




Research Article - (2026) Volume 5, Issue 2
Study of Etiology and Outcomes of Operated Cases of Small Bowel Obstruction
Received Date: Feb 18, 2026 / Accepted Date: Mar 19, 2026 / Published Date: Apr 17, 2026
Copyright: ©2026 Helly Kothari, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kothari, H., Sachdeva, R. U. (2026). Study of Etiology And Outcomes of Operated Cases of Small Bowel Obstruction. J Surg Care, 5(2), 01-36.
Abstract
Background: Small bowel obstruction (SBO) is one of the most common surgical emergencies encountered in clinical practice and is associated with significant morbidity and mortality. It occurs due to mechanical or functional interruption in the normal passage of intestinal contents. The etiology of SBO varies widely and commonly includes postoperative adhesions, hernias, malignancies, volvulus, and inflammatory conditions. Early diagnosis and timely surgical intervention are essential to prevent complications such as bowel ischemia, necrosis, perforation, and sepsis. Understanding the etiological factors and evaluating postoperative outcomes can help improve management strategies and reduce complications.
Methods: A prospective observational study was conducted in the Department of General Surgery at a tertiary care center over a period of 30 months from December 2022 to July 2025. A total of 50 patients diagnosed with small bowel obstruction who underwent surgical management were included in the study. Diagnosis was established based on clinical examination and radiological investigations including abdominal X-ray and CT scan, while definitive confirmation was made intraoperatively. Data regarding demographic characteristics, clinical presentation, laboratory findings, imaging results, operative findings, surgical procedures performed, and postoperative outcomes were collected and analyzed.
Results: The majority of patients were above 60 years of age with a male predominance. The most common presenting symptoms were abdominal pain, vomiting, abdominal distension, and obstipation. Adhesions were identified as the most common cause of obstruction followed by hernias and malignancies. Surgical procedures performed included adhesiolysis, hernia repair, and bowel resection with anastomosis. Postoperative complications such as wound infection and prolonged hospital stay were observed in a minority of patients. Early surgical intervention was associated with improved outcomes and reduced complications.
Conclusion: Adhesions remain the most common etiological factor in surgically managed cases of small bowel obstruction. Early diagnosis, appropriate preoperative resuscitation, and timely surgical intervention significantly improve patient outcomes and reduce morbidity.
Keywords
Small Bowel Obstruction, Adhesions, Intestinal Obstruction, Surgical Management, Postoperative Outcomes
Introduction
Intestinal obstruction refers to a significant mechanical impairment or complete arrest in the passage of contents through the intestine. It is a serious condition that can result in a variety of symptoms, including cramping pain, vomiting, obstipation (severe constipation), and a lack of flatus (the inability to pass gas). These symptoms often lead to a considerable degree of distress for patients and, if left untreated, can result in serious complications. The diagnosis of intestinal obstruction is primarily clinical, based on the symptoms and physical examination findings. It is typically confirmed by abdominal x-rays, which can show the characteristic signs of bowel distention and air-fluid levels, helping to identify the level and cause of the obstruction [1].
Treatment of intestinal obstruction generally involves fluid resuscitation to address dehydration and electrolyte imbalances caused by vomiting and fluid loss. Nasogastric suction is often employed to decompress the stomach and relieve pressure on the intestine. This helps in alleviating symptoms like vomiting and abdominal distention. However, in cases of complete obstruction, particularly those caused by mechanical blockages, surgical intervention is often required to relieve the obstruction, correct any underlying anatomical issues, and prevent complications such as bowel necrosis or perforation [2].
Mechanical obstruction can occur at various levels of the digestive tract, and it is classified based on whether it affects the small bowel or large bowel. Obstruction of the small bowel, including the duodenum, is one of the most common types of mechanical bowel obstruction, whereas large bowel obstruction is less frequent but still presents significant challenges. The obstruction can be either partial or complete, depending on the extent to which the passage through the intestine is blocked. Partial small bowel obstructions are more likely to resolve with nonoperative treatment, with approximately 85% of these cases showing improvement without the need for surgery. On the other hand, complete small bowel obstructions, which are more severe, typically require surgical intervention to restore normal bowel function [2].
The etiology of intestinal obstruction is crucial in determining the probable outcomes and guiding treatment decisions. There are several potential causes of mechanical obstruction, and understanding the underlying etiology helps to predict the severity and potential complications of the condition. Common causes of small bowel obstruction include adhesions, hernias, and tumors. Adhesions, which are fibrous bands that form between bowel loops following surgery, are one of the most frequent causes of small bowel obstruction. Hernias, where a portion of the bowel protrudes through an opening in the abdominal wall, can also lead to bowel obstruction, especially when they become incarcerated or strangulated. Tumors, whether benign or malignant, can block the intestine either by direct invasion or by causing external compression of the bowel [3].
Other less common causes of small bowel obstruction include inflammatory conditions such as Crohn's disease, which can cause strictures and narrowing of the bowel, as well as volvulus, where a loop of intestine twists upon itself, cutting off the blood supply. Intussusception, a condition in which one part of the intestine telescopes into an adjacent part, can also lead to obstruction, particularly in children. In addition to these mechanical causes, there are also functional causes of obstruction, where there is a failure of normal bowel motility, as seen in conditions like pseudo-obstruction, which can occur in patients with conditions such as Parkinson's disease or after abdominal surgery [4].
The diagnosis of small bowel obstruction is based on the patient's clinical presentation, with confirmation provided by imaging studies such as abdominal x-rays or a computed tomography (CT) scan. Abdominal x-rays can reveal the characteristic features of bowel distention and air-fluid levels, which suggest the presence of an obstruction. A CT scan may be performed in more complicated or uncertain cases, as it provides more detailed information about the location, cause, and extent of the obstruction. In some cases, additional diagnostic procedures such as endoscopy or laparoscopy may be needed to identify the underlying cause of the obstruction, particularly when there is a suspicion of a tumor or other structural abnormality [5].
Treatment of small bowel obstruction is initially conservative, with a focus on fluid resuscitation, bowel decompression through nasogastric suction, and management of the underlying cause. Nonoperative management is effective in a significant proportion of cases, especially for partial obstructions caused by adhesions or hernias that are not strangulated. Conservative management involves careful monitoring of the patient's condition, management of pain, and correction of electrolyte imbalances. In patients with partial obstruction, if there is no evidence of strangulation or ischemia, spontaneous resolution of the obstruction may occur within a few days, and surgical intervention may be avoided [6].
In cases of complete small bowel obstruction, surgical intervention is often necessary. Surgery is typically indicated when there is evidence of bowel ischemia, strangulation, or perforation, as these complications can lead to life-threatening conditions such as peritonitis or sepsis. The surgical approach depends on the underlying cause of the obstruction. For example, if the obstruction is caused by adhesions, the surgeon may need to perform adhesiolysis to release the fibrous bands. In the case of a hernia, the surgeon may need to reduce the hernia and repair the defect in the abdominal wall. If the obstruction is caused by a tumor, surgical resection of the tumor may be necessary [7].
The prognosis of patients with small bowel obstruction depends on several factors, including the underlying etiology, the degree of bowel ischemia or necrosis, the patient's overall health, and the promptness of treatment. Patients with partial obstructions who are treated conservatively have a generally favorable prognosis, with most of these cases resolving without the need for surgery. However, patients with complete obstruction or those with complications such as strangulation, ischemia, or perforation have a more guarded prognosis. Early diagnosis and intervention are critical to improving outcomes and preventing serious complications [2].
In this study, we have reviewed our experience with small bowel obstruction and examined the common etiological factors and surgical management approaches at Sheth LG Hospital, Narendra Modi Medical College. Our findings highlight the importance of early diagnosis, appropriate management strategies, and the role of surgery in cases of complete obstruction. By analyzing the common causes of small bowel obstruction and evaluating the outcomes of surgical interventions, we aim to contribute to the current body of knowledge and provide insights into improving the management of this condition [1].
The study also emphasizes the need for continuous improvement in the understanding and management of small bowel obstruction. As new technologies and techniques in diagnosis and treatment continue to emerge, it is essential for clinicians to stay updated on the latest advancements in the field. In particular, the use of minimally invasive surgical techniques, such as laparoscopy, has shown promise in improving patient outcomes and reducing recovery times in patients with small bowel obstruction. Additionally, the identification and management of patients at high risk for complications, such as those with multiple comorbidities or a history of previous abdominal surgeries, are crucial in ensuring optimal care [8].
Small bowel obstruction is a serious medical condition that requires timely diagnosis and appropriate management. While conservative treatment may be effective in many cases, surgical intervention is often necessary for patients with complete obstruction or complications such as strangulation, ischemia, or perforation. By understanding the common causes and treatment strategies for small bowel obstruction, healthcare providers can better manage this condition and improve patient outcomes. Our study at Sheth LG Hospital provides valuable insights into the management of small bowel obstruction, and we hope that these findings will contribute to advancing knowledge and improving clinical practice in this area [9].
Aims and Objectives
1. To study various causes and factors responsible of small bowel Obstruction
2. To study indications of surgical management in case of small bowel Obstruction
3. To study surgical procedures and it's outcome in relation to etiological factors in small bowel Obstruction.
Review of Literature
Historical Review
• Treatment of acute intestinal obstruction dates back centuries. Ancient Egyptians recognized conditions like strangulated hernia and intussusception.
• Fabricus d'Aquopendente (12th century) described end-to-end anastomosis for intestinal repair.
• Ambroise Pare (1510-1590) identified obstruction as a pathological entity, using mercury and lead bullets for severe cases.
• Franco (1561) performed the first surgery for strangulated hernia.
• Jonathan Hutchison (1871) conducted the first successful intussusception surgery, while Hirschprung (1877) used saltwater enema to reduce intussusception.
• In 1880, Block Parker and Kerr introduced exteriorization, primary resection, and anastomosis techniques.
• Roentgen (1893) discovered X-rays, and Schwartz (1911) highlighted their use in locating obstructions, with Kloiber (1919) emphasizing their importance in diagnosing the level of obstruction.
Embryology of Small Intestine
• The primitive gut is initially in communication with the yolk sac, forming the foregut, midgut, and hindgut.
• In the 5th week, the gut elongates rapidly, forming the primary intestinal loop, with the cephalic limb developing into the duodenum, jejunum, and proximal ileum, and the caudal limb forming the distal ileum, cecum, appendix, ascending colon, and transverse colon.
• The hindgut gives rise to the distal third of the transverse colon, sigmoid colon, rectum, and upper anal canal.
Rotation and Fixation of the Midgut Loop
• The midgut loop undergoes a 270° rotation, positioning the jejunum and ileum in the abdominal cavity.
• The pre-arterial segment forms the jejunum and ileum, while the post-arterial segment forms the colon.
• Deficient fixation can cause ptosis, torsion, and volvulus, while excessive fixation can lead to mobility issues, such as kinks or compression.
• Malrotation predisposes to volvulus, which leads to intestinal obstruction, particularly in the ileocecal region.
Anatomy of the Small Intestine
• The small intestine spans 6-7 meters, consisting of the duodenum, jejunum, and ileum.
• The duodenum is the shortest, widest, and most fixed part of the small intestine, divided into four parts: superior, descending, horizontal, and ascending.
• The jejunum occupies the upper left abdomen, and the ileum occupies the lower right abdomen and pelvis.
• Blood supply to the duodenum is from the right gastric, supraduodenal, and other arteries, while the jejunum and ileum receive blood from the superior mesenteric artery.
Pathophysiology of Bowel Obstruction
• Distension: The accumulation of gas and fluid leads to intestinal distension, reduced motility, and dehydration. Swallowed air, fermentation of sugars, and secretion interactions contribute to distension.
• Motility: Initially, increased motility tries to push contents past the obstruction. Over time, hypoxia and inflammation decrease motility, leading to a loss of gut contractility.
• Circulatory Changes: Vascular compromise from extrinsic pressure or closed-loop obstruction leads to ischemia, with severe cases progressing to strangulation. This triggers systemic inflammatory responses and organ dysfunction.
• Metabolic Effects: Proximal obstruction causes dehydration, hypochloremia, and metabolic alkalosis. Distal obstruction leads to more severe dehydration, hypotension, and shock, with the risk of bowel strangulation and organ failure.
Overview of Small Bowel Obstruction (SBO)
Small Bowel Obstruction (SBO) is a significant clinical condition characterized by the partial or complete blockage of the small intestine. The small bowel, which includes the duodenum, jejunum, and ileum, plays a crucial role in nutrient absorption and the passage of digestive contents. When an obstruction occurs, the normal flow of chyme (partially digested food), fluids, and gases is disrupted, leading to symptoms such as abdominal pain, bloating, vomiting, and constipation. SBO can result from a variety of causes, ranging from mechanical blockages (such as adhesions, hernias, tumors) to functional issues (such as paralytic ileus) [2].
SBO is a common surgical emergency, with a variety of etiologies that can affect individuals of all age groups. The condition is characterized by a spectrum of presentations, from mild, self-limiting cases to life-threatening emergencies. The pathophysiology of SBO involves increased intraluminal pressure, bowel distension, and changes in motility, which can lead to ischemia, bacterial overgrowth, and even perforation if left untreated [10].

Significance of Studying SBO in Clinical Settings
Studying SBO is critical for several reasons. First, SBO is one of the leading causes of acute abdominal pain and is responsible for a significant number of hospital admissions and surgical interventions worldwide. Understanding its etiology and the factors that influence patient outcomes can improve early diagnosis, guide treatment strategies, and reduce complications associated with delayed intervention.
Second, SBO can occur in a variety of clinical settings, including post-operative patients (especially those who have undergone abdominal surgery), individuals with chronic conditions like inflammatory bowel disease (IBD), or those with lifestyle-related risk factors like obesity or hernia. In each case, the management approach may differ based on the underlying cause, severity, and the patient's overall health status.
