronavirus Disease 2019 (COVID-19) and influenza were excluded based on negative polymerase chain reaction tests for both viruses. Decompensated heart failure was also considered but was ruled out due to a stable ejection fraction. Therefore, the clinical picture is consistent with an exacerbation of COPD, and the patient's symptoms and presentation align with this diagnosis.
Treatment and Prognosis
Following treatment for COPD exacerbation and pneumonia, the patient's anticoagulant regimen was adjusted based on a cardiology consultation, leading to an increased dosage of warfarin. However, after the diagnosis of a retroperitoneal hematoma, warfarin therapy was halted, and management was tailored according to the specifics outlined in Table 2.
Follow Up and Outcomes
The patient was treated for COPD exacerbation and pneumonia, resulting in a decrease in cough and phlegm; however, the chest pain persisted. During daily evaluations, an increase in troponin levels was noted, prompting a cardiology consultation. The consultation recommended initiating anticoagulation therapy to achieve an INR of 2-3 and performing coronary angiography once the patient's pulmonary status stabilized. After starting anticoagulants (heparin and warfarin), the patient developed abdominal pain in the periumbilical region that radiated to the back. The patient did not exhibit any signs of external hemorrhage, such as melena, hematemesis, rectorrhagia, hematuria, or hemoptysis, and an ultrasound of the abdomen and pelvis was normal. However, due to the persistence of pain and a 3 g/dL drop in hemoglobin, a CT scan with oral and IV contrast of the abdomen and pelvis was requested, which revealed a 110 x 180 mm retroperitoneal hematoma (Figure 3 and 4).

Figure 3: Retroperitoneal Hematoma in the Left Side
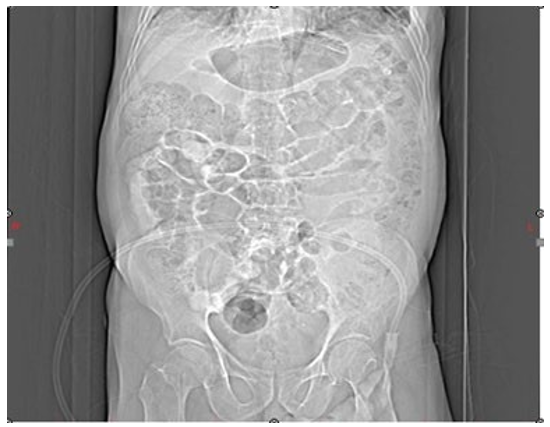
Figure 4: Abdominal Distension
A surgical consultation recommended ICU admission, correction of the coagulation disorder, and close observation. During observation, a superficial hematoma developed at the flank, extending to the testis. While hospitalized, the patient's creatinine level rose to 2.3 mg/dL, which improved after four days of conservative management and hydration. During ICU monitoring, Premature Ventricular Complexes (PVCs) and Premature Atrial Complexes (PACs) were detected. Upon ICU admission, the patient received treatment for anticoagulant complications as outlined in Table 2.
|
Treatment |
Type |
Administration (Dosage) |
Duration |
|
FFB |
Pharmacologic |
2 unites per 8 hours |
3 days |
|
Platelet |
Pharmacologic |
10 unites daily |
3 days |
|
Packed cell |
Pharmacologic |
2 unites daily |
3 days |
|
PCC |
Pharmacologic |
4 unites stat |
One Day |
|
Vit K |
Pharmacologic |
10 mg single dose |
One Day |
|
FFB: Fresh Frozen Blood, PCC: Prothrombin Complex Concentrate, Vit: Vitamin |
|||
Table 2: Treatment of Adverse Complications during Follow-Up
After stabilization of hemodynamics and hematoma size, the patient developed asymmetry in lower extremity size. A Doppler vein ultrasound revealed Deep Vein Thrombosis (DVT) in the distal lower extremities. Due to the presence of a hematoma and the contraindication to anticoagulation, an Inferior Vena Cava (IVC) filter was placed. On the fourth day of ICU admission, the patient experienced transient Atrial Fibrillation (AF), which resolved spontaneously. During follow-up, ultrasound reports indicated that the size of the retroperitoneal hematoma remained unchanged in the first few days of ICU admission but began to diminish after five days. After one week in the ICU, the patient was transferred to the internal medicine ward. Following ultrasound confirmation of hematoma organization, Apixaban was prescribed. Despite cardiology's recommendation for coronary angiography, the patient declined the procedure. The patient was discharged after 20 days, with significant improvement in cough and phlegm.
