
Journal of Veterinary Health Science(JVHS)
ISSN: 2831-3887 | DOI: 10.33140/JVHS
Impact Factor: 0.762

Research Article - (2025) Volume 6, Issue 2
Strategic Framework for Addressing Antimicrobial Resistance: Governance Practices and Innovation in Teaching Hospitals
Received Date: Oct 17, 2025 / Accepted Date: Nov 14, 2025 / Published Date: Nov 28, 2025
Copyright: ©2025 Tatiana da Silva Campos, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Campos, T. D. S., Camargo, F. C. (2025). Strategic Framework for addressing Antimicrobial Resistance: Governance Practices and Innovation in Teaching Hospitals. J Vet Heal Sci, 6(2), 01-10.
Abstract
Introduction: Antimicrobial resistance (AMR) is the ability of microorganisms to become resistant to drugs. This resistance is a global health threat due to multifactorial factors not only in humans, but also in animals and agricultural production. The justification for the present study is related to the theme as a global health emergency in the face of the impacts of the pandemic, and the need to better understand the complex relationships between hospital governance and the fight against AMR in teaching hospitals. The objective, therefore, is to propose an empirical model on governance practices and innovations in addressing AMR.
Methods: The Convergent Care Research (CCR) method was employed, utilizing a qualitative approach with triangulation of sequentially conducted studies: a) documentary analysis, b) scoping review, and c) semi-structured interviews. The study was conducted in a large teaching hospital within Brazil's Unified Health System (SUS) in the Triângulo Mineiro region in 2023.
Results: Through the triangulation of all proposed studies, it was possible to establish an empirical theoretical model that indicates that practices related to responsiveness, evidence-based practices, and innovations, as well as hospital practices and routines, are the outputs, products, and tools proposed for addressing AMR in the researched hospital.
Conclusions: No similar proposal was identified in the literature. This is a unique proposal, the first in Latin America to strengthen the governance of public teaching hospitals in addressing AMR. It is expected that, when applying the model to public teaching hospitals, given the combination of the three practices presented—focusing on staff training and development, active surveillance and audits, and diagnostic innovation and strengthening hospital routines—controls (sensitive monitoring indicators) will signal a decline in infection rates.
Keywords
Governance, Theoretical Models, Antimicrobial Drug Resistance
Introduction
Antimicrobials are medications used to treat infections caused by bacteria, fungi, viruses, and parasites. They are essential for maintaining health in both humans and animals and are also useful for microbiological control in agricultural production. However, microorganisms can become resistant to these medications, a phenomenon known as antimicrobial resistance (AMR). In addition to the spread of resistant pathogens, AMR leads to reduced therapeutic effectiveness, increased mortality, and higher healthcare costs [1].
AMR is increasingly recognised as a global health threat. Its escalation was particularly observed in the context of the SARS- CoV-2 pandemic, covid-19. Coupled with the challenges of infection control that interfered with the prevalence of morbidity and mortality during the pandemic, viral and bacterial resistances have emerged as a global health emergency [2].
As a result of the challenges related to infection control and the prevalence of morbidity and mortality during the pandemic, viral and bacterial resistances present a significant global health crisis. This issue is intrinsically linked to the current health context and may involve accelerated patterns of AMR and a higher incidence within healthcare services [3].
In a comprehensive review study, data from the year 2019 showed the mortality rates attributable to and associated with bacterial resistance to antimicrobials by region as per the Global Burden of Disease (GBD). It was demonstrated that in 2019, 1.27 million deaths (uncertainty interval [UI] 0.911–1.71, 95%) were directly attributable to resistance. Based on a counterfactual scenario of the absence of infection, it was estimated that 4.95 million deaths (3.62–6.57) were associated with bacterial AMR. Furthermore, among the 21 regions of the GBD, Australia exhibited the lowest burden of AMR in 2019, with 6.5 deaths per 100,000 inhabitants (95% UI 4.3–9.4) attributable to AMR and 28.0 deaths per 100,000 (18.8–39.9) associated with AMR in the same year [2].
In the post-pandemic context, a quadripartite global alliance is gaining momentum, comprising the World Health Organization, World Organisation for Animal Health, United Nations Food and Agriculture Organization, and United Nations Environment Programme, which prioritise the issue of AMR. This concept, known as "One Health," represents a socio-ecological approach to human, animal, plant, and environmental health, expressed through inter-institutional commitments. Sustainable solutions are sought through a political agenda, intersectoral actions, and transdisciplinary efforts [4].