Finally, by studying the different causes, diagnostic techniques, and treatment modalities for SBO, healthcare professionals can provide more targeted and effective interventions. This can lead to better management of the condition, reduced hospital stays, and improved long-term outcomes for patients [11].
Brief Discussion of Clinical Importance and Need for Surgical Intervention
The clinical importance of SBO arises from the fact that, if left untreated or poorly managed, it can lead to severe complications such as bowel ischemia, necrosis, perforation, and sepsis. As SBO can progress rapidly, early recognition and intervention are critical to reducing morbidity and mortality.
While some cases of SBO, particularly partial obstructions or those caused by non-strangulated hernias, may resolve with conservative treatment (such as fluid resuscitation, nasogastric decompression, and bowel rest), many patients with complete or complicated SBO require surgical intervention. Surgical management is typically needed when there is evidence of strangulation (loss of blood flow to the affected bowel), perforation (rupture of the bowel wall), or non-resolution despite conservative treatment [12].
Surgical options range from exploratory laparotomy, which allows the surgeon to directly visualize and address the underlying cause of the obstruction, to minimally invasive laparoscopic techniques that are increasingly being used due to their shorter recovery times and reduced risk of infection. Depending on the etiology, surgical procedures may include adhesiolysis (removal of adhesions), hernia repair, bowel resection (removal of necrotic bowel tissue), or re-establishment of bowel continuity.
In summary, SBO is a serious condition that requires timely diagnosis and appropriate intervention. Studying its etiology, clinical presentation, and surgical management is essential to improving outcomes and reducing the burden of this common surgical emergency [2].
Etiology of Small Bowel Obstruction
The etiology of small bowel obstruction (SBO) can be broadly classified into mechanical and functional causes, with some less common causes contributing to the overall incidence of the condition. Understanding these causes is crucial for proper diagnosis and management, as the treatment and prognosis largely depend on the underlying etiology.
Mechanical Causes
i. Adhesions
o Definition and Pathophysiology: Adhesions are fibrous bands of scar tissue that form between bowel loops or between the bowel and the abdominal wall following surgery. These adhesions are the most common cause of SBO, particularly after abdominal or pelvic surgeries. They can cause partial or complete blockage by restricting the normal movement of the intestine or by constricting sections of the bowel.
o Clinical Impact: Adhesions may not cause symptoms immediately after surgery but can develop over time. They account for approximately 60-70% of SBO cases. Patients may experience intermittent symptoms of obstruction, which worsen as the adhesions contract and cause more pronounced mechanical obstruction.
o Management: Treatment for adhesions may initially involve conservative measures, such as fluid resuscitation and nasogastric decompression. However, surgical intervention (adhesiolysis) is often necessary if conservative management fails. Surgery involves removing or separating the fibrous bands to restore bowel movement [13].
ii. Hernias
o Definition and Types: Hernias occur when a portion of the bowel protrudes through a weak spot or opening in the abdominal wall or diaphragm. Common types of hernias that lead to SBO include inguinal, femoral, umbilical, and incisional hernias.
o Mechanism of Obstruction: Incarceration (when the bowel becomes trapped) and strangulation (when the blood supply to the bowel is compromised) are serious complications of hernias that can lead to SBO. These conditions are more likely to result in bowel ischemia, necrosis, and ultimately, perforation if not treated promptly [14].
o Clinical Presentation: Patients may present with localized pain, nausea, vomiting, and abdominal distension. In the case of strangulation, signs of systemic sepsis, including fever and tachycardia, may also be present.
o Management: Hernias require surgical repair, which may involve hernia reduction (for incarcerated hernias) and closure of the defect. In cases of strangulated hernias, bowel resection and re-anastomosis may be required if the bowel is necrotic [15].
iii. Tumors
o Malignant and Benign Tumors: Tumors, both benign (e.g., lipomas, leiomyomas) and malignant (e.g., adenocarcinomas, lymphoma), can obstruct the small bowel either by direct invasion or by extrinsic compression from surrounding structures.
o Mechanism: Tumors can cause obstruction by physically blocking the lumen of the bowel or by narrowing it over time. Malignant tumors may also compromise the blood supply to the bowel, leading to ischemia.
o Clinical Presentation: Symptoms typically include abdominal pain, vomiting, and weight loss, especially in cases of malignant tumors. Vomiting may be more pronounced due to proximal obstruction, and bowel distension is often present.
o Management: Surgical resection of the tumor is the mainstay of treatment, often accompanied by adjuvant chemotherapy or radiotherapy in the case of malignancy. Tumors in the small bowel may also require bowel resection with anastomosis [16].
iv. Volvulus
o Definition and Pathophysiology: Volvulus refers to the twisting of a portion of the bowel, leading to a mechanical obstruction and cutting off the blood supply to the affected segment. It commonly occurs in the sigmoid colon, but can also occur in the small bowel (particularly in the midgut).
o Clinical Impact: Volvulus can result in bowel ischemia and gangrene if not treated promptly. It is more common in older adults and in individuals with abnormal bowel motility.
o Clinical Presentation: The patient may present with acute abdominal pain, distension, vomiting, and signs of ischemia (e.g., tachycardia, fever, and hypotension).
o Management: Treatment involves untwisting the affected bowel (detorsion), usually followed by bowel resection if ischemia or necrosis is present. In some cases, a surgical procedure called a "defunctioning colostomy" may be performed [17].
v. Intussusception
o Definition and Mechanism: Intussusception occurs when one part of the intestine (the "intussusceptum") telescopes into the adjacent section (the "intussuscipiens"). This often leads to a blockage and can cause reduced blood flow to the affected bowel, potentially leading to necrosis.
o Clinical Presentation: While more common in children, adult cases of intussusception can present with abdominal pain, vomiting, and blood in the stool. In adults, it is often associated with an underlying tumor.
o Management: Non-surgical reduction is often performed in children, but in adults, surgery is frequently required. The treatment involves reducing the intussusception or resecting the affected bowel if there is necrosis or an underlying tumor [18].

Functional Causes
i. Paralytic Ileus
o Definition and Pathophysiology: Paralytic ileus is a functional obstruction in which there is a loss of normal peristalsis (the muscular contractions that move food through the digestive tract). This can occur due to a variety of factors such as surgery, medications, or electrolyte imbalances.
o Clinical Presentation: Symptoms of paralytic ileus include bloating, nausea, vomiting, and a lack of bowel sounds. Unlike mechanical obstruction, there is no physical blockage of the bowel.
o Management: Treatment involves addressing the underlying cause (e.g., correcting electrolyte imbalances, stopping offending medications, treating infections). In some cases, nasogastric decompression and supportive care (fluid resuscitation, nutritional support) may be necessary [19].
ii. Pseudo-Obstruction
o Definition and Mechanism: Pseudo-obstruction refers to the clinical signs and symptoms of SBO without a mechanical cause. This can be caused by neuromuscular disorders (e.g., Parkinson's disease, diabetes), trauma, or metabolic disturbances (e.g., hypothyroidism, hypokalemia).
o Clinical Presentation: Symptoms are similar to those of mechanical SBO, including abdominal pain, bloating, and vomiting, but without any structural abnormality on imaging.
o Management: Management focuses on treating the underlying disorder, as well as using prokinetic agents and supportive care to restore bowel function [20].
iii. Inflammatory Bowel Diseases (IBD)
o Role in SBO: Conditions like Crohn's disease and ulcerative colitis can lead to SBO due to chronic inflammation, stricture formation, or fibrosis of the bowel. These conditions can result in narrowing of the small intestine, causing functional or mechanical obstruction.
o Clinical Presentation: Symptoms of IBD-related SBO may include abdominal pain, diarrhea, weight loss, and malnutrition, with intermittent episodes of obstruction.
o Management: Treatment of IBD-related SBO may include medications (e.g., corticosteroids, immunosuppressants), nutritional support, and in some cases, surgery to remove strictures or diseased bowel segments [21].
Less Common Causes
i. Infection
o Mechanism: Infections like tuberculosis or tropical enteritis can cause bowel obstruction by leading to bowel wall thickening, ulceration, or granulomatous inflammation. These infections are more common in certain geographic areas and can mimic the symptoms of SBO.
o Management: Treatment typically involves antibiotics or antimicrobials targeted to the specific pathogen causing the infection.
ii. IBD-Related Strictures
o Pathophysiology: Chronic inflammatory diseases like Crohn's disease can lead to the formation of strictures (narrowing of the bowel lumen), which can cause partial or complete obstruction.
o Management: Management may include medical therapy to control the inflammation and prevent further narrowing, but in some cases, surgical intervention such as bowel resection may be necessary to remove the stricture [22].
iii. Other Rare Causes
o Foreign Bodies: Ingested foreign objects, particularly in children, can cause mechanical obstruction in the small bowel.
o Gallstones: Large gallstones can obstruct the small intestine, leading to a condition known as gallstone ileus, where a stone enters the bowel through a fistula.
o Vascular Obstruction: Conditions such as mesenteric ischemia, where blood flow to the small bowel is reduced, can cause bowel dysfunction and obstruction [23].
Clinical Presentation and Diagnosis
Symptoms: Abdominal Pain, Vomiting, Distension, Inability to Pass Gas or Stool
The clinical presentation of Small Bowel Obstruction (SBO) can vary depending on the severity, location, and cause of the obstruction. However, certain key symptoms are consistently observed in most patients, which help in the early identification and management of the condition.
i. Abdominal Pain
o Abdominal pain is the hallmark symptom of SBO. It often presents as crampy, colicky pain due to the peristaltic contractions of the intestine attempting to propel contents past the obstruction. The pain is usually intermittent and may worsen as the obstruction progresses.
o The location and nature of the pain can provide clues to the underlying cause. For instance, pain localized to a specific area might suggest a hernia or localized adhesion, while generalized pain could point to more widespread causes such as a tumor or volvulus [1].
ii. Vomiting
o Vomiting occurs as a result of the bowel's inability to move contents forward. The vomiting typically starts with food material and progresses to bile or feculent material as the obstruction worsens. The presence of feculent vomiting is a significant indicator of severe obstruction or bowel ischemia.
o Vomiting can lead to dehydration and electrolyte imbalances, which can complicate the clinical picture and worsen the patient's overall condition.
iii. Abdominal Distension
o Abdominal distension is common in SBO, particularly in cases of complete obstruction. It occurs due to the accumulation of gas and fluids above the site of obstruction, leading to visible swelling of the abdomen.
o Distension can be severe and may be associated with tenderness upon palpation, as the distended bowel wall becomes more sensitive [24].
iv. Inability to Pass Gas or Stool (Obstipation)
o The inability to pass gas (flatus) or stool is a classic sign of SBO. Patients typically report a lack of bowel movements and an inability to pass gas for several hours to days, depending on the severity of the obstruction.
o This symptom is particularly significant when it is associated with crampy abdominal pain and vomiting, as it suggests a mechanical blockage in the intestine.
Other symptoms that may be associated with SBO include fever (in cases of bowel ischemia or perforation), dehydration (due to vomiting and fluid loss), and an increase in heart rate (tachycardia), especially when sepsis is present [25].

Imaging Techniques: X-rays, CT Scans, Ultrasound, and Endoscopy for Diagnosis
Imaging plays a crucial role in confirming the diagnosis of SBO, determining the level and cause of the obstruction, and guiding management decisions. Several imaging modalities are commonly used, each with its advantages and limitations.
i. X-rays
o Abdominal X-ray is often the first imaging study performed in suspected cases of SBO. A plain X-ray can reveal classic signs of bowel obstruction, such as:
• Air-fluid levels: These are seen in a step-ladder pattern in upright films and indicate the presence of a blocked section of bowel.
• Dilated Bowel Loops: Dilatation of the proximal bowel occurs as a result of the obstruction. Typically, the bowel is dilated above the obstruction site, while the distal bowel may appear collapsed.
• Absent Gas in the Rectum: In cases of complete obstruction, the rectum may be gas-free, which supports the diagnosis of SBO.
o X-rays are particularly useful in detecting signs of free air, which may indicate bowel perforation, a life-threatening complication of SBO [5].
ii. CT Scan o CT Scan of the Abdomen is increasingly used in the diagnosis of SBO, especially when the cause is uncertain or when complications are suspected (e.g., strangulation or ischemia).
• Advantages: CT provides more detailed information than X-rays and can help identify the specific cause of the obstruction (e.g., hernia, tumor, adhesion, volvulus).
• Signs of SBO on CT: These include bowel distension, multiple air-fluid levels, and evidence of the obstructing cause (such as a tumor or a hernia sac).
• Detection of Complications: CT scans can also help assess for complications like bowel ischemia, perforation, or mesenteric ischemia by revealing signs such as bowel wall thickening, loss of bowel wall enhancement, or free air in the peritoneal cavity.
• High Sensitivity: CT is highly sensitive and accurate in diagnosing SBO, particularly in differentiating between partial and complete obstructions [5].
iii. Ultrasound
o Abdominal Ultrasound is a non-invasive imaging modality that can be helpful in certain situations, particularly in children and pregnant women, where radiation exposure is a concern.
• Signs of SBO on Ultrasound: Ultrasound can reveal distended bowel loops, especially in the small bowel. It is also useful in detecting fluid-filled loops and can help identify causes like hernias.
• Limitations: Ultrasound is less effective than CT in determining the precise cause of obstruction or evaluating complications such as ischemia or perforation.
iv. Endoscopy
o Endoscopic Examination is used primarily when the etiology of SBO is suspected to be due to a lesion that can be directly visualized, such as a tumor, foreign body, or inflammatory bowel disease.
v. Types of Endoscopy
• Gastroscopy: Can be used to assess the upper GI tract if the obstruction is suspected in the duodenum or proximal small intestine.
• Colonoscopy: Can be useful when the obstruction is located near the ileocecal valve or in cases of suspected colonic obstruction, particularly if there is concern for a tumor or stricture.
• Role in Diagnosis: Endoscopy is not usually the first choice for SBO diagnosis but can help in identifying and treating certain causes of obstruction (e.g., removal of foreign bodies, biopsy of tumors) [26].