Discussion
SRH is a rare but potentially fatal complication of anticoagulants such as warfarin and heparin, presenting with a variety of clinical manifestations [1,6]. In this case, an 84-year-old male smoker with a medical history of hypertension, ischemic heart disease, pulmonary embolism, and COPD presented to the emergency department with cough, dyspnea, and chest pain. During his course of care, he developed an SRH that was managed with conservative therapy. Despite the patient's advanced age, comorbid conditions (including PTE and DVT), and high mortality risk, aggressive therapy limitations were respected, and he was successfully treated and discharged from the hospital. We conducted a literature search using PubMed, Google Scholar, Web of Science, and Trip databases with terms such as "retroperitoneal," "hematoma OR hemorrhage," and "warfarin." We identified seven case studies encompassing 12 cases (seven male and five female), aged between 21 to 82 years, showing a mortality rate of 41.6%. Among these, six cases involved warfarin administration, with a 33% mortality rate (Table 3).
|
Case study |
Gender |
Age |
Type of Anticoagulant |
Anticoagulant indication |
First Clinical Manifestation |
Site of Hematoma |
INR Level |
Hb |
History of Trauma |
Management |
Outcome |
|
1.Hashemi H et al [7] |
M |
40 |
Subcutaneous enoxaparin 80 mg bd |
Prophylactic due to COVID-19 hyper coagulable condition |
Right costal vertebral angle pain, hypotension and tachycardia |
Right costal vertebral angle pain, hypotension and tachycardia |
- |
9.5
g/dl |
- |
Anticoagulation therapy discontinued and received IV fluid and PBCs |
Discharged |
|
|
M |
Late80 s |
Warfarin 5g qd, aspirin 80 mg qd |
Ischemic stroke history and Prophylactic due to COVID-19 hyper coagulable condition |
- |
Right psoas muscle |
2.3 |
9.5 g/dl |
- |
Anticoagulation therapy discontinued and received IV fluid and PBCs |
Discharged |
|
|
F |
60 |
Intravenous heparin 1000 U/h |
Acute thrombosis in right radial vein |
Pitting edema on right upper limb |
Right psoas muscle |
|
9.5
g/dl |
|
Anticoagulation therapy discontinued and received IV fluid |
Discharged |
|
|
F |
Late 50s |
Subcutaneous enoxaparin 60 mg bd |
PTE |
hypotension |
Right psoas muscle |
|
8.9
g/dl |
|
Anticoagulation therapy discontinued and received IV fluid and PBCs |
Discharge |
|
|
M |
70 |
Subcutaneous enoxaparin 80 mg bd |
Prophylactic due to COVID-19 hyper coagulable condition |
Left flank and inguinal pain, hypotension and tachycardia |
Left iliopsoas muscle |
- |
7 |
- |
Anticoagulation therapy discontinued and received IV fluid, FFP and PBCs And angioembolization |
Discharged |
|
|
M |
70 |
Aspirin 80 mg qd, subcutaneous heparin 7500 tds |
Acute coronary syndrome and Prophylactic due to COVID-19 hyper coagulable condition |
Hypotension |
Right Psoas Muscle |
- |
fall |
- |
Anticoagulation therapy discontinued and received IV fluid, FFP and PBCs And angioembolization |
Discharged |
|
2. Hosseini M et al [1] |
M |
25 |
Warfarin |
Aortic Valva replacement |
Abdominal distention and low-grade fever with hypotension |
Diffuse bleeding around the left diaphragm and multiple nodular hemorrhage on the greater omentum |
2.4 |
- |
- |
Recusation Measures |
Death |
|
3.Tosun A et al [8] |
M |
21 |
Warfarin, 1 week |
Aortic and mitral valve replacement |
Groin pain radiated to left knee and a mass on right gluteal region |
Left iliac muscle |
5.47 |
11.8
g/dl |
- |
Anticoagulation therapy discontinued and received FFP and vitamin K |
Discharged |
|
4.Westergren T et al [9] |
F |
82 |
2.5 mg of warfarin daily. 4 weeks |
DVT and PTE |
- |
- |
>8 |
- |
- |
She was hospitalized and was given 5 mg of vitamin K orally |