Despite governmental efforts, such as the Global Antimicrobial Resistance and Use Surveillance System (GLASS), aimed at standardising global AMR surveillance, and Brazil’s Ministry of Health strengthening programmes supporting clinicians and epidemiologists to access more accurate information on community and hospital infections, leading to the adoption of stewardship programmes for improved prescribing, significant knowledge gaps regarding innovations on the topic still persist [1,5-8].
It is noteworthy that teaching hospitals within Brazil's Unified Health System (SUS) occupy a strategic position for innovations in AMR management. These institutions serve as traditional loci of teaching-service integration, which, as part of their mission, promote the development of the teaching-research binomial to achieve qualified academic training and care [9].
Consequently, the justification for conducting the present study is linked to the theme of AMR as a global health emergency in light of the pandemic’s implications, and the need to better understand the complex relationships between hospital governance and the confrontation of AMR. There are gaps in research addressing the political agenda of AMR, its implementation, and how it has evolved in the post-pandemic context alongside healthcare services [3,5,10].
Moreover, a literature review conducted by Murray and collaborators, based on the World Health Organization’s global action plan, found gaps relating to the limitations of available conceptual models in the literature [1,2]. This fact hampers the application of operational research for public health policy management. Although operational research models are designed to optimise a specific objective criterion subject to a set of constraints, the quality of the solution depends on how well the model represents the real system [11].
Theoretical models can be characterised as a hypothetical- deductive representation of life or parts of it, aiming to understand, explain, and/or predict relationships at a specific moment in time, for specific people and places [12].
In this regard, we question: How can we contribute to the public agenda for tackling AMR within the context of teaching hospitals? What innovations have been implemented to confront antimicrobial resistance in the hospital environment? Thus, the objective is to develop an empirical theoretical model on governance practices and innovations for addressing antimicrobial resistance in a public teaching hospital.
Materials and Methods
Ethical Approval
Regarding ethical aspects, this study is part of a larger research project entitled "Convergent Care Research for the Implementation of Evidence-Based Practice among the Teams of a Public Teaching Hospital," approved on 9 June 2017, CAAE number: 64910317.6.0000.5154, and consolidated opinion number 2.110.319, from the Federal University of Triângulo Mineiro, in accordance with the resolution of the National Health Council 466/2012 [13]. Data were collected after participants understood and signed the Informed Consent Form.
Study Design
This is a Convergent Care Research (PCA) study, a qualitative approach grounded in action research [14]. It is considered that practical realities provide a vast field for knowledge construction, prioritising health actions as research objects. In this approach, the researcher seeks to integrate thought and action for the improvement of practice through interventions that are susceptible to experiential learning. It includes care activities as part of the research process, implementing actions in settings to discover realities, resolve problems, or induce innovations. Thus, fieldwork is a crucial tool for methodological development, as represented.
Regarding the study setting, according to Interministerial Ordinance No. 285, dated 24 March 2015, teaching hospitals are health establishments that belong to or are affiliated with a higher education institution (HEI), either public or private, which serve as settings for the practice of teaching activities in the health area and are certified as established by the Teaching Hospital Certification Programme [15]. It is noted that the SUS operates at various levels of governance, from local care, through municipal, microrregional, macrorregional, interstate, national, cross-border, to a global scale, with this governance being inter-federative, collaborative, participative, and network-based.
These hospitals are characterised as reference units in procedures of higher technological density (complexity) and are centres for training, teaching, and practising important health specialties, particularly for specialist medical professionals. They also contribute to processes of care innovation and technological incorporation in health. The HC-UFTM serves 27 municipalities (Map 2) that comprise the health macrorregion of Triângulo Sul in the state of Minas Gerais, corresponding to 806,000 people, as the only hospital that provides high-complexity care, entirely under the SUS. Additionally, it receives patients from other regions of Minas Gerais, amounting to a population of 800,000 people [16].