Differential Diagnosis: Identifying SBO from Other Abdominal Conditions
SBO can present with symptoms similar to other abdominal conditions, making the differential diagnosis important. Differentiating SBO from other conditions ensures appropriate treatment and avoids unnecessary interventions. Some key conditions to consider in the differential diagnosis include:
• Acute Appendicitis:
o Both SBO and appendicitis can present with abdominal pain, vomiting, and distension. However, appendicitis is often characterized by localized right lower quadrant pain, which can help differentiate it from generalized SBO.
o A CT scan or ultrasound can help confirm appendicitis, showing an inflamed appendix or absence of obstruction.
• Acute Pancreatitis:
o Acute pancreatitis can cause upper abdominal pain, vomiting, and abdominal distension. However, the pain in pancreatitis is typically more constant and radiates to the back, and lab tests (amylase, lipase) can support the diagnosis.
o CT scans or ultrasound may reveal an inflamed pancreas or gallstones as the underlying cause [27].
• Perforated Peptic Ulcer:
o Perforated ulcers often present with sudden severe abdominal pain, vomiting, and distension, similar to SBO. However, the pain from a perforated ulcer is typically sharp and localized to the epigastric region. o Abdominal X-ray or CT can show free air under the diaphragm, indicating perforation, which is absent in SBO.
• Gastroenteritis:
o Gastroenteritis can present with vomiting, diarrhea, and abdominal discomfort, which overlap with SBO symptoms. However, diarrhea and the absence of obstipation (inability to pass gas or stool) help differentiate the two.
o The presence of fever and a history of recent infection may point towards gastroenteritis.
• Diverticulitis:
o Diverticulitis can cause localized abdominal pain, usually in the left lower quadrant, along with fever, nausea [28].
Indications for Surgical Management
Surgical management in Small Bowel Obstruction (SBO) is often required when the condition is severe, unresponsive to conservative treatments, or complicated by additional factors such as strangulation, ischemia, or bowel perforation. Early intervention is crucial to prevent complications like bowel necrosis, perforation, and systemic infection. Understanding when surgical intervention is necessary, how to manage patients preoperatively, and the criteria for determining the timing of surgery are all vital to improving patient outcomes and reducing morbidity and mortality associated with SBO [1].
When Surgery is Required: Complete vs Partial Obstruction, Strangulation, Ischemia
Surgical intervention is generally indicated in cases of complete SBO, complications such as strangulation or ischemia, and when conservative management fails. The severity and progression of the obstruction, along with the patient's overall health and response to nonoperative treatment, dictate the decision to proceed with surgery.
• Complete vs Partial Obstruction
o Partial Obstruction: In cases of partial SBO, where the bowel is only partially obstructed, nonoperative measures are often successful. Conservative treatments like fluid resuscitation, nasogastric decompression, and bowel rest are usually sufficient, with a significant number of cases resolving spontaneously over time. However, the clinical course must be monitored closely. If symptoms persist or worsen, surgical intervention may be necessary, especially if the obstruction progresses or if there is suspicion of complications like strangulation or perforation [2].
o Complete Obstruction: Complete SBO represents a more severe form, where there is a total blockage of the intestinal lumen. This type of obstruction is often more urgent and generally does not resolve with conservative management. Surgical intervention is often required to relieve the obstruction, prevent bowel necrosis, and avoid more severe complications. Incomplete relief from conservative treatments, failure to pass gas or stool, or worsening abdominal pain and distension would typically prompt the need for surgery [1].
• Strangulation
o Strangulated Obstruction occurs when there is a loss of blood flow to a segment of the bowel due to the obstruction. This leads to ischemia, and if untreated, can progress to bowel necrosis and perforation. Strangulation is considered a surgical emergency and is associated with significantly higher morbidity and mortality. Signs of strangulation include severe, constant pain, a tense and tender abdomen, fever, tachycardia, and sometimes signs of systemic infection or shock. Surgical intervention is urgently needed to relieve the obstruction and to assess and possibly resect the ischemic bowel to prevent sepsis [29].
• Ischemia
o Ischemic Bowel occurs when blood flow to a portion of the small intestine is compromised, leading to tissue hypoxia and potential necrosis. This can occur due to strangulation, mesenteric artery occlusion, or volvulus. If the ischemia is not rapidly addressed, it can lead to irreversible damage, bowel perforation, peritonitis, and septic shock. Surgical treatment typically involves resecting the non-viable bowel tissue and restoring blood supply where possible. In cases of mesenteric ischemia, thrombolysis or embolectomy may also be considered to restore blood flow to the affected area [30].
Preoperative Management: Fluid Resuscitation, Nutritional Support, Infection Control
Preoperative management plays a critical role in optimizing the patient's condition before surgery and minimizing the risk of complications. Effective management can enhance recovery, improve surgical outcomes, and reduce postoperative morbidity.
• Fluid Resuscitation
o Patients with SBO often present with dehydration due to vomiting, fluid loss, and decreased oral intake. Fluid resuscitation is essential to restore the intravascular volume, correct electrolyte imbalances (especially sodium, potassium, and bicarbonate), and prevent hypovolemic shock. Intravenous (IV) fluids, including crystalloids (e.g., normal saline or Ringer's lactate), are administered to stabilize the patient. The use of appropriate IV fluids helps to maintain blood pressure and tissue perfusion, thus optimizing the patient's ability to tolerate surgery. In severe cases, blood products may be required if significant fluid loss or hemorrhage has occurred [31].
• Nutritional Support
o Nutritional support is crucial, especially if the SBO is prolonged. A nasogastric tube (NGT) is often used to decompress the stomach and prevent further accumulation of gastric contents. In cases of prolonged SBO, total parenteral nutrition (TPN) may be considered to provide essential nutrients and maintain the patient's nutritional status while bowel rest is required. If surgical correction is delayed, enteral nutrition through a nasojejunal tube may be an option if tolerated, although the use of enteral nutrition is typically avoided during active obstruction.
• Infection Control
o Patients with SBO, especially those at risk of bowel perforation or strangulation, are susceptible to infections like peritonitis, sepsis, and wound infections. Broad-spectrum antibiotics are often started preoperatively to prevent or treat infections, particularly if there is concern for bowel perforation or ischemia. If signs of infection (fever, tachycardia, hypotension) are present, aggressive antibiotic therapy is essential to reduce the risk of postoperative complications. Antibiotics are tailored based on the patient's clinical status and culture results once available [32].
Criteria for Surgery: Timing and Decision-Making for Surgical Intervention
The timing of surgery is crucial, as delays in intervention can lead to worsened outcomes, including bowel ischemia, necrosis, and systemic infection. Several criteria help in making the decision for surgery, based on the severity of symptoms, the response to conservative management, and the patient's clinical condition.
• Timing of Surgery
o Early Surgical Intervention: In cases of complete obstruction, strangulation, or ischemia, surgery is typically indicated without delay. The longer the bowel is obstructed, the higher the risk of ischemic injury and perforation, leading to sepsis and multiorgan failure. Early intervention is crucial in preventing these complications. Surgery should also be performed promptly if conservative treatment is unsuccessful within 48–72 hours of symptom onset. The condition of the patient, including their hemodynamic stability and response to fluid resuscitation, should also be considered when determining the timing.
o Delayed Surgical Intervention: In some cases, surgery may be delayed if the obstruction is partial and the patient is responding well to conservative management. If the patient shows signs of improvement (e.g., decreasing abdominal distension, passing gas or stool), the need for surgery may be postponed. However, careful monitoring is essential, and if the patient's condition worsens or if there are signs of complications, surgery should be performed without hesitation. Delaying surgery in cases of strangulated or ischemic bowel can result in increased morbidity and mortality [33].
• Decision-Making for Surgery
o Clinical Assessment: The decision to perform surgery is guided by the patient's clinical condition. Key factors to consider include the severity of symptoms (pain, distension, vomiting), physical examination findings (tenderness, fever, signs of sepsis), and laboratory results (elevated white blood cell count, electrolyte imbalances). The patient's overall health status, comorbidities, and ability to tolerate surgery also play a significant role in decision-making.
o Imaging Results: Imaging studies (e.g., CT scan, abdominal X-rays) provide critical information regarding the location and cause of the obstruction. CT scans, in particular, are useful for identifying the presence of ischemia, strangulation, or perforation. These findings can expedite the decision to perform surgery. In cases where the cause is unclear or complicated (e.g., unclear etiology, massive distension), exploratory laparotomy may be indicated.
o Surgical Considerations: Once surgery is deemed necessary, the approach is determined by the underlying cause of the obstruction. For example, if adhesions are the cause, adhesiolysis may be performed. If a hernia is present, the hernia will need to be reduced and repaired. In cases of tumors or strictures, resection and anastomosis may be required. The surgeon must also consider the patient's condition (e.g., risk of complications like wound infection, anastomotic leak) when determining the type of surgery [34].
Surgical Procedures and Postoperative Outcomes
Surgical management of small bowel obstruction (SBO) is crucial in cases where conservative treatment fails or when the obstruction is complicated by factors such as strangulation, ischemia, or perforation. The surgical approach depends on the underlying cause of the obstruction and the patient's overall condition. Postoperative outcomes, including recovery time and potential complications, play an important role in determining the success of the intervention.
Surgical Approaches: Exploratory Laparotomy, Laparoscopic Surgery, Adhesiolysis, Hernia Repair, and Bowel Resection
The surgical approach to SBO depends on the severity of the obstruction, its cause, and the clinical condition of the patient. Several surgical procedures are employed to relieve the obstruction, remove the underlying cause, and restore normal bowel function.
• Exploratory Laparotomy
o Indications: An exploratory laparotomy is typically performed when the cause of the obstruction is uncertain or when there are signs of complications such as strangulation or bowel perforation. It involves a large abdominal incision to directly visualize the abdominal contents, identify the site of the obstruction, and treat any underlying causes [1].
o Procedure: The surgeon carefully inspects the small and large intestines, identifying areas of obstruction, ischemia, or perforation. If adhesions are present, they may be divided, or if a hernia is present, it may be reduced and repaired. Any damaged or necrotic bowel is removed, and the remaining bowel is re-anastomosed to restore continuity.
o Advantages: It provides direct access to the abdomen and allows for the removal or repair of obstructing lesions, such as adhesions, tumors, or hernias. It also provides the ability to treat complications like ischemia or perforation [2].
• Laparoscopic Surgery
o Indications: Laparoscopy is increasingly being used as a minimally invasive approach to treat SBO, particularly when the underlying cause is due to adhesions or small hernias. It involves using small incisions and a camera to visualize the abdominal cavity and perform the surgery.
o Procedure: Laparoscopic surgery offers the advantage of quicker recovery, less postoperative pain, and smaller scars. The surgeon uses specialized instruments to address the cause of obstruction, such as adhesiolysis or hernia repair, through the small incisions. If necessary, bowel resection and anastomosis can also be performed laparoscopically.
o Advantages: Minimally invasive techniques reduce hospital stay and the risk of wound infection. Laparoscopy is associated with less postoperative pain, quicker mobilization, and faster recovery times, especially in uncomplicated cases of SBO [35].
o Limitations: Laparoscopy is not always feasible in complicated SBO cases, such as those involving bowel ischemia, massive adhesions, or perforation, as the conditions may require a more extensive approach.
• Adhesiolysis
o Indications: Adhesiolysis is the surgical procedure of choice when SBO is caused by adhesions. It is typically performed when the obstruction is due to post-surgical adhesions that bind the bowel loops together or to the abdominal wall.
o Procedure: The surgeon carefully separates the adhesions using blunt or sharp dissection. If the adhesions are extensive, laparotomy may be necessary to allow for thorough dissection. Laparoscopic adhesiolysis is also possible in some cases.
o Complications: While adhesiolysis can effectively relieve the obstruction, it carries the risk of bowel injury or damage to surrounding organs, which may lead to further complications [36].
• Hernia Repair
o Indications: Hernia repair is indicated when the obstruction is caused by an incarcerated or strangulated hernia. The hernia may be reducing (the bowel may be manually pushed back into the abdomen) or incarcerated (trapped without blood supply), requiring surgical intervention.
o Procedure: If the hernia is strangulated, the affected portion of the bowel may need to be resected. Once the bowel is reduced or resected, the surgeon repairs the defect in the abdominal wall. In some cases, mesh is used to reinforce the repair and reduce the risk of recurrence.
o Complications: The recurrence of the hernia after repair can occur, especially if the repair is not done with adequate tension. In complicated cases, bowel necrosis may necessitate resection and bowel anastomosis [37].
• Bowel Resection
o Indications: Bowel resection is performed when there is bowel ischemia, necrosis, or extensive damage to the bowel due to prolonged obstruction, strangulation, or volvulus. It may also be indicated in cases of tumors or strictures that cause a mechanical blockage.
o Procedure: The affected portion of the bowel is surgically removed, and the healthy ends are re-anastomosed to restore bowel continuity. In some cases, a stoma (colostomy or ileostomy) may be temporarily created if an anastomosis is not feasible.
o Complications: Potential complications include anastomotic leakage, wound infections, and nutritional malabsorption. Patients who undergo bowel resection may require longer recovery times and close follow-up to ensure proper bowel function [38].
Postoperative Recovery: Monitoring, Infection Control, and Nutritional Support
Postoperative care is critical to ensuring a successful recovery after surgery for SBO. Following surgery, patients must be closely monitored for complications, and various supportive measures must be implemented to aid recovery.
• Monitoring
o Vital Signs: Monitoring the patient's vital signs, including heart rate, blood pressure, respiratory rate, and temperature, is essential to detect early signs of complications such as infection or shock.
o Abdominal Examination: The surgical site and abdomen must be carefully examined to assess for signs of infection, distension, or peritonitis. Bowel sounds should be monitored to assess the return of bowel motility.
o Urine Output: Adequate urine output is an important indicator of kidney function and fluid balance. A drop in urine output can suggest dehydration, shock, or renal insufficiency, necessitating further intervention.