Death |
|
5.Masamoto H et al [10] |
F |
39 |
She had been taking warfarin for 23 years. Thereafter, the medication was switched to heparin from 6 to 21 weeks of gestation. After this, she was prescribed oral warfarin again (3.5 mg/d) |
Mitral valve replacement |
Neurological deficit |
|
A strict control of PT/ INR |
- |
- |
She was hospitalized and was given 5 mg of vitamin K orally |
Death |
|
6. Lissoway J et al [6] |
F |
63 |
Initially, subcutaneous enoxaparin 80 mg every 12 hours in addition to warfarin 5 mg daily from day 2 |
A 24-h history of severe, non-exertional chest pain and new-onset paroxysmal atrial flutter without ST-segment elevation. |
Approximately 36 hours after admission, she became acutely hypotensive and developed tachycardia. |
- |
- |
- |
- |
She was transferred to the medical intensive care unit and intubated for respiratory arrest. Multiple rounds of standard advanced cardiac life support and infusion of blood products were performed. |
Death |
|
7. Jain et al [11] |
M |
66 |
M Unfractionated heparin 7000 IU |
Coronary angioplasty operation |
Hypotension |
Left psoas and iliacus muscle |
1.4 |
7.8 |
- |
Anticoagulation therapy discontinued and received IV fluid, FFP, PBCs Colloids and inotropes |
Death |
|
INR: International Ratio, PBCs: Packed Red Blood Cells, FFP: Fresh Frozen Plasma, DVT: Deep Vein Thrombosis, PTE: Pulmonary Thromboembolism, IU: International Unit, PT: Prothrombin Time, bd: Two Times a Day, tds: Three Times a Day, qds: Four Times a day. |
|||||||||||
Table 3: Review of Case Studies Including Clinical Manifestations, Type and Indication of Anticoagulants, Managements and Outcome
Hashemi et al., reported a series of 6 patients with COVID-19 and anticoagulant-induced retroperitoneal hematoma, where 4 patients recovered with conservative therapy involving IV fluids and blood transfusion, while 2 recovered through angioembolization [7]. Won et al. reported the treatment of a 48-year-old female on warfarin and aspirin, who required transcatheter atrial embolization after developing compartment syndrome due to SRH [12]. The usual signs and symptoms of SRH include abdominal distension, abdominal and back pain, a fall in Hemoglobin (Hb) and BP and peritoneal irritation [1,7]. Additionally, diffuse vasculopathy, atherosclerosis, and vasculitis of small vessels can result in the rupture of the most fragile vessels, causing diffuse bleeding [13]. The therapeutic window of warfarin is narrow, and anticoagulant treatment is easily influenced by concomitant conditions such as renal or hepatic disease, and medications including antibiotics, paracetamol, and simvastatin. Risk factors for SRH include age over 70 years and the use of oral anticoagulants and antiplatelets. It is crucial to carefully monitor Hb and BP, and consider SRH when these parameters fall [1,7].
Conclusion
Since an SRH may not be visible on ultrasound in the early days, its clinical diagnosis might be overlooked. Therefore, physicians should exercise increased vigilance in diagnosing SRH. Warfarin- induced SRH is a rare complication that can be effectively managed with conservative therapy, even in elderly patients with other comorbidities such as recent myocardial infarction, arrhythmias-including recurrent PVCs, PACs, AF and DVT due to discontinuation of anticoagulants and acute kidney injury on chronic kidney disease, without the need for aggressive or surgical interventions. A key highlight of our case report is that the patient’s recovery was achieved through meticulous monitoring and the administration of blood products, including fresh frozen plasma, packed red blood cells and prothrombin complex concentrate over several days.