Figure 1: Map of Triângulo Sul Health Macrorregion (MG)
Source: IBGE Cities, 2020
It accounts for 73% of all medium and high complexity services in the macrorregion and 100% of high complexity services in that area, except for cancer treatment. This macrorregion comprises the following cities: Água Comprida, Araxá, Campo Florido, Campos Altos, Carneirinho, Comendador Gomes, Conceição das Alagoas, Conquista, Delta, Fronteira, Frutal, Ibiá, Itapagipe, Iturama, Limeira do Oeste, Pedrinópolis, Perdizes, Pirajuba, Planura, Pratinha, Sacramento, Santa Juliana, São Francisco de Sales, Tapira, Uberaba, União de Minas, and Veríssimo. The hospital has 306 beds across inpatient units, emergency services, and intensive therapy units. The Hospital de Clínicas da Universidade Federal do Triângulo Mineiro, HC-UFTM (FIGURE), has five annexes: Maria da Glória Outpatient Clinic, Specialties Outpatient Clinic, Paediatric Outpatient Clinic, Rehabilitation Centre, and Chemotherapy Centre, totalling 173 consulting rooms [17].
Contextual Analysis and Data Interpretation
The proposed study types were organised in a sequential and complementary manner. The first study is a documentary analysis aimed at identifying strategies for hospital governance [10]. The second consists of a scoping review to survey potential innovations for addressing AMR according to global literature [18]. The third study employed semi-structured interviews with stakeholders of the hospital to identify, according to their perspectives, the governance strategies that should be strengthened and the potential innovations [19].
The empirical-theoretical model was developed based on the triangulation of the results from the previous studies and consisted of the creation of a technical product presented to the governance of the researched hospital (FIGURE 2).

Figure 2: Convergent Care Research Conduction Scheme
The research was conducted from 18 March 2023 to November 2023.
• Documentary Analysis: A descriptive, quantitative-qualitative research approach was adopted. The research question was: how do public governance practices support the management of AMR in a teaching hospital within the Brazilian Unified Health System (SUS)? To address this, a documentary analysis was performed from 18 March to 09 April 2023 on the official website of the Hospital de Clínicas da Universidade Federal do Triângulo Mineiro, a hospital in the network of the Brazilian Hospital Services Company (EBSERH) [17]. The selection of research tabs on the website was based on an analysis of the content of the five existing tabs: access to information, governance, management at a glance, institutional documents, and communication, where it was found that the governance and institutional document tabs were related to the research topic, the management of AMR. The first step involved searching through publicly accessible electronic sources for all current free-access documents published up to March 2023, except for the “service bulletins” for which the search criterion began in 2021 due to the innovation date and time of the last document update [10,17].
• The scoping review was conducted using the PCC strategy, where the Population consisted of initiatives and innovations; Concept related to the management of AMR; and Context pertained to teaching hospitals. The descriptors used were: “Antimicrobial Resistance” “Teaching Hospitals” “Health Strategies” and “Innovation” The databases employed included: Lilacs, PubMed, Cochrane Library, Embase, Web of Science, and Scopus. Eligible articles included complete, freely accessible articles in Portuguese, English, and Spanish, published in the last ten years, from 2013 to 2023. Exclusions included review articles, editorials, letters to the editor, guidelines, research proposals, monographs, dissertations, and theses. Data collection occurred in March 2023, and the data extracted from the databases were imported into the Ryan manager from the Qatar Computing Research Institute (QCRI), a free web application available for analysis in the following order: publication date, title, and authors. The Rayyan application provides tools for managing duplicates based on research methods and keywords, recording decisions for inclusion, exclusion, or uncertainty. Removed duplicates were considered only once and were not completely discarded. The first decision-making analysis step, conducted in pairs, involved reading titles and abstracts, with uncertainties discussed in meetings for decision-making. In the next step, a full reading of the previously selected articles was performed, following the guidelines of the Prisma Extension for Scoping Reviews (Prisma-ScR): Checklist and Explanation to systematise the selection and inclusion of studies [20,21]. A manual search through reading the references of the included primary studies was also employed, and those studies meeting the defined inclusion criteria were included in the review [18].
• The stakeholders were selected based on the documents related to the documentary analysis (eligibility criterion). Organisational leaders were identified, as they were coordinators or vice-coordinators of committees, commissions, or working groups. This constituted a purposive sample. A list was compiled based on the results of the documentary analysis. Each interviewee was invited via messaging application with a brief introduction of the research and an estimation of the time required, not exceeding thirty minutes. Interviews were conducted at the most convenient time for the interviewee at the research institution, in their workplace, at a pre-scheduled time. Before beginning the interview, the approval of the Research Ethics Committee (CEP) was presented, along with a reading of the Free and Informed Consent Form (TCLE). Following the initial set of sociodemographic questions regarding professional practice and qualifications, the semi- structured questions were posed, recorded with the consent of all participants, with the author of the research serving as the interviewer. Data collection occurred from September to November 2023 [19].