• Infection Control
o Antibiotics: Prophylactic antibiotics are commonly administered before surgery to reduce the risk of postoperative infections. If bowel perforation or contamination occurs during surgery, antibiotics may be continued postoperatively.
o Wound Care: Proper wound care is critical to prevent infections, especially in cases of laparotomy, where the incision is larger and the risk of wound infection is higher. Regular dressing changes and monitoring for signs of infection (redness, discharge, fever) are essential.
o Sepsis Management: If sepsis develops, it is vital to escalate treatment with appropriate antibiotics, fluid resuscitation, and possibly vasopressor support to maintain hemodynamic stability [31].
• Nutritional Support
o Fluid and Electrolyte Balance: Postoperatively, patients are at risk of dehydration due to the loss of fluids during surgery, vomiting, or nasogastric drainage. IV fluids are essential to maintain hydration and restore electrolyte balance. This is particularly important in patients who have undergone bowel resections or extensive adhesiolysis.
o Enteral Nutrition: Early enteral nutrition is beneficial in promoting recovery, as it helps maintain gut integrity and reduces the risk of infection. If bowel function is restored, oral feeding is gradually resumed, starting with clear liquids and progressing to solid foods.
o Parenteral Nutrition: In cases of prolonged SBO or when the patient cannot tolerate enteral nutrition, total parenteral nutrition (TPN) may be required. TPN provides essential nutrients intravenously and helps maintain the patient's nutritional status until normal bowel function is restored [39].
Short-Term and Long-Term Outcomes: Recovery Time, Complications, Recurrence Rates
The outcomes following surgery for SBO vary depending on the underlying cause, the surgical procedure performed, and the patient's overall health. Both short-term and long-term outcomes should be carefully monitored to ensure the best possible recovery.
• Short-Term Outcomes
o Recovery Time: The length of hospital stay varies based on the type of surgery performed and the patient's response to treatment. Patients who undergo laparoscopic surgery often have shorter recovery times, with many being discharged within a few days. In contrast, those who undergo open surgery (e.g., exploratory laparotomy) may require a longer stay, especially if there are complications or if bowel resection is necessary.
o Complications: Short-term complications include wound infections, anastomotic leaks, intra-abdominal abscesses, deep vein thrombosis (DVT), and pulmonary embolism. Close monitoring for signs of these complications is essential for early intervention. Early ambulation and deep breathing exercises can help reduce the risk of thromboembolic complications [40].
• Long-Term Outcomes
o Recurrence Rates: Recurrence of SBO is common, especially in cases where adhesions are the primary cause. Adhesions can form again postoperatively, leading to further episodes of obstruction. Some studies report recurrence rates of up to 20% to 30% within 5 years of surgery. Patients who undergo bowel resection may also be at risk for long-term bowel dysfunction or malabsorption, particularly if a significant portion of the small intestine is removed.
o Chronic Pain and Bowel Dysfunction: Some patients experience chronic abdominal pain, bloating, or altered bowel habits after surgery, especially if the bowel was resected or if complications such as adhesions or ischemia occurred. Long-term follow-up is necessary to monitor for any lasting gastrointestinal issues [41].
Previous Studies
Lo et al. This study reviewed 430 patients who underwent surgery for small bowel obstruction (SBO) to evaluate the risk factors influencing early postoperative outcomes. The most common causes of SBO were peritoneal adhesions (42.3%) and hernias (26.8%). The study found that old age, female sex, nonadhesive obstructions, and hernias were significantly associated with bowel strangulation. The 30-day mortality rate was 6.5%, with a median postoperative hospital stay of 8 days. Old age and comorbidities like pulmonary disease were independent factors associated with higher mortality. The overall complication rate was 35.5%, and old age was the only significant factor related to postoperative complications [42].
Meier et al. - This study compared outcomes of 221 patients with acute SBO treated either surgically (136 patients) or conservatively (85 patients). The study found that the recurrence of SBO symptoms and hospitalizations were significantly lower in the surgical group, with 14% of surgical patients being readmitted for recurrent SBO, compared to 29.4% in the conservative group. The study concluded that surgical management of SBO led to fewer recurrent symptoms and hospitalizations compared to conservative treatment. However, the need for further surgery for new SBO episodes was similar between the two groups. Mortality rates did not differ significantly between surgical and conservative treatments [43].
Karakas et al. This retrospective study evaluated 735 patients with acute mechanical bowel obstruction (AMBO) to analyze the etiology, management, and survival. The study found that adhesions were the most common cause (43.3%), followed by tumors (26.2%) and hernias (6%). The study indicated that conservative management was the most common approach (53.2%), while surgical resection was performed in 21.9%. The overall mortality rate was 8.6%, with tumors being the leading cause of death. The study observed that adhesions were particularly prevalent in patients post-abdominal surgery [44].
Markogiannakis et al. This prospective study analyzed the clinical presentation, etiology, management, and outcomes of 150 patients with acute mechanical bowel obstruction. The study found that the most common causes were adhesions (64.8%), incarcerated hernias (14.8%), and large bowel cancer (13.4%). The majority of patients (58.7%) were treated conservatively, while 41.3% required surgery. The study highlighted the importance of early diagnosis and emphasized that while many cases can be managed conservatively, a significant proportion require immediate surgical intervention due to the risk of bowel ischemia, necrosis, and perforation [45].
Reddy & Cappell (201) This systematic review focused on recent developments in the diagnosis and treatment of small bowel obstruction (SBO). It highlighted that abdominal adhesions were the most common cause of SBO (60-70% of cases), with hernias and neoplasms being other significant causes. The study emphasized the use of abdominal CT for diagnosis, noting that SBO usually resolves with medical therapy but requires surgical intervention for cases of complete obstruction, perforation, or severe ischemia. Laparoscopy was noted as an increasingly common approach for surgical management of adhesive SBO. The overall mortality for SBO was around 10%, rising to 30% in cases of bowel necrosis or perforation [46].
Maung et al., In this article, the authors discuss the evaluation and management of small-bowel obstruction (SBO) as part of the Eastern Association for the Surgery of Trauma (EAST) guidelines. The study emphasizes the importance of computed tomography (CT) as a critical diagnostic tool for SBO, particularly multidetector CT scans with multiplanar reconstructions. The authors recommend surgical exploration for patients showing clinical signs of generalized peritonitis or those with evidence of ischemia on imaging. In contrast, initial nonoperative management can be safely performed for both partial and complete SBO in patients without significant clinical deterioration. The role of laparoscopy as a viable alternative to laparotomy in selected cases is also highlighted. The article concludes with evidence-based guidelines aimed at improving the diagnosis and management of SBO [47].
Girma et al. focus on the outcomes of surgically treated cases of small-bowel obstruction (SBO) at a hospital in Ethiopia. The study found that sigmoid volvulus and adhesions were the most frequent causes of obstruction. Surgery was performed on 69% of the patients, with a 5.5% mortality rate. The study identified significant predictors of adverse outcomes, including prior surgery, ischemic changes, and delayed presentation. The authors conclude that early intervention and proper preoperative management are crucial in improving survival rates, and recommend enhancing surgical care capacity in resource-limited settings for better management of SBO [48].
Pedziwiatr et al. review changes in the epidemiology of mechanical bowel obstruction (MBO) over the years, with a particular focus on the role of adhesions in modern cases. The study notes that adhesions have replaced volvulus as the leading cause of MBO, reflecting changes in the clinical setting and surgical practices. The authors also highlight that although many cases of SBO resolve conservatively, surgical intervention remains necessary in cases of strangulation, bowel necrosis, or when conservative management fails. The article suggests that advances in diagnostic imaging and minimally invasive surgical techniques have improved the overall prognosis of SBO patients [49].
Beyene and Negassa investigate the outcomes of small-bowel obstruction (SBO) at a hospital in Ethiopia, focusing on the impact of different management approaches. Sigmoid volvulus and adhesions were found to be the most common causes of SBO, with 69.3% of patients undergoing surgery. The study highlights that early diagnosis and timely surgical intervention are critical in reducing complications, which include bowel ischemia, perforation, and sepsis. Mortality rates were low, but prolonged hospital stays and recurrence were notable outcomes. The authors recommend strengthening diagnostic and surgical resources to improve management outcomes in the region [50].
Mir et al. This study, conducted in India, reviewed 51 patients with small bowel obstruction (SBO) admitted between June 2016 and December 2018. The majority of patients were aged around 44.7 years, with abdominal pain and vomiting being common presenting symptoms. Adhesion obstruction was the most common cause (52.9%), followed by malignancy (15.7%). Management was divided into conservative (49%) and surgical (51%) approaches, with laparoscopic adhesiolysis performed in 21.6% of patients. The results showed that laparoscopic surgery led to faster recovery and fewer complications compared to open surgery, with a statistically significant difference in operative time, hospital stay, and time for bowel recovery [51].
Olausson et al. This multicenter prospective study in Denmark examined the management and short-term outcomes of patients with small bowel obstruction (SBO). The study included 316 patients with a median age of 72 years, and CT scans were used for diagnosis in 99% of cases. Non-operative management was successful in 78.3% of cases, and urgent surgery was performed in the remaining patients. The study found that despite the higher surgery rates in Denmark compared to international standards, patient outcomes (mortality of 7.3% and morbidity of 17.1%) were similar to those of more conservative management strategies. The study highlights the benefits of early surgical intervention and the high success rates of non-operative management in stable patients [52].
Choi et al. This systematic review and meta-analysis focused on the safety of non-operative management for small bowel obstruction (SBO) in patients without previous abdominopelvic surgery (virgin abdomen). The analysis, which included six cohort studies, found that de novo adhesions were the most common cause of SBO in this group. The prevalence of malignant causes was around 7.7%, but most were not suspected before surgery. Non-operative management was successful in up to 84% of cases, although a high proportion of trials failed. The study concluded that, while non-operative management is often attempted, it may not be safe to forego surgery entirely in all patients, and careful monitoring and follow-up are essential [52].
Materials and Methods
Study Type
The study was designed as a prospective observational study, aiming to examine the clinical outcomes, management approaches, and various factors influencing surgical intervention in cases of small bowel obstruction (SBO). As a prospective study, it tracked patients from the point of admission through their treatment, monitoring the progression of their condition and their postoperative outcomes. This observational nature allowed for the collection of real-time clinical data, providing an opportunity to evaluate the effectiveness of both surgical and conservative management options for SBO.
Study Site
The study was conducted at a tertiary health-care center, which is a specialized hospital providing advanced care for patients with complex medical conditions. This setting allowed for the inclusion of patients from a wide demographic, including those with severe or complicated cases of SBO that require specialized surgical intervention. The study site had the necessary facilities and resources, including state-of-the-art diagnostic tools, specialized surgeons, and intensive care units for managing the postoperative recovery of patients with SBO.
Study Duration
The study was planned to span from December 2022 to July 2025, a period of approximately 2.5 years. This duration allowed ample time to accumulate a sufficient sample size of patients with SBO, as well as time to observe the long-term outcomes and complications of surgical interventions. The extended study period also enabled researchers to analyze variations in patient demographics, etiology, and surgical outcomes, allowing for a more comprehensive understanding of SBO management.
Study Sample
The study sample consisted of patients diagnosed with small bowel obstruction (SBO) who underwent surgical intervention during the study period. All patients who were diagnosed with SBO and treated surgically at the study site were included in the sample.
Inclusion Criteria
• All operated cases of small bowel Obstruction of all age groups.
Exclusion Criteria
• Operated cases with intraoperative findings of small bowel pathology along with additional pathology . (eg. Perforated appendix , gynecological pathology)
Procedure and Methodology
This study was conducted in the Department of General Surgery at a tertiary care center over a period of 30 months, from December 2022 to July 2025. During this period, cases of small bowel obstruction (SBO) were studied and analyzed to understand the clinical presentation, management, and postoperative outcomes.
The diagnosis of SBO was provisionally established by the surgeon based on clinical presentation and supporting radiological evidence, including abdominal X-rays and CT scans, while the definitive diagnosis was confirmed at the time of surgery. Cases with additional bowel pathologies or co-existing small bowel perforation were excluded from the study to focus specifically on primary SBO cases.
Surgical Timing Categorization: Based on the time interval between hospital admission and surgery, cases were categorized into three groups:
• Immediate Surgery: Surgery performed within 4 hours of hospital admission.
• Same-Day Surgery: Surgery performed within 4 to 24 hours of admission.
• Delayed Surgery: Surgery performed more than 24 hours after admission.
Operative Detail: The study collected comprehensive data regarding the surgical procedure performed. This included:
• The site of the obstruction (e.g., jejunum, ileum, or duodenum).
• The size of any perforation or stricture, if present.
• The nature and quantity of peritoneal soiling, which helps assess the extent of bowel contamination.
• The gross appearance of the bowel affected by the obstruction.
• The nature of the surgical operation performed (e.g., adhesiolysis, bowel resection, hernia repair). In cases where appropriate, tissue biopsies were taken for histological confirmation to further assess the nature of the obstructing lesion.
Outcomes
• Mortality was defined as death occurring after the surgical intervention.
• Morbidity was defined in terms of the duration of hospital stay and any complications associated with the surgery (e.g., wound infection, anastomotic leak, or bowel dysfunction).
Data Collection: Details were gathered from the patients' case sheets and clinical examination records, which included the following information:
• Patient Demographics: Name, age, sex, and inpatient number.
• Clinical Features: Detailed record of the clinical presentation, including symptoms such as abdominal pain, vomiting, distension, and inability to pass gas or stool.
• Abdominal Findings: Observations during clinical examination, such as tenderness, guarding, or rebound tenderness, which would indicate peritoneal irritation or ischemia.
This data was then analyzed to evaluate the relationship between surgical timing, operative findings, and patient outcomes, with a focus on factors that influence morbidity and mortality in small bowel obstruction cases.