Conclusion
Since an SRH may not be visible on ultrasound in the early days, its clinical diagnosis might be overlooked. Therefore, physicians should exercise increased vigilance in diagnosing SRH. Warfarin- induced SRH is a rare complication that can be effectively managed with conservative therapy, even in elderly patients with other comorbidities such as recent myocardial infarction, arrhythmias-including recurrent PVCs, PACs, AF and DVT due to discontinuation of anticoagulants and acute kidney injury on chronic kidney disease, without the need for aggressive or surgical interventions. A key highlight of our case report is that the patient’s recovery was achieved through meticulous monitoring and the administration of blood products, including fresh frozen plasma, packed red blood cells and prothrombin complex concentrate over several days.
Disclosures
Human Subjects: Consent was obtained or waived by all participants in this study. Ethics committee, Shahrekord university of Medical Sciences issued approval IR.SKUMS.REC.1403.049. this report was ethically approved by ethics committee of the Shahrekord university of Medical Sciences that followed all ethical aspects of ethics of research.
Conflicts of Interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following:
Payment/Services Info: All authors have declared that no financial support was received from any organization for the submitted work.
Financial Relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other Relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
- Hosseini, M., Hosseinzadeh, A., Raufian, K., & Hedjazi, A. (2015). Nontraumatic retroperitoneal hematoma after warfarin administration: fatal case report and review of the literature. The American journal of forensic medicine and pathology, 36(4), 245-248.
- Gilard-Pioc, S., Guerard, P., Paraf, F., & François-Purssell,I. (2017). Sudden death by spontaneous epiglottic hematoma secondary to high blood levels of warfarin. Journal of forensic sciences, 62(4), 1094-1096.
- López-Martínez, L., Molina-Nuevo, J. D., Pedrosa-Jiménez,M. J., & Juliá-Mollá, E. (2022). Spontaneous haematomas in anticoagulated COVID-19 patients: diagnosis and treatment by embolization. CardioVascular and Interventional Radiology, 45(7), 1001-1006.
- Nasr, M. A., Khallafalla, H., Kumar, V. R., & Pathan, S.A. (2019). Warfarin-induced spontaneous retroperitoneal hemorrhage from the renal vein: A rare case with an uncommon etiology. Qatar Medical Journal, 2019(1), 6.
- Gagnier, J. J., Kienle, G., Altman, D. G., Moher, D., Sox, H., & Riley, D. (2013). The CARE guidelines: consensus- based clinical case reporting guideline development. Global advances in health and medicine, 2(5), 38-43.
- Lissoway, J., & Booth, A. (2010). Fatal retroperitoneal hematoma after enoxaparin administration in a patient with paroxysmal atrial flutter. American Journal of Health-System Pharmacy, 67(10), 806-809.
- Hashemi, H., Moradi, H., Hashemi, M., Naderi, Z., & Jafarpisheh, S. (2022). Retroperitoneal hematoma in patients with COVID-19 infection during anticoagulant therapy: A case series and literature review. Journal of International Medical Research, 50(9), 03000605221119662.
- Tosun, A., Inal, E., Keles, I., Tulmaç, M., Tosun, Ö., Aydin, G., & Orkun, S. (2014). Conservative treatment of femoral neuropathy following retroperitoneal hemorrhage: a case report and review of literature. Blood Coagulation & Fibrinolysis, 25(7), 769-772.
- Westergren, T., Johansson, P., & Molden, E. (2007). Probable warfarin–simvastatin interaction. Annals of Pharmacotherapy, 41(7-8), 1292-1295.
- Masamoto, H., Uehara, H., Mekaru, K., Uezato, T., Sakumoto, K., & Aoki, Y. (2009). Warfarin-associated fetal intracranial hemorrhage in woman with mitral valve replacements: a case report. American journal of perinatology, 26(08), 597-600.
- Jain, A. K., Aggarwal, A., & Aggarwal, R. (2021). Spontaneous retroperitoneal haemorrhage post-coronary angioplasty: a case report. European Heart Journal-Case Reports, 5(2), ytab005.
- Won, D. Y., Kim, S. D., Park, S. C., Moon, I. S., & Kim,J. I. (2011). Abdominal compartment syndrome due to spontaneous retroperitoneal hemorrhage in a patient undergoing anticoagulation. Yonsei medical journal, 52(2), 358-361.
- Akuzawa, N., & Kurabayashi, M. (2018). Multiple spontaneous hemorrhages after commencing warfarin therapy. SAGE Open Medical Case Reports, 6, 2050313X18778380.