• Construction of the Empirical-Theoretical Model: This was dependent on all the final results of the previous studies, as this type of model is essentially based on empirical relationships derived from a series of observed data, aiming to encompass the greatest possible representativeness of a phenomenon.
Results
Table 1 summarises the results of each study described during the methodological process
|
Types of Study |
Document Analysis |
Scoping Review |
Semi-Structured Interviews |
|
Approach |
Quantitative-Qualitative |
Review Study |
Qualitative Approach |
|
Population |
Documents on Hospital Governance available on the institutional website |
Complete scientific articles indexed in the following databases: Lilacs, PubMed, Cochrane Library, Embase, Web of Science, and Scopus |
Strategic leadership in the Hospital Organisation working with AMR |
|
Objective |
Identify public governance practices that support the confrontation of AMR in a teaching hospital within the SUS | |
Identify innovations for the management of antimicrobial resistance in teaching hospitals based on scientific production |
Identify the challenges faced in managing antimicrobial resistance and potential innovations. |
|
Main Results |
A total of 1567 documents were identified, of which 86 contained content related to addressing antimicrobial resistance. It was found that the researched hospital utilises governance practices to confront AMR. Its actions are predominantly based on assistive strategies for the prevention and control of infections. |
Resulted in a final sample of 17 articles published in indexed health journals. The absolute frequency analysis of similar terms found was: Forms and guides for prescription control ( n=02 ); Institutional committees and quality indicators ( n= 02) ; Timely Diagnostic Detection ( n= 02); Information Technology ( n= 02) ; Training and Professional Development ( n=02) ; Reinforcement of precautions and cleaning and disinfection routines (n=04); Active audits and institutional epidemiological surveys ( n= 12). |
The challenges included: a) promoting strategic management involving internal and external dialogue within the public teaching hospital; b) developing the health teams within the hospital to enhance leadership capacity in confronting antimicrobial resistance; and c) innovating processes, routines, and products in managing risks for the institution's sustainability. The innovations were grouped into: Evidence- based decision-making in services; Use of research in practice; Management of antimicrobials; Development of health teams; and Patient-Centred and Timely Care. |
|
Source: Compiled by the authors from the references of each study. Campos, et al., 2023; Campos, T.S., Camargo, F.C., 2024; Campos, Tatiana da Silva, 2024. |
|||
Table 1: Results of the Studies
The construction of the empirical theoretical model, dependent on all the final results from the previous studies, as this type of model is essentially based on empirical relationships arising from a series of observed data, aimed to encompass the greatest possible representation of a phenomenon. This is an empirical theoretical model intended to present the governance practices employed in confronting AMR in a teaching hospital (FIGURE 3).
Hospital Governance Model
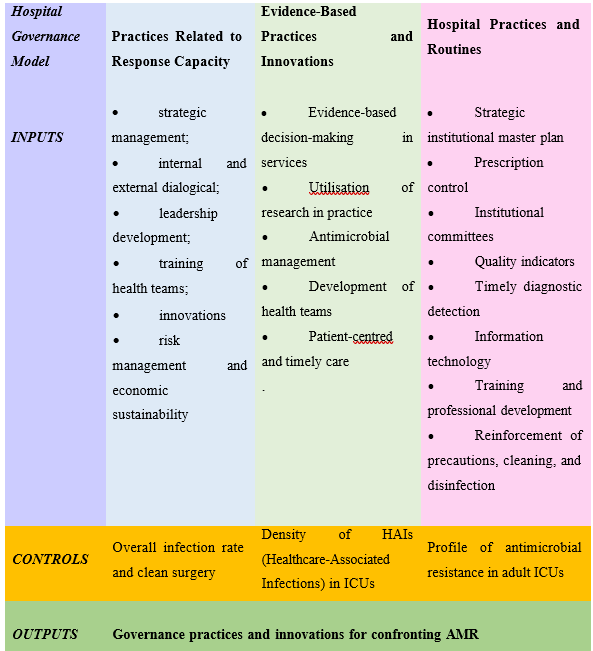
Figure 3: Strategic Framework: Empirical Theoretical Model
Source: Compiled by the authors, 2024.
The practices related to response capacity, evidence-based practices and innovations, and hospital practices and routines are the results (outputs) generated from the triangulation of the findings from the research stages (inputs).