Results
This prospective observational study was conducted on a cohort of 50 patients who presented with clinical signs and symptoms consistent with small bowel obstruction (SBO) and subsequently underwent surgical management at a tertiary care hospital. The results reported herein are organized thematically into demographic profiles, clinical characteristics, preoperative assessment, intraoperative findings, postoperative outcomes, and statistical interpretation. All patients included in the study satisfied the inclusion criteria of surgically treated SBO with no intraoperatively identified confounding pathologies, such as appendicitis or gynecological disease.
Demographic and Baseline Characteristics
A total of 50 patients were enrolled in the study. The age of patients ranged from 18 to 82 years, with a mean age of 49.2 years
|
Age Group (Years) |
Frequency |
Percentage (%) |
|
18–30 |
10 |
20.0 |
|
31–40 |
9 |
18.0 |
|
41–50 |
3 |
6.0 |
|
51–60 |
5 |
10.0 |
|
>60 |
23 |
46.0 |
Table 1: Frequency Distribution of Age Groups

Figure 1: Bar Chart for Frequency Distribution of Age Groups
With respect to sex distribution, males constituted a higher proportion of cases compared to females. Specifically, 60% of the patients were male (n = 30), while 40% were female (n = 20), establishing a male-to-female ratio of 1.5:1. This male predominance in surgical SBO aligns with prior literature suggesting higher rates of surgical adhesions and hernia-related obstructions in men.
|
Sex |
Frequency |
Percentage (%) |
|
Male |
30 |
60.0 |
|
Female |
20 |
40.0 |
Table 2: Sex-wise Distribution of Patients
Figure 2: Pie chart for Sex-wise Distribution of Patients
Clinical Presentation
The symptom duration prior to hospital admission varied significantly across the cohort. Approximately 20% of patients presented within 24 hours of symptom onset, whereas a larger proportion (64%) presented between 1 to 5 days of symptom progression. The delay in presentation may be attributed to initial misinterpretation of symptoms or lack of access to tertiary care. Table 3 summarizes the distribution of symptom duration at presentation.
|
Duration |
Frequency |
Percentage (%) |
|
<24 hours |
9 |
18.0 |
|
1–2 days |
20 |
40.0 |
|
3–5 days |
21 |
42.0 |
Table 3: Duration of Symptoms Prior to Admission
Abdominal distension was one of the most frequently reported symptoms, present in 86% of patients. This reflects the physiological impact of luminal obstruction and associated bowel dilation, a key clinical indicator necessitating radiologic evaluation and potential operative intervention.
|
Distension |
Frequency |
Percentage (%) |
|
Yes |
43 |
86.0 |
|
No |
7 |
14.0 |
Table 4: Frequency of Abdominal Distension
Vomiting was reported by nearly all patients. The type of vomitus was categorized based on patient history, with bilious vomiting observed in a majority (68%), indicating a more proximal obstruction site in many cases.
|
Vomiting Type |
Frequency |
Percentage (%) |
|
Bilious |
34 |
68.0 |
|
Non-bilious |
16 |
32.0 |
Table 5: Type of Vomitus Observed Among Patients
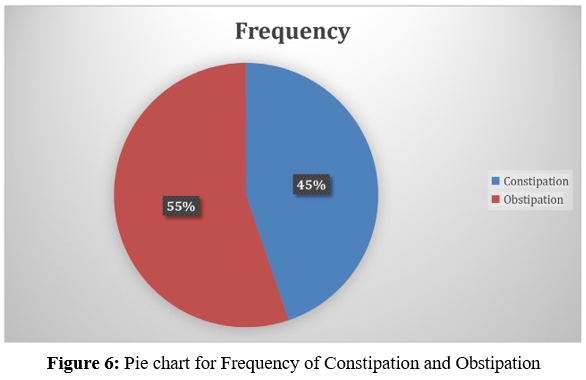
Constipation and obstipation were analyzed as distinct yet often overlapping symptoms. Constipation was present in 60% of patients, whereas obstipation—a more severe form characterized by absence of both stool and flatus—was noted in 74%, consistent with complete mechanical obstruction.
|
Symptom |
Frequency |
Percentage (%) |
|
Constipation |
30 |
60.0 |
|
Obstipation |
37 |
74.0 |
Table 6: Frequency of Constipation and Obstipation
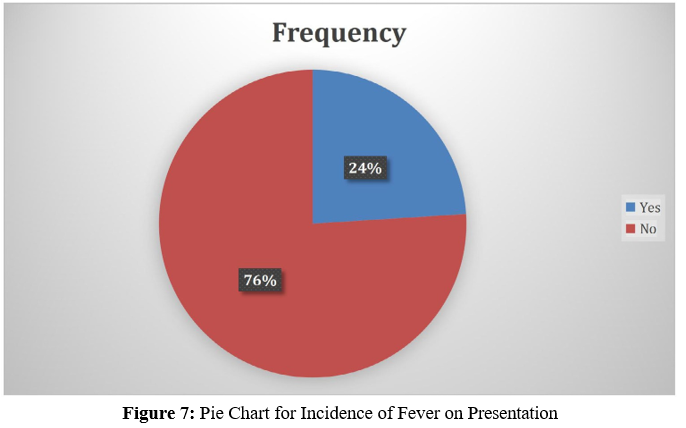
Fever, though not universally present, was identified in 24% of cases. Fever often indicates evolving complications such as peritonitis or ischemia, necessitating prompt surgical intervention.
|
Fever |
Frequency |
Percentage (%) |
|
Yes |
12 |
24.0 |
|
No |
38 |
76.0 |
Table 7: Incidence of Fever on Presentation
Bowel sounds were categorized into hyperactive, hypoactive, and silent. Hyperperistalsis was observed in 44% of cases, while 20% had absent bowel sounds, suggestive of late-stage obstruction or ischemic compromise.
|
Peristalsis Type |
Frequency |
Percentage (%) |
|
Hyperactive |
22 |
44.0 |
|
Hypoactive |
18 |
36.0 |
|
Silent |
10 |
20.0 |
Table 8: Distribution of Peristalsis Status

Figure 8: Pie Chart for Distribution of Peristalsis Status
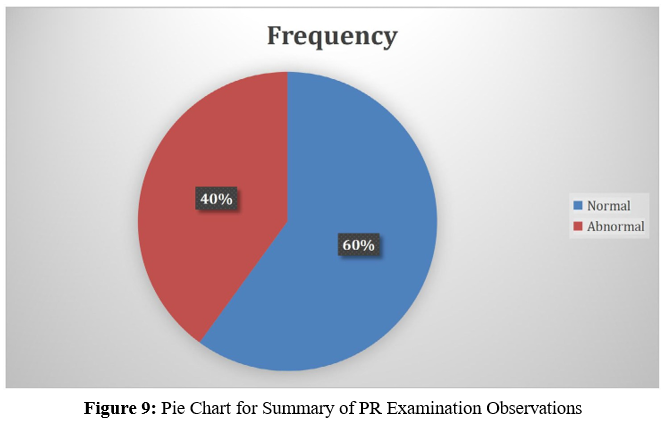
Per rectal examination findings played a critical role in confirming distal obstruction and ruling out palpable masses or rectal bleeding. Approximately 40% of patients had abnormal findings on digital rectal examination (DRE), including empty rectum or impacted stool.
|
PR Finding |
Frequency |
Percentage (%) |
|
Normal |
30 |
60.0 |
|
Abnormal |
20 |
40.0 |
Table 9: Summary of PR Examination Observations
Preoperative Assessment
The preoperative evaluation of all patients included assessment of renal perfusion, hematologic parameters, electrolyte status, and imaging findings. These data were essential in determining the operative risk, need for fluid resuscitation, and stratifying patients for early versus delayed surgical intervention.
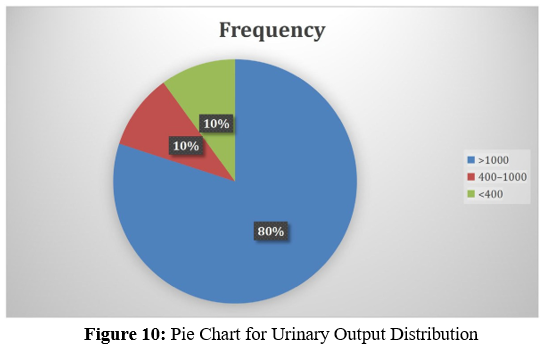
Urine Output Per Day
Assessment of renal output was conducted at admission. A majority (80%) of patients had urine output exceeding 1000 mL/ day, indicating adequate renal perfusion. However, oliguria (<400 mL/day) was noted in 10% of the patients, necessitating urgent resuscitative measures.
|
Output Range (mL/day) |
Frequency |
Percentage (%) |
|
>1000 |
40 |
80.0 |
|
400–1000 |
5 |
10.0 |
|
<400 |
5 |
10.0 |
Table 10: Urinary Output Distribution
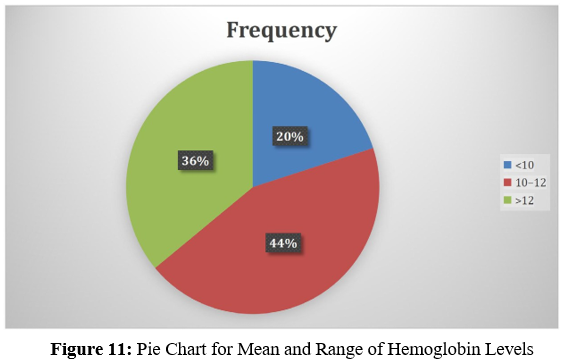
Hemoglobin (HB) Levels
The mean hemoglobin level across the cohort was 11.2 ± 1.6 g/ dL. Ten patients (20%) had hemoglobin values below 10 g/ dL. Preoperative anemia was particularly evident in patients undergoing resection, likely secondary to chronic blood loss or nutritional deficiencies.
|
Hb Level (g/dL) |
Frequency |
Percentage (%) |
|
<10 |
10 |
20.0 |
|
10–12 |
22 |
44.0 |
|
>12 |
18 |
36.0 |
Table 11: Mean and Range of Hemoglobin Levels
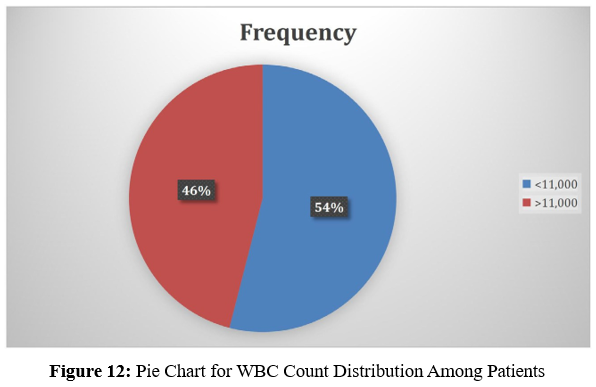
White Blood Cell (WBC) Count
White cell counts were elevated (>11,000/mm³) in 46% of patients, suggesting systemic inflammatory response. Neutrophilic predominance was commonly observed in these cases, which is consistent with bowel ischemia or evolving peritonitis.
|
WBC Count (/mm³) |
Frequency |
Percentage (%) |
|
<11,000 |
27 |
54.0 |
|
>11,000 |
23 |
46.0 |
Table 12: WBC Count Distribution Among Patients
8.3.4. Serum Potassium (K+) and Sodium (Na+) Levels
Electrolyte derangements were prevalent at presentation. Hypokalemia (K+< 3.5 mmol/L) was observed in 28% of patients, whereas hyponatremia (Na+ < 135 mmol/L) was noted in 38%. These disturbances reflect vomiting-induced losses and third-space fluid sequestration in bowel loops.
|
Electrolyte |
Normal (n) |
Abnormal (n) |
% Abnormal |
|
Sodium (Na+) |
31 |
19 |
38.0 |
|
Potassium (K+) |
36 |
14 |
28.0 |
Table 13: Serum Electrolyte Status Preoperatively

Figure 13: Bar chart for Serum Electrolyte Status Preoperatively
Radiological Findings
Radiological confirmation of SBO was integral to diagnosis. Imaging was done via erect abdominal X-rays, ultrasound (USG), and contrast-enhanced computed tomography (CECT), depending on clinical indication.
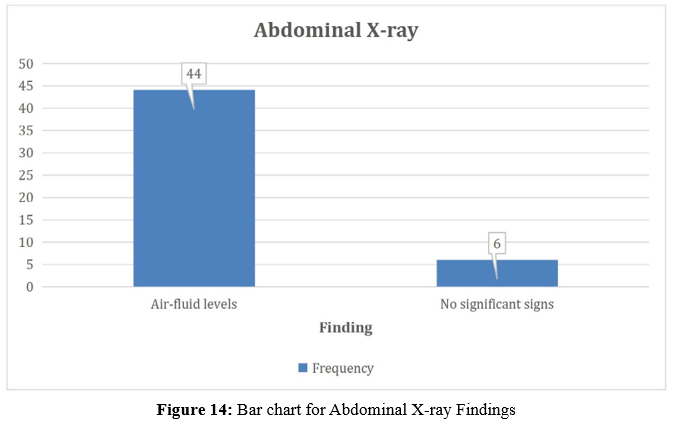
Air-Fluid Levels on X-Ray
Air-fluid levels were observed in 88% of patients, a hallmark radiologic sign of small bowel obstruction. Absence of classical radiological findings did not exclude diagnosis, especially in early-stage presentations.
|
Finding |
Frequency |
Percentage (%) |
|
Air-fluid levels |
44 |
88.0 |
|
No significant signs |
6 |
12.0 |
Table 14: Abdominal X-ray Findings
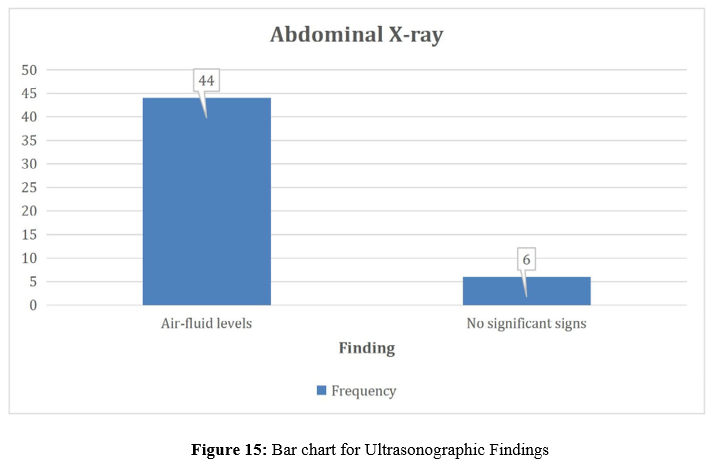
Bowel Dilatation on (Ultrasound)
Ultrasound confirmed bowel dilatation in 84% of cases. While operator-dependent, USG remains a non-invasive bedside modality that aids rapid screening in unstable patients.
|
Bowel Dilatation |
Frequency |
Percentage (%) |
|
Present |
42 |
84.0 |
|
Absent |
8 |
16.0 |
Table 15: Ultrasonographic Findings
CECT Findings
Contrast-enhanced CT scans were performed in 20 cases (40%) based on severity, atypical presentation, or suspicion of closed-loop obstruction. The transition zone was visible in 50% of these scans, and closed-loop obstruction was identified in 30%. CECT was instrumental in triaging patients for immediate surgical intervention.
|
Finding |
Frequency |
Percentage (%) (of 20) |
|
Transition zone |
10 |
50.0 |
|
Closed loop obstruction |
6 |
30.0 |
|
No significant findings |
4 |
20.0 |
Table 16: CECT Abdomen Results Summary

Figure 16: Bar chart for CECT Abdomen Results Summary
Intraoperative Findings
All patients underwent laparotomy under general anesthesia after adequate preoperative optimization. The intraoperative findings were categorized based on the nature of the obstruction, etiology, and extent of surgical intervention required. Adhesions were the most common cause, followed by resectable strictures and hernias.
Type of Surgery Performed
Adhesiolysis was the most frequently performed surgical procedure, accounting for 40% of cases. Resection and primary anastomosis were necessary in 30% of patients, usually those with gangrenous or non-viable bowel segments. Other procedures included strictureplasty for tubercular or inflammatory strictures, band release in congenital causes, and hernia repair.
|
Type of Surgery |
Frequency |
Percentage (%) |
|
Adhesiolysis |
20 |
40.0 |
|
Resection and Anastomosis |
15 |
30.0 |
|
Strictureplasty |
5 |
10.0 |
|
Band Release |
6 |
12.0 |
|
Hernia Repair |
4 |
8.0 |
Table 17: Surgical Procedures Undertaken
Duration of Surgery
Operative duration varied depending on the complexity of the obstruction and the need for bowel resection or reconstruction. The mean operative time was 94.6 ± 22.5 minutes. Patients undergoing resection and anastomosis had longer surgical times (mean ~112 minutes) compared to those receiving adhesiolysis or hernia repair.
|
Etiology |
Mean Duration (min) |
Range (min) |
|
Adhesions |
78.2 ± 14.5 |
60–100 |
|
TB Strictures |
104.5 ± 19.6 |
85–130 |
|
Hernia-related |
82.3 ± 12.8 |
70–105 |
|
Volvulus/Closed loop |
112.8 ± 17.3 |
90–140 |
Table 18: Mean Operative Time by Etiology
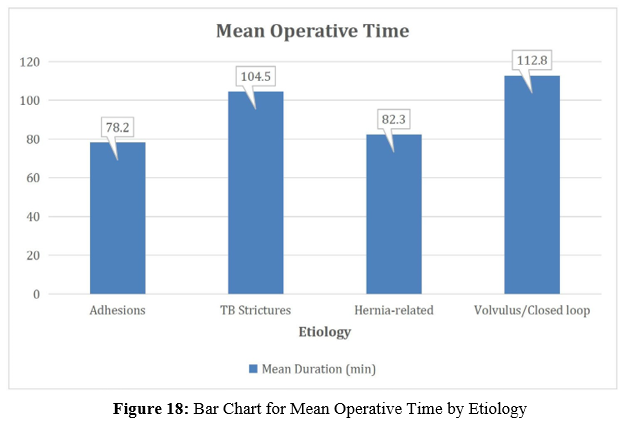
Drain Insertion
Abdominal drains were inserted in 62% of cases. The highest frequency of drain usage was noted in patients who underwent resection and anastomosis, primarily as a precautionary measure in high-risk or contaminated fields.
|
Surgery Type |
Drain Placed (n) |
Percentage (%) |
|
Resection & Anastomosis |
14 |
93.3 |
|
Adhesiolysis |
10 |
50.0 |
|
Other Procedures |
7 |
58.3 |
Table 19: Frequency of Drain Placement by Surgery Type

Figure 19: Bar Chart for Frequency of Drain Placement by Surgery Type
Postoperative Outcomes
Postoperative recovery was monitored closely in terms of return of bowel activity, complications such as wound discharge or ileus, and need for reintervention. The length of hospital stay was recorded for each patient and correlated with surgical findings and outcomes.
Duration of Postoperative Antibiotic Use
Patients received intravenous antibiotics postoperatively ranging from 3 to over 7 days. The mean duration was 5.6 ± 1.8 days. Patients with resected bowel or postoperative complications received extended antibiotic therapy.
|
Duration (days) |
Frequency |
Percentage (%) |
|
3–5 |
28 |
56.0 |
|
6–7 |
15 |
30.0 |
|
>7 |
7 |
14.0 |
Table 20: Number of Days of Antibiotics Post-Surgery
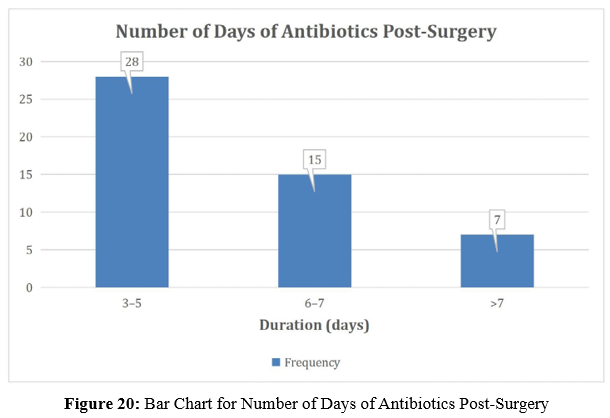
Stitch Line Discharge
Stitch line discharge was observed in 6 patients (12%), all of which were managed with local wound care and extended dressings. No surgical site infections required operative drainage.
|
Discharge |
Frequency |
Percentage (%) |
|
Present |
6 |
12.0 |
|
Absent |
44 |
88.0 |
Table 21: Incidence of Stitch Line Discharge
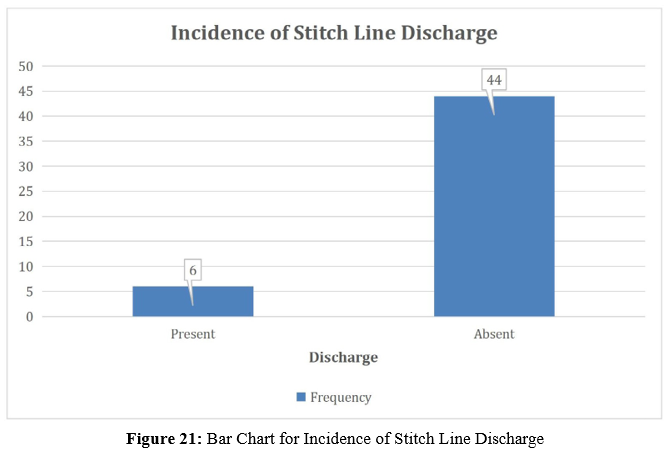
Postoperative Ileus Nine
patients (18%) developed postoperative ileus, which resolved conservatively in most cases. These patients had delayed return of bowel sounds, increased nasogastric aspirate, and mild abdominal distension.
|
Ileus |
Frequency |
Percentage (%) |
|
Present |
9 |
18.0 |
|
Absent |
41 |
82.0 |
Table 22: Frequency of Postoperative Ileus

Figure 22: Bar Chart for Frequency of Postoperative Ileus
Return of Peristalsis (Post-Op Day)
The return of bowel sounds, a proxy for gastrointestinal recovery, occurred most frequently on postoperative day 2, with 20% of patients showing recovery within the first day.
|
Post-op Day |
Frequency |
Percentage (%) |
|
Day 1 |
10 |
20.0 |
|
Day 2 |
22 |
44.0 |
|
Day 3 |
12 |
24.0 |
|
≥Day 4 |
6 |
12.0 |
Table 23: Postoperative Day of Return of Bowel Sounds
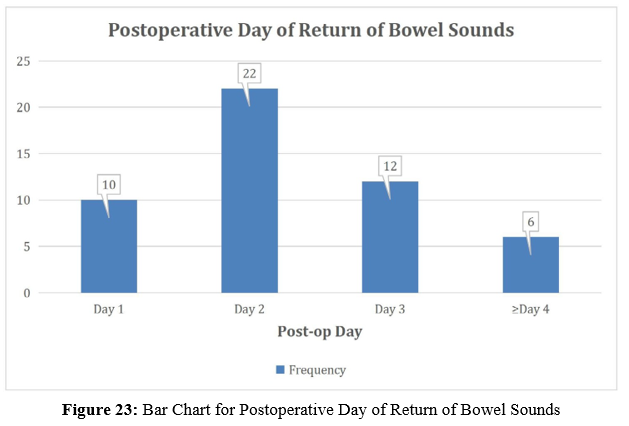
8.5.5. Postoperative Serum Potassium (K+)
Persistent hypokalemia (<3.5 mmol/L) was observed in 8 patients despite intraoperative and postoperative correction. These patients required potassium supplementation and delayed resumption of oral feeding.
|
K+ Level (mmol/L) |
Frequency |
Percentage (%) |
|
<3.5 |
8 |
16.0 |
|
3.5–5.0 |
42 |
84.0 |
Table 24: Postoperative Potassium Levels
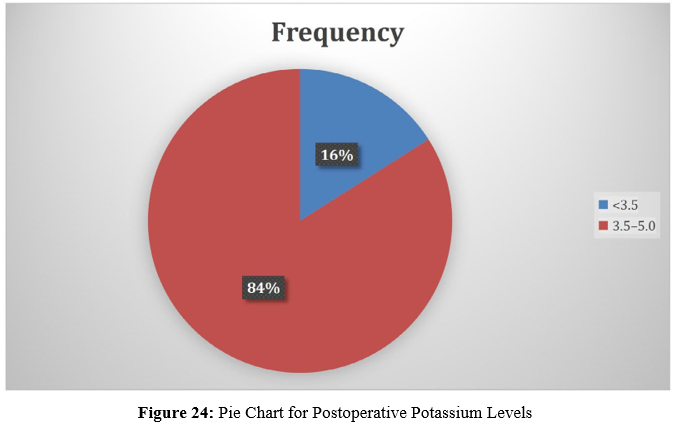
Re-Intervention Required
Three patients (6%) required surgical re-intervention. Two underwent re-exploration for burst abdomen and one for anastomotic leak. All were managed successfully with secondary procedures.
|
Re-intervention |
Frequency |
Percentage (%) |
|
Required |
3 |
6.0 |
|
Not required |
47 |
94.0 |
Table 25: Surgical Re-Intervention Rates

Figure 25: Pie Chart for Surgical Re-Intervention Rates
Duration of Hospital Stay
The average hospital stay was 8.4 ± 2.3 days. Patients with resection and complications stayed longer, while uncomplicated adhesiolysis cases were discharged earlier.
|
Category |
Mean Stay (days) |
|
Adhesiolysis (no complications) |
6.8 ± 1.4 |
|
Resection (with complication) |
11.2 ± 2.1 |
|
Other uncomplicated cases |
7.5 ± 1.6 |
Table 26: Length of Hospital Stay by Etiology and Complication
Statistical Analysis
To provide a comprehensive understanding of the relationships between clinical presentation, surgical findings, and postoperative outcomes, a series of descriptive summaries, correlation tests, and significance analyses were conducted. All tests adhered to standard statistical methodologies with p-values < .05 considered statistically significant.
Descriptive Statistics
Descriptive statistics summarized the central tendency and dispersion of key demographic, hematologic, and biochemical parameters. The mean age of the patients was 49.2 years with a standard deviation of 15.1. Hemoglobin levels ranged from 8.4 to 14.2 g/dL, with a mean of 11.2. White blood cell counts varied from 8,400 to 16,200/mm³, with a mean of approximately 11,380.
|
Parameter |
Mean ± SD |
Range |
|
Age (years) |
49.2 ± 15.1 |
18–82 |
|
Hemoglobin (g/dL) |
11.2 ± 1.6 |
8.4–14.2 |
|
WBC (/mm³) |
11,380 ± 2,110 |
8,400–16,200 |
|
Serum Sodium (Na+) |
135.8 ± 4.2 |
128–143 |
|
Serum Potassium (K+) |
3.9 ± 0.5 |
2.9–5.1 |
|
Hospital Stay (days) |
8.4 ± 2.3 |
5–16 |
Table 27: Summary Statistics for Demographic and Lab Parameters
Stratification by Etiology
Outcomes varied significantly by underlying etiology. Patients with adhesive obstruction had the lowest complication rates (10%), while those with tubercular or volvulus-related obstruction had substantially higher rates. Notably, patients with volvulus had a mean hospital stay exceeding 11 days.
|
Etiology |
Complication Rate (%) |
Mean Hospital Stay (days) |
|
Adhesions |
10.0 |
6.8 |
|
Tubercular Strictures |
33.3 |
10.5 |
|
Hernia-related |
25.0 |
8.7 |
|
Volvulus/Closed Loop |
50.0 |
11.2 |
Table 28: Comparison of Outcomes by Surgical Etiology
These data support the clinical understanding that etiology directly impacts not only surgical complexity but also the likelihood of complications and extended hospitalization.