Regarding the practices related to response capacity, their construction includes the promotion of strategic management that involves internal and external dialogical management within the public teaching hospital. This aims to strengthen communication among workers, work processes, the strategic needs of the hospital, and patient-centred care. Additionally, the development of health teams within the hospital to enhance leadership capacity in confronting AMR reflects the need for improvements in workforce sizing, employee turnover, and the retention of professionals and talent. Innovations in processes, routines, and products concerning risk management for the institution's sustainability were also highlighted. Here, the necessity of strengthening the integration of research, teaching, and assistance was emphasised as a proactive avenue for addressing the demands of the hospital institution itself, overcoming polarising aspects that comprise this relationship.
Evidence-based practices and innovations are underpinned by several pillars: they should be actions outlined in the Strategic Master Plan or other institutional planning of the hospital; there should be an internal contract developed with the hospital’s care units to agree on actions addressing antimicrobial resistance; there should be a panel for quality indicators sensitive to the theme of antimicrobial resistance, including the resistance/sensitivity profile of germs to antimicrobials; the promotion of institutional research within the hospital on this topic is essential; summarised and easily accessible reports, such as on a website, regarding research already conducted in the hospital on the subject should be available; support should be given for the development of new classes of antibiotics and drugs; and partnerships with graduate programmes at affiliated universities are recommended.
With regard to hospital practices and routines, their constitution is focused on actions such as: management of antimicrobials, aiming to strengthen hospital practice in accordance with antimicrobial stewardship, which is an antibiotic management programme; promoting pharmacotherapeutic reconciliation for antibiotic therapy; having applications that generate reports; and ensuring the control of antimicrobial release through an auditable application, timely and systematic regarding the use of antimicrobials in the hospital. There should be control for the release of antimicrobials through an adjustable application; team development through training in various modalities; development of campaigns to raise awareness among the entire hospital community, similar to patient safety campaigns, with an emphasis on hand hygiene and zero adornment; and keeping protocols regarding precautions, infection control, and other related institutional routines updated in accordance with scientific evidence and ANVISA recommendations. Patient-centred and timely care points towards perspectives such as strengthening multidisciplinary discharge orientations for patients; enhancing networked operations with shared responsibility among hospitals concerning the health of communities in their territories; alert systems; and implementing diagnostic improvements for AMR through methods such as molecular biology.
The control measures regarding the application of these practices are related to the hospital's infection indicators: overall infection rates and clean surgery, density of healthcare-associated infections (HAIs) in ICUs, and the antimicrobial resistance profile in adult ICUs, along with control data from the infection control commission related to assistance (CCIRAS).
Discussion
Reflecting on the daily operations of the hospital, as pointed out, having a local strategic agenda for confronting AMR is a crucial action. This is especially true regarding the implementation of managerial and operational practices to ensure that the work process aims at quality care [22]. Therefore, there is a need for a more participatory management style that is in constant dialogue with the hospital organisation, enhancing adherence and proactivity regarding care protocols and patient-centred care.
One study discusses that to build safer patient care, it is essential that, in addition to all healthcare professionals, management and even the patients themselves actively participate in this practice. Thus, initiatives focused on the development of teams and leadership, such as strategies for ongoing education and continuous training, act as facilitators. The proximity between leaders and their teams is another aspect that fosters a more participatory and collaborative environment [22-24].
However, understaffing undermines the quality of care provided and increases the workload, limiting the public teaching hospital's capacity to respond to AMR. The imbalance between human resources and work demand is associated with longer hospital stays, higher rates of urinary tract infections related to invasive procedures, and lower patient satisfaction with care [22,23]. The stakeholders also pointed out limitations regarding response capacity related to infrastructure, ergonomics, and biosafety. Increasingly, it is crucial for the institution's strategic agenda to focus on the working environment to minimise exposure to stressful situations, which ultimately jeopardise both the health of the workers and the care provided [25,26].
Another review study indicates that improved decision-making skills are directly related to better patient outcomes and a reduction in clinical errors. The implementation of evidence-based practices and advanced technologies results in improvements in diagnostic accuracy and care efficiency [27].
The innovative perspectives highlighted reflect a focus on improvement concerning local needs. Evidence-based decision- making in services indicates innovations ranging from action planning to technologies that provide timely monitoring of infection indicators, demonstrating that these actions optimise financial and, primarily, human resources, contributing significantly to the prevention of infection increases.