Correlation Analysis Between Variables
Pearson correlation coefficients were computed between key clinical parameters and postoperative outcomes, such as complication rates and duration of hospital stay. A moderate positive correlation (r = 0.41) was found between the duration of symptoms and hospital stay. Elevated white blood cell count also showed a moderate correlation (r = 0.45) with postoperative complications.
|
Variables |
Hospital Stay (r) |
Complications (r) |
|
Duration of Symptoms |
0.41 |
0.38 |
|
WBC Count |
0.33 |
0.45 |
|
Serum Sodium (Na+) |
–0.27 |
–0.31 |
|
Type of Surgery (Ordinal) |
0.44 |
0.39 |
Table 29: Correlation Matrix of Clinical and Outcome Variables
These correlations indicate that longer symptom duration, elevated WBC, and more invasive surgery are moderately associated with poor outcomes.
Association Tests (Chi-Square / T-Test)
To determine the statistical significance of relationships observed in clinical practice, categorical variables were assessed using Chi-square tests, while continuous variables were compared using independent sample t-tests. Several significant associations were identified:
• A statistically significant association was found between type of surgery and postoperative complications (X² = 6.49, p = .038), with resection procedures carrying a higher risk.
• Hyponatremia was significantly associated with postoperative ileus (t = 2.35, p = .021), suggesting that sodium imbalance may impair intestinal motility recovery.
• Duration of symptoms showed a strong correlation with length of hospital stay (r = 0.41, p = .003), confirming the prognostic value of early presentation.
|
Parameter |
Test Used |
p-value |
Interpretation |
|
Surgery Type vs. Complication |
Chi-square |
.038 |
Significant association |
|
Serum Na+ vs. Post-op Ileus |
t-test |
.021 |
Significant association |
|
Fever vs. WBC Elevation |
Chi-square |
.107 |
Not significant |
|
Duration vs. Hospital Stay |
Pearson r |
.003 |
Significant correlation |
Table 30: Tests of Significance: Clinical Parameters vs. Outcomes
Relationship between Hypokalemia and Postoperative Ileus in Small Bowel Obstruction Surgery
This table summarizes the relationship between hypokalemia (serum potassium levels < 3.5 mmol/L) and the development of postoperative ileus in patients who underwent surgery for small bowel obstruction (SBO). It highlights the prevalence of hypokalemia, its potential role in exacerbating ileus, and the impact of electrolyte correction on postoperative recovery. Statistical associations and clinical management strategies are also discussed to underscore the importance of electrolyte balance in preventing complications like ileus post-su
|
Factor |
Hypokalemia (K+ < 3.5 mmol/L) |
Postoperative Ileus |
|
Prevalence in the cohort |
28% (14 patients) |
18% (9 patients) |
|
Relation between the conditions |
Hypokalemia can impair motility, contributing to ileus. |
8 patients with ileus had persistent hypokalemia. |
|
Postoperative correction |
Corrected intraoperatively and postoperatively, but 16% had persistent hypokalemia. |
Ileus management included nasogastric aspiration and supportive care. |
|
Outcome and Management |
Potassium supplementation required for correction. |
Correction of hypokalemia can improve ileus recovery. |
|
Statistical Association |
Significant association with low sodium and ileus (p = 0.021). |
Hypokalemia can prolong ileus and recovery. |
Table 31: Relationship Between Hypokalemia and Postoperative Ileus
Discussion
Small bowel obstruction (SBO) represents a prevalent surgical emergency encountered in general surgical practice worldwide. The prompt identification, appropriate classification, and timely surgical intervention remain pivotal in reducing morbidity and mortality associated with this condition. The present prospective observational study evaluated 50 patients who were surgically managed for SBO at a tertiary care hospital. Through structured documentation and rigorous analysis of clinical, biochemical, radiological, intraoperative, and postoperative data, this study aimed to identify the predominant etiologies, clinical profiles, surgical practices, and patient outcomes in the context of SBO. These findings are not only reflective of local epidemiology but also contribute to the wider discourse on SBO management, particularly within the context of resource-constrained healthcare settings.
The demographic profile observed in this study aligns with several global reports, albeit with regional variations. The mean age of the patients in the present cohort was 49.2 years, and a substantial proportion (46%) were above 60 years of age. This finding corroborates existing literature suggesting that SBO, particularly due to adhesions and malignancy, predominantly affects older individuals. However, the notable representation of younger patients (nearly 20% in the 18–30 age group) underscores the need to consider congenital bands, tubercular strictures, and postoperative adhesions in younger age groups, especially in regions with high tuberculosis prevalence and increasing rates of laparotomies in reproductive age populations.
Sex distribution in the present study revealed a male predominance (60%), resulting in a male-to-female ratio of 1.5:1. This trend has also been reported in prior studies, with potential explanations including higher rates of occupational physical strain, delayed health-seeking behavior among males, and increased incidence of hernia and adhesive disease. Conversely, in populations where gynecological pathologies contribute significantly to abdominal surgeries, female preponderance in postoperative adhesions has also been observed. However, given the exclusion criteria in this study which omitted patients with intraoperative gynecological pathologies, the sex-related etiologic distribution may be inherently influenced by selection bias.
Symptomatology in SBO is characteristically dominated by abdominal pain, distension, vomiting, and altered bowel habits. In the present cohort, abdominal distension was the most frequent symptom, reported in 86% of cases. This finding is consistent with literature emphasizing that distension is nearly universal in complete or high-grade obstructions. Vomiting was reported in all patients, with 68% experiencing bilious vomiting, typically indicative of proximal obstruction. The presence of constipation and obstipation in 60% and 74% of patients respectively reinforces the classical clinical triad used to suspect mechanical obstruction. Importantly, 24% of the patients also presented with fever, potentially suggestive of bowel ischemia or systemic inflammatory response due to strangulated bowel or perforation, which warrants immediate operative intervention.
Peristaltic activity, as assessed clinically and supported by auscultation, revealed that 44% of patients exhibited hyperactive bowel sounds, typically associated with early or partial obstruction. Conversely, hypoactive and absent bowel sounds, found in 36% and 20% respectively, indicate progression to ileus or ischemic bowel compromise, findings that have been similarly described by Araujo Teixeira et al. and Ucaner et al. These results validate the diagnostic utility of a focused clinical examination in the early stratification of obstruction severity.
Preoperative laboratory parameters provided key insights into patient physiology at presentation. The mean hemoglobin level was 11.2 g/dL, with 20% of patients exhibiting values below 10 g/dL. These findings are in line with the known nutritional deficiencies and chronic blood loss often observed in patients with obstructive or inflammatory bowel conditions. The elevation of white blood cell counts in nearly half the cohort (46%) points toward a systemic inflammatory or septic response. Similar hematologic alterations were reported by Al-Darwish et al., who identified leukocytosis as a reliable predictor of bowel strangulation. Serum sodium and potassium abnormalities were prevalent in 38% and 28% of patients, respectively, underscoring the volume depletion, vomiting, and third-space losses characteristic of SBO. These biochemical disturbances are clinically significant and must be corrected promptly before anesthesia induction to reduce perioperative complications.
Radiological evaluation remains central to confirming the diagnosis of SBO and planning surgical strategy. In this study, abdominal X-rays were diagnostic in 88% of patients, revealing the classic air-fluid levels. Although abdominal radiography remains a widely accessible first-line modality, its sensitivity is limited, especially in partial obstruction or early-stage disease. Ultrasonography demonstrated bowel dilatation in 84% of cases, supporting its role as a bedside, non-invasive, and repeatable tool, particularly useful in unstable patients. However, it was the contrast-enhanced CT (CECT) scans—performed in 20 selected patients—?that provided detailed anatomical delineation, revealing transition zones and closed-loop obstructions in 80% of scanned patients. The superior diagnostic yield of CECT, as compared to plain radiographs and ultrasound, has been established in previous studies (Sohil & Apoorva, 2012), and was reaffirmed in this cohort. This highlights the necessity for selective use of CECT, especially in patients with inconclusive clinical and preliminary imaging findings.
Surgical intervention varied according to intraoperative findings and underlying pathology. Adhesiolysis was the most frequently performed procedure (40%), consistent with global reports which identify adhesions as the leading cause of SBO, especially in developed and increasingly in developing nations with high surgical volumes. Resection and anastomosis were performed in 30% of cases, often due to gangrenous or ischemic bowel secondary to volvulus or closed-loop obstruction. The mean operative time was understandably higher in these cases, reflecting the complexity and meticulous technique required for bowel resection and reconstruction. The overall frequency of drain insertion (62%) was appropriately higher in resection cases (93%), in line with the standard surgical practice to monitor anastomotic integrity and peritoneal contamination.
Postoperative recovery and complication profiles were closely examined. The mean hospital stay across all patients was 8.4 days, with extended durations observed in patients undergoing resection or experiencing postoperative complications. The median time to return of bowel sounds was postoperative day 2, which matches established recovery timelines in gastrointestinal surgery. However, 18% of patients developed postoperative ileus, a finding consistent with the incidence reported by Sanchez et al. and indicative of delayed gastrointestinal motility secondary to surgical handling, electrolyte imbalances, or underlying sepsis. Persistent hypokalemia in 16% of patients after surgery, despite intraoperative correction, further supports the hypothesis that electrolyte disturbances play a key role in ileus development.
Stitch line discharge occurred in 12% of patients, though none required surgical re-intervention for wound complications. Re-exploration was necessitated in only three patients (6%), two for burst abdomen and one for anastomotic leak. This rate compares favorably with published data, where reoperation rates in SBO range from 5–15% depending on etiology and institutional protocols. Importantly, there was no recorded mortality in the present study, highlighting the effectiveness of timely diagnosis, adequate preoperative optimization, and standardized perioperative protocols in mitigating adverse outcomes.
Statistical analysis yielded several clinically meaningful insights. First, the duration of symptoms before presentation significantly correlated with prolonged hospital stay, emphasizing the critical value of early presentation and referral. Second, elevated WBC count and low sodium levels were significantly associated with postoperative complications, particularly ileus, aligning with the findings of Ten Broek et al. who identified these as markers of systemic stress. Perhaps most importantly, the type of surgery performed was significantly associated with complication rates; resections carried a higher burden of morbidity than simple adhesiolysis or band releases. This reinforces the importance of conservative surgery when feasible, alongside careful patient selection for more extensive procedures.
Compared with other recent observational studies, the present study exhibits several consistent findings, including the predominance of adhesions, the utility of CECT in complex diagnoses, and the association of biochemical abnormalities with adverse outcomes. However, unlike some of these studies, particularly those from high-income countries, tuberculosis remains a significant contributor to SBO in this cohort, necessitating high clinical suspicion and timely anti-tubercular therapy where indicated.
The strengths of this study include its prospective design, well-defined inclusion and exclusion criteria, and comprehensive variable tracking, ranging from clinical findings to postoperative outcomes. The embedded statistical analysis has helped identify real-time predictors of poor prognosis, allowing for evidence-informed decisions in future clinical settings. Nevertheless, certain limitations must be acknowledged. The sample size, while sufficient for descriptive and correlational analyses, limits the generalizability of inferential conclusions. Larger multicenter studies are needed to validate these associations in diverse populations. Additionally, due to resource constraints, not all patients underwent uniform imaging (CECT), which could have introduced bias in surgical planning. Finally, the follow-up period was limited to six weeks post-discharge; thus, long-term complications such as adhesive recurrence or incisional hernias could not be captured.
Summary
Small bowel obstruction (SBO) is a critical surgical emergency characterized by a complex interplay of etiologies, clinical manifestations, and outcomes. This prospective observational study was conducted over a period of 30 months at a tertiary care center, involving 50 patients who underwent surgical intervention for SBO. The primary objectives were to evaluate the various causes of SBO, assess the indications for operative management, and correlate intraoperative findings with postoperative outcomes.
Patients were enrolled based on stringent inclusion criteria, specifically excluding those with intraoperative findings of confounding pathologies such as appendicitis or gynecological disease. A comprehensive master chart captured variables ranging from demographic and symptom profiles to laboratory parameters, radiologic findings, surgical details, and postoperative recovery indicators.
The demographic analysis revealed that SBO was more prevalent in elderly males, with a mean patient age of 49.2 years and a male-to-female ratio of 1.5:1. The most common clinical presentations included abdominal distension (86%), vomiting (68% bilious), and obstipation (74%). Laboratory evaluations indicated that nearly half of the patients had elevated white blood cell counts and significant electrolyte imbalances, notably hyponatremia and hypokalemia.
Radiological imaging played a pivotal role in diagnosis and preoperative planning. While X-rays demonstrated classical air-fluid levels in most cases, CECT scans offered detailed anatomical resolution in 40% of patients, identifying transition zones and closed-loop obstructions with high sensitivity. Intraoperatively, adhesiolysis emerged as the most frequent surgical procedure, followed by resection and anastomosis in more complicated presentations such as ischemia or volvulus.
Postoperative outcomes varied by the nature of surgery and patient condition at presentation. The average hospital stay was 8.4 days, and the complication rate was highest in patients requiring bowel resection. Common postoperative complications included ileus (18%) and stitch line discharge (12%), though the overall morbidity remained within acceptable limits. Re-intervention was needed in only three cases (6%), and no mortality was reported.
Statistical analysis affirmed significant associations between duration of symptoms, laboratory derangements, type of surgery, and postoperative outcomes. In particular, elevated WBC counts and low sodium levels were predictive of prolonged recovery and complications. The findings underscore the critical role of timely intervention, the value of detailed clinical and radiological assessment, and the need for context-specific surgical decision-making.
In essence, this study highlights the multifactorial nature of small bowel obstruction and emphasizes that early diagnosis, guided surgical planning, and vigilant postoperative care are essential for achieving optimal clinical outcomes. These insights contribute to the growing body of evidence on SBO and may inform future clinical guidelines, particularly in similar high-burden, resource-variable settings.
Conclusion
This prospective observational study on surgically treated cases of small bowel obstruction offers a comprehensive overview of the clinical spectrum, underlying etiologies, intraoperative findings, and short-term outcomes associated with this surgical emergency. Conducted at a tertiary care hospital over a span of 30 months, the study provides valuable insights into the real-world management of SBO in a high-volume, resource-conscious clinical setting.
The findings underscore that adhesive obstruction remains the predominant cause of SBO in the postoperative population, while other etiologies such as tubercular strictures, congenital bands, and hernias also contribute significantly, especially in regions with endemic infections and high surgical burden. The clinical presentation was consistent with established literature, with abdominal distension, vomiting, and obstipation serving as key diagnostic indicators. Importantly, early recognition of these features, coupled with targeted imaging—particularly contrast-enhanced computed tomography—enabled timely and appropriate surgical decision-making.
Intraoperatively, the type of surgical procedure was found to be a critical determinant of postoperative outcomes. Patients undergoing adhesiolysis generally had favorable recoveries with shorter hospital stays and fewer complications. In contrast, those requiring resection and anastomosis for ischemic or gangrenous bowel were at increased risk of postoperative ileus, electrolyte imbalances, and delayed gastrointestinal recovery. These findings reaffirm the importance of conservative surgery when feasible and the need for aggressive perioperative optimization in complex cases.
Biochemical parameters, including elevated white blood cell counts and hyponatremia, emerged as significant predictors of postoperative morbidity. These easily accessible markers should be integrated into early risk stratification protocols to improve perioperative monitoring and anticipate complications. The absence of mortality in this cohort is a testament to the efficacy of prompt diagnosis, structured resuscitation, skilled surgical intervention, and diligent postoperative care.
In conclusion, small bowel obstruction continues to pose diagnostic and therapeutic challenges, but its outcomes can be significantly improved through early recognition, evidence-based surgical strategies, and context-specific postoperative management. This study contributes to the growing understanding of SBO by reinforcing the value of individualized care and offers practical insights for surgical teams working in similar healthcare environments. Future studies with larger sample sizes and extended follow-up periods are warranted to further refine treatment protocols and assess long-term sequelae, such as adhesion recurrence or incisional hernias. Until then, the emphasis must remain on timely intervention, clinical vigilance, and adaptable surgical judgment.
References
- Kulaylat, M. N., & Doerr, R. J. (2001). Small bowel obstruction. In Surgical treatment: evidence-based and problem-oriented. Zuckschwerdt.
- Schick, M. A., Kashyap, S., Collier, S. A., & Meseeha, M. (2025). Small bowel obstruction. In StatPearls [Internet]. StatPearls Publishing.
- Catena, F., De Simone, B., Coccolini, F., Di Saverio, S., Sartelli, M., & Ansaloni, L. (2019). Bowel obstruction: a narrative review for all physicians. World Journal of Emergency Surgery, 14(1), 20.
- Ford, M. M. (2021). Crohn's disease obstructions. Clinics in Colon and Rectal Surgery, 34(04), 227-232.
- Nelms, D. W., & Kann, B. R. (2021). Imaging modalities for evaluation of intestinal obstruction. Clinics in colon and rectal surgery, 34(04), 205-218.
- Tong, J. W. V., Lingam, P., & Shelat, V. G. (2020). Adhesive small bowel obstruction–an update. Acute Medicine & Surgery, 7(1), e587.
- Ghimire, S. K., Shrestha, S., Jha, R., Maharjan, S., & Shrestha,M. (2025). Small bowel obstruction secondary to strangulated obturator hernia with transected ileal segment: A case report. International Journal of Surgery Case Reports, 129, 111098.
- Ten Broek, R. P., Krielen, P., Di Saverio, S., Coccolini, F., Biffl, W. L., Ansaloni, L., ... & van Goor, H. (2018). Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group. World Journal of Emergency Surgery, 13(1), 24.
- Catena, F., Di Saverio, S., Kelly, M. D., Biffl, W. L., Ansaloni, L., Mandalà, V., ... & Jeekel, J. (2011). Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2010 evidence-based guidelines of the World Society of Emergency Surgery. World Journal of Emergency Surgery, 6(1), 5.
- Miller, G., Boman, J., Shrier, I., & Gordon, P. H. (2000). Etiology of small bowel obstruction. The American Journal of Surgery, 180(1), 33-36.
- Detz, D. J., Podrat, J. L., Castro, J. C. M., Lee, Y. K., Zheng, F., Purnell, S., & Pei, K. Y. (2021). Small bowel obstruction. Current problems in surgery, 58(7), 100893.
- Aka, A. A., Wright, J. P., & DeBeche-Adams, T. (2021). Small bowel obstruction. Clinics in Colon and Rectal Surgery, 34(04), 219-226.
- Welle, N. J., Sajjad, H., Adkins, A., & Burns, B. (2017). Bowel adhesions.
- Lassandro, F., Iasiello, F., Pizza, N. L., Valente, T., di Santo Stefano, M. L. M., Grassi, R., & Muto, R. (2011). Abdominal hernias: radiological features. World journal of gastrointestinal endoscopy, 3(6), 110.
- Kang, C. H., & Tsai, C. Y. (2014). Richter's femoral hernia manifested by a progressive ileus. Formosan Journal of Surgery, 47(5), 193-196.
- Gupta, S., & Gupta, S. (1982). Primary tumors of the small bowel: a clinicopathological study of 58 cases. Journal of surgical oncology, 20(3), 161-167.
- Lieske, B., & Antunes, C. (2023). Sigmoid volvulus. StatPearls.
- Jain, S., & Haydel, M. J. (2025). Child Intussusception. [Updated 2023 Apr 10]. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
- Weledji, E. P. (2020). Perspectives on paralytic ileus. Acute Medicine & Surgery, 7(1), e573.
- Ahmed, S., & Sharman, T. (2023). Intestinal pseudo-obstruction. In StatPearls [Internet]. StatPearls Publishing.
- Rieder, F., Zimmermann, E. M., Remzi, F. H., & Sandborn,W. J. (2013). Crohn's disease complicated by strictures: asystematic review. Gut, 62(7), 1072-1084.
- Malikowski, T., Mahmood, M., Smyrk, T., Raffals, L., & Nehra, V. (2018). Tuberculosis of the gastrointestinal tract and associated viscera. Journal of clinical tuberculosis and other mycobacterial diseases, 12, 1-8.
- Nuño-Guzmán, C. M., Marín-Contreras, M. E., Figueroa-Sánchez, M., & Corona, J. L. (2016). Gallstone ileus, clinical presentation, diagnostic and treatment approach. World journal of gastrointestinal surgery, 8(1), 65.
- Maule, W. F. (1990). Nausea and vomiting. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition.
- Jackson, P., & Cruz, M. V. (2018). Intestinal obstruction: evaluation and management. American family physician, 98(6), 362-367.
- Rosano, N., Gallo, L., Mercogliano, G., Quassone, P., Picascia, O., Catalano, M., ... & Marano, I. (2021). Ultrasound of small bowel obstruction: a pictorial review. Diagnostics, 11(4), 617.
- Lotfollahzadeh, S., Lopez, R. A., & Deppen, J. G. (2024). Appendicitis. In StatPearls [Internet]. StatPearls Publishing.
- Chung, K. T., & Shelat, V. G. (2017). Perforated peptic ulcer-an update. World journal of gastrointestinal surgery, 9(1), 1.
- Pothiawala, S., & Gogna, A. (2012). Early diagnosis of bowel obstruction and strangulation by computed tomography in emergency department. World Journal of Emergency Medicine, 3(3), 227.
- Monita, M. M., & Gonzalez, L. (2017). Acute mesenteric ischemia.
- Castera, M., Borhade, M. (2023). Fluid Management. [Updated 2022 Sep 5]. StatPearls [Internet] Treasure Island (FL): StatPearls Publishing.
- Vadivelu, N., Kodumudi, G., Leffert, L. R., Pierson, D. C., Rein, L. K., Silverman, M. S., ... & Kaye, A. D. (2023). Evolving therapeutic roles of nasogastric tubes: current concepts in clinical practice. Advances in therapy, 40(3), 828-843.
- Mthethwa, M. R., Aldous, C., & Madiba, T. E. (2021). Clinicopathological spectrum of small bowel obstruction and management outcomes in adults–experience at a regional academic hospital complex. South African Journal of Surgery, 59(3), 118-123.
- Pages-Bouic, E., Millet, I., Curros-Doyon, F., Faget, C., Fontaine, M., & Taourel, P. (2015). Acute pelvic pain in females in septic and aseptic contexts. Diagnostic and interventional imaging, 96(10), 985-995.
- Szeliga, J., & Jackowski, M. (2017). Laparoscopy in small bowel obstruction–current status–review. Videosurgery and Other Miniinvasive Techniques, 12(4), 455.
- Pawlak, M., East, B., & De Beaux, A. C. (2021). Algorithm for management of an incarcerated inguinal hernia in the emergency settings with manual reduction. Taxis, the technique and its safety. Hernia, 25(5), 1253-1258.
- Vallicelli, C., Coccolini, F., Catena, F., Ansaloni, L., Montori, G., Di Saverio, S., & Pinna, A. D. (2011). Small bowel emergency surgery: literature's review. World Journal of Emergency Surgery, 6(1), 1.
- Hussen Mostafa Adam, M., Bakhit, S., Ahmed, M. E., Almahal, M. A., Ali, H. A., Ahmed, M. O., ... & Salim, O. E. F.H. (2024). Postoperative Intravenous Fluids and Electrolytes Management After Gastrointestinal Surgery in a Sudanese Teaching Hospital: A Prospective Audit. Cureus, 16(10), e71709.
- Springer, J. E., Bailey, J. G., Davis, P. J., & Johnson, P. M. (2014). Management and outcomes of small bowel obstruction in older adult patients: a prospective cohort study. Canadian Journal of Surgery, 57(6), 379.
- Fevang, B. T. S., Fevang, J., Lie, S. A., Søreide, O., Svanes, K., & Viste, A. (2004). Long-term prognosis after operation for adhesive small bowel obstruction. Annals of surgery, 240(2), 193-201.
- Lo, O. S. H., Law, W. L., Choi, H. K., Lee, Y. M., Ho, J. W.C., & Seto, C. L. (2007). Early outcomes of surgery for small bowel obstruction: analysis of risk factors. Langenbeck's archives of surgery, 392(2), 173-178.
- Meier, R. P., de Saussure, W. O., Orci, L. A., Gutzwiller, E. M., Morel, P., Ris, F., & Schwenter, F. (2014). Clinical outcome in acute small bowel obstruction after surgical or conservative management. World journal of surgery, 38(12), 3082-3088.
- Karakas, D. Ö., Yesiltas, M., Gökçek, B., Egin, S., & Hot,S. (2019). Etiology, management, and survival of acute mechanical bowel obstruction: Five-year results of a training and research hospital in Turkey. Turkish Journal of Trauma & Emergency Surgery/Ulusal Travma ve Acil Cerrahi Dergisi, 25(3).
- Markogiannakis, H., Messaris, E., Dardamanis, D., Pararas, N., Tzertzemelis, D., Giannopoulos, P., ... & Bramis, I. (2007). Acute mechanical bowel obstruction: clinical presentation, etiology, management and outcome. World journal of gastroenterology: WJG, 13(3), 432.
- Rami Reddy, S. R., & Cappell, M. S. (2017). A systematic review of the clinical presentation, diagnosis, and treatment of small bowel obstruction. Current gastroenterology reports, 19(6), 28.
- Maung, A. A., Johnson, D. C., Piper, G. L., Barbosa, R. R., Rowell, S. E., Bokhari, F., ... & Kerwin, A. J. (2012). Evaluation and management of small-bowel obstruction: an Eastern Association for the Surgery of Trauma practice management guideline. Journal of Trauma and Acute Care Surgery, 73(5), S362-S369.
- Girma, H., Negesso, M., Tadese, J., Hussen, R., & Aweke,Z. (2021). Management outcome and its associated factors among surgically treated intestinal obstruction cases in Dilla University Referral Hospital, Southern Ethiopia. A cross-sectional study. International Journal of Surgery Open, 33, 100351.
- Pqdziwiatr, M., Budzynski, P., Stanek, M., Mattok, M., Major, P., Wierdak, M., ... & Budzynski, A. (2015). Mechanical bowel obstruction-changes in aetiology over the past 145 years: a single centre retrospective cohort study. Acta Chirurgica Belgica, 115(6), 397-403.
- Beyene, E., & Negassa, M. (2024). Causes, management outcome, and associated factors in patients admitted with a diagnosis of intestinal obstruction to Ambo University Referral Hospital: a 3-year retrospective chart review. African Health Sciences, 24(2), 348.
- Mir, S. A., Wani, R. A., Hassan, Y., Parray, F. Q., & Chowdri,N. A. (2019). Etiology and Management of Small Bowel Obstruction with Special Reference to Role of Laparoscopy A Single Centre Experience. Surgical Science, 10(04), 113.
- Olausson, M., Aerenlund, M. P., Azzam, M., Bjerke, T., Burcharth, J. F. H., Dibbern, C. B., ... & Smith, H. G. (2023). Management and short-term outcomes of patients with small bowel obstruction in Denmark: a multicentre prospective cohort study. European Journal of Trauma and Emergency Surgery, 49(2), 1121-1130.
- Choi, J., Fisher, A. T., Mulaney, B., Anand, A., Carlos, G., Stave, C. D., ... & Weiser, T. G. (2020). Safety of foregoing operation for small bowel obstruction in the virgin abdomen: systematic review and meta-analysis. Journal of the American College of Surgeons, 231(3), 368-375e1.