Implications for practice suggest the need for the creation of training programmes that promote knowledge about Evidence- Based Practice (PBE) and its translation into clinical contexts, as well as organisational projects that support formal leaders in this process [28].
Nonetheless, changes in processes and routines face resistance, often rooted in the culture of “this is how it's always been” The culture in public hospitals within the SUS is characterised by a rigid organisational structure and centralisation of power, resulting in competition, individualism, and difficulty in developing teamwork; a lack of interest in promoting interpersonal relationships; and disregard for the needs of workers [25,26,29].
Thus, innovations in processes and routines within Brazilian public hospitals are urgently needed, as pointed out by the stakeholders. However, there is a scarcity of scientific literature addressing innovations in the everyday practice of hospital governance. Much of the scientific output centres on technologies—such as applications and products—but little discussion exists around innovations in governance [30].
Seeing innovations as generators of solutions to public health demands, identifying the needs and demands of society regarding health services, is also challenging due to the gap between the scientific knowledge produced and its operationalisation and utilisation by society. The impact of these data lies in identifying the potential for innovation in health focused on processes [30].
Finally, financial resource limitations have been widely identified as a limiting factor for the necessary innovations to improve teaching and research care conditions in confronting AMR. Financial difficulties, throughout the national political history, have made the public health system a target for reduced government investment. This system, already penalised in recent years, had its situation worsened by the pandemic scenario in 2020 [31,32].
From this perspective, the integration of teaching-service-research, privileged in the settings of public teaching hospitals, should be valued as potential. In any case, the development of governance in teaching hospitals must be strictly aligned with the values important to patients, with the goal of providing sufficient and appropriate services in a safe and dignified manner [29]. Aligning the confrontation of AMR will only be possible if teaching hospitals assume their vocation of "teaching to care," remaining integrated with contemporary social demands, many of which are grounded in actions related to governance practices in the proposed model.
Practical Implications
It is desired that the topic be incorporated into the institutional political agenda through working groups that develop the strategic master plan, in which challenging points are diagnosed and actions proposed, with defined deadlines for the joint improvement of work processes. There are implications for training and engagement within the hospital community.
With the network management of public university hospitals, the proposal is also expected to inspire other hospitals with similar infrastructure and service profile. Given the network management and sustainability, it faces a potential measurable reduction in the rates of healthcare-associated infections and in the prevalence of multidrug-resistant microorganisms; improved efficiency in the use of antimicrobials, with reduced hospital costs, better clinical outcomes, and strengthening the integration of teaching-research- assistance, positioning the hospital as a reference in confronting AMR.
Study Limitations
Regarding the limitations of the research, they were those expected due to the nature of the adopted method: the study was conducted in a single hospital, which limits the generalisation of results. In particular, there are limitations associated with the interpretation of findings, influenced by researchers' subjectivity in translating reality, as the results depend on the understanding of the research participants. However, the intentional sampling of stakeholders (organisational leaders) may introduce bias, and in future research, it is important to incorporate the perspectives of non-leadership professionals or from other sectors (such as pharmacy or nursing). Nevertheless, the entirety of the intentional sample was achieved.
Much emphasis in the results is placed on technological innovations. Innovations in governance—such as changes in organisational culture or collaborative decision-making—while addressed, require further depth even though they are cited as challenges. This includes discussing financial limitations for the implementation of the model and how to overcome them through cost-effectiveness strategies for applying the proposed practices. Thus, this research has a significant contribution to local decision- making and to guiding the response capacity of the analysed hospital in its governance to confront AMR. This research also contributes to strengthening the political agenda and global and local agreements in the face of this growing global health threat.
7. Final Considerations and Future Studies
The proposed empirical theoretical model, built from empirical observations, literature review, and interviews with stakeholders, offers a practical framework for decision-making in hospital governance, focusing on confronting AMR. Its tripartite structure (response capacity, evidence-based practices, and hospital routines) reflects the complexity of the problem and the need for multi-level interventions, aligned with global guidelines such as "One Health."
It is expected that in the pilot application of this model, the implementation of one or more items from the three central practices—especially team training and innovations in diagnostics—will result in a decline in monitored infection indicators (e.g., HAI rates, resistance profiles). To ensure effectiveness, it is recommended that hospitals adapt the model to their local realities, prioritising: the integration of management, research, and assistance; the allocation of resources for accessible technologies; and ongoing evaluation through sensitive indicators.
As the first Latin American proposal for AMR governance in public teaching hospitals, this study fills a critical gap in the literature but also reveals transversal challenges, such as the need for sustainable funding and resistance to cultural changes. Future research proposals include evaluating the implementation of the model in other teaching hospitals, comparing pre and post-intervention results using mixed methods (qualitative and quantitative); exploring cost-effectiveness strategies for the proposed innovations, such as the use of artificial intelligence in diagnostics or partnerships with pharmaceutical industries; and investigating institutional barriers to adopting practices, including the perceptions of non-leadership professionals and the influence of regional public policies.
Finally, it is highlighted that the sustainability of the actions will depend on the alignment between institutional, national, and global agendas, reinforcing the role of teaching hospitals as centres of innovation and active vigilance in the fight against AMR.
Declarations
The authors declare that there are no relevant conflicts of interest pertaining to the content of this article. They also state that no funding was received for the conduct of this study.'Clinical trial registration number: not applicable.'
References
- World Health Organization. Global action plan on antimicrobial resistance. Geneva: WHO, 2015.
- Murray, C. J., Ikuta, K. S., Sharara, F., Swetschinski, L., Aguilar, G. R., Gray, A., ... & Tasak, N. (2022). Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. The lancet, 399(10325), 629-655.
- Aguiar, J. N., de Carvalho, I. P. S. F., Domingues, R. A. S.,Souto Maior, M. D. C. L., Luiza, V. L., Barreto, J. O. M., & Tavares, N. U. L. (2023). The evolution of Brazilian human health policies for the prevention and control of antimicrobial resistance: a scoping reviewEvolución de las políticas de prevención y control de la resistencia a los antimicrobianos desde la perspectiva de la salud humana en Brasil: revisión exploratoria. Revista Panamericana de Salud Publica= Pan American Journal of Public Health, 47, e77-e77.
- Pan American Health Organization; World Health Organization. Antimicrobial resistance. Washington, DC: PAHO: WHO, 2022.
- Corrêa, J. S., Zago, L. F., Silva-Brandão, R. R. D., Oliveira,S. M. D., Fracolli, L. A., Padoveze, M. C., & Currea, G. C.C. (2022). Antimicrobial resistance in Brazil: an integrated research agenda. Revista da Escola de Enfermagem da USP, 56, e20210589.
- Frattari, A., Savini, V., Polilli, E., Di Marco, G., Lucisano, G., Corridoni, S., ... & Parruti, G. (2019). Control of Gram- negative multi-drug resistant microorganisms in an Italian ICU: Rapid decline as a result of a multifaceted intervention, including conservative use of antibiotics. International Journal of Infectious Diseases, 84, 153-162.
- Pillonetto, M., Jordão, R. T. D. S., Andraus, G. S., Bergamo, R., Rocha, F. B., Onishi, M. C., ... & Abreu, A. L. D. (2021). The experience of implementing a national antimicrobial resistance surveillance system in Brazil. Frontiers in public health, 8, 575536.
- Godman, B., Egwuenu, A., Haque, M., Malande, O. O., Schellack, N., Kumar, S., ... & Seaton, R. A. (2021). Strategies to improve antimicrobial utilization with a special focus on developing countries. Life, 11(6), 528.
- Camargo, F. C., Iwamoto, H. H., Galvão, C. M., Monteiro, D. A. T., Goulart, M. B., & Garcia, L. A. A. (2017). Models for the implementation of evidence-based practice in hospital based nursing: A narrative review1. Texto & Contexto- Enfermagem, 26.
- Campos, T.S. et al. (2023). Public Governance Practices in the Face of Antimicrobial Resistance in a Teaching Hospital of the Unified Health System: A Documentary Analysis. Facthus Journal of Administration and Management, vol. 6, no. 1, pp. 261–285.
- Melo, F. C. C. D., Costa, R. F. R. D., & Corso, J. M. D. (2020). A conceptual model for studies on social determinants of health in Brazilian municipalities. Saúde e Sociedade, 29, e181094.
- de Souza Filho, B. A. B., Tritany, É. F., Arana, G. A. C., & Struchiner, C. J. (2023). Theoretical models: necessary reflections. Revista Brasileira de Epidemiologia, 26, e230038.
- Resolution No. 466, of December 12, 2012. (2012). Ministry of Health. Brasília, DF.
- Trentini, M. & Beltrame, V. (2006). Convergent-Care Research (PCA) Led to the Real Field of Nursing Action. Cogitare Enfermagem, 11(2).
- Ministry of Health. Interministerial Ordinance No. 285, of March 24, 2015. Redefines the Programme for the Certification of Teaching Hospitals (HE). Brasília, DF: Ministry of Health, 2015.
- Brazilian Company of Hospital Services (EBSERH). Our History. Brazilian Company of Hospital Services. Brasília, DF, 2021.
- Brazilian Company of Hospital Services – EBSERH. HC- UFTM - Hospital de Clínicas da UFTM. Brasília, DF, 2023.
- Campos, T.D.S., Camargo, F.C. (2024). Innovations in the Management of Antimicrobial Resistance in Teaching Hospitals: A Scoping Review. Public Policy & City, vol. 2, p. e1086, 2024.
- 29. Campos, Silva, T. D., (2024). Governance Practices and Innovations for Addressing Antimicrobial Resistance in a Public Teaching Hospital / Tatiana da Silva Campos. 2024. 113 p. Dissertation (Professional Master's in National Network Public Administration) — Federal University of Triângulo Mineiro, Uberaba, MG, 2024.
- Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid,(2016). Rayyan—a web and mobile app for systematic reviews. Systematic reviews, 5(1), 210.
- Peters, M. D., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., ... & Khalil, H. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI evidence synthesis, 18(10), 2119-2126.
- Santos, T. B. S., Moreira, A. L. A., Suzart, N. A., & Pinto, I. C.D. M. (2020). Gestão hospitalar no Sistema Único de Saúde: problemáticas de estudos em política, planejamento e gestão em saúde. Ciência & Saúde Coletiva, 25, 3597-3609.
- Cavalcante, E. F. D. O., Pereira, I. R. B. D. O., Leite, M. J. V. D. F., Santos, A. M. D., & Cavalcante, C. A. A. (2019). Implementation of patient safety centers and the healthcare- associated infections. Revista gaucha de enfermagem, 40, e20180306.
- Lima, K. M. S., Souza, C. S., Rocha, H. M. D. N., & Santos, I. R. A. D. (2023). Adherence of Nursing Professionals to the Bloodstream Infection Prevention Bundle. Contemporary Nursing Journal, 12, e4757.
- Ferreira, L., Barbosa, J. S. D. A., Esposti, C. D. D., & Cruz, M. M. D. (2019). Permanent Health Education in primary care: an integrative review of literature. Saúde em Debate, 43, 223-239.
- Baccin, A. A., Lucchese, V. C., Lima, A. L. D. D., Medeiros, B. V. D. S., Maliska, J. K. D. L., & Vasconcellos, S. J. L. (2023). Strategies for Coping with Stress and Engagement in Hospital Nursing Teams. Electronic Journal of Health Collection, 23(1), e11602.
- Freitas, M. D. G., Silva, É., & Soares, J. D. O. (2024).Decision-Making in Emergency Services by Nurses: A Literature Review. Nursing Brazil, 23(4), 1880–1892.
- Santos, D., Cardoso, D., Cardoso, A. F., Duque, F. M., Fernandes, B., Sousa, R. C., & Amaral, A. F. (2024). The Perception of Formal Leaders in Nursing About Evidence- Based Practice. Nursing Reference Journal, 1–8.
- Javani, A., Jamali, A., & Ghoorchian, N. G. (2023). Factors affecting the good governance in teaching hospitals: A narrative review. Medical Journal of the Islamic Republic of Iran, 37, 94.
- Oliveira, m. D., S. R., Biolchini, J. C. D. A., & Mello, R. E.S. D. (2023). Science and Technology in Favor of InnovationManagement in Public Health: A Case Study of Academic Institutions in the State of Rio de Janeiro. Asklepion: Health Information, 2(2), 38–51.
- De Melo, G. C. V., Do Nascimento, Í. C. S., Santos, A. R. S., Maia, A. J. R., & Moreira, C. S. (2020). Current Crisis in Public Health in Brazil: A Historical and Financial Reflection. XX USP International Conference in Accounting. University of São Paulo, São Paulo, SP.
- Oliveira, A. H. B. B. de, & Mendes, A. (2023). Proposals for the Restructuring of SUS Funding: A Systematic Review of the Literature. JMPHC ( Journal of Management and Primary Health Care ) ISSN 2179-6750, 15 (special issue), e039–e039.