
Archivos de Ciencia e Investigación(ADCI)
ISSN: 3068-014X | DOI: 10.33140/ADCI

Research Article - (2025) Volume 1, Issue 2
South American & Italy Impact Asbestos Mesothelioma:Time Series Reconstruction (1997-2016) and Comparison with Incidence by Age and Sex
Received Date: Mar 17, 2025 / Accepted Date: Jul 16, 2025 / Published Date: Aug 21, 2025
Copyright: ©Â©2025 Gustavo Gomez Barbieri. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Barbieri, G. G. (2025). South American & Italy Impact Asbestos Mesothelioma:Time Series Reconstruction (1997-2016) and Comparison with Incidence by Age and Sex. Arch Cienc Investig, 1(2), 01-11.
Abstract
Background: The use of asbestos is millennial. However, the use of asbestos in South America began in 1930 and peaked in 1960. Understanding how asbestos production has affected the incidence and mortality of pulmonary mesothelioma is critical in the design of public policies in developing countries.
Objectives: this study is aimed at interrupted and deslapse time series of incidence and deaths for mesothelioma in the period 1970-2009 in Italy and comparing South America incidence and mortality data.
Design, Setting and Participants: deaths for pleural cancer and mesothelioma (1997-2016) were recorded by WHO database and Virtas’s levels of asbestos’s. National incidence and mortality data were compared during the overlapping period (1930-2000).
Results: From the analysis of the Latin American Asbestos market, Brazil is the only country whose historical production of asbestos is comparable to that of Italy, having produced 89.7% (2925537 ktons) with respect to the European country, the rest of the South American countries combined produced a 0.25%. Mortality caused by mesothelioma and incident cases with certain diagnosis are overlapping, as are mortality due to pleural cancer other than mesothelioma and mesothelioma incidence with uncertain diagnosis (probable/possible).
Conclusions: this epidemiological analysis of deaths encoded as pleural tumors suggests carefully investigating space- temporal distribution before excluding them could be mesotheliomas. Some new lights have been thrown on the statistical behavior of mesothelioma mortality. Therefore, there is an underestimation and a real non-declaration of asbestos in the South American markets that could explain the mortality and incidences observed.
Keywords
Pleural Mesothelioma, Mortality, Incidence, Interrupted Time Series Regression, Paris Weinstein Regression
Introduction
Malignant mesothelioma is an aggressive asbestos-related cancer originating from the lining cells of pleural and peritoneal cavities as well as pericardium and tunica vaginalis. It is characterized by a long period of latency (30-50 years) and poor quality of life for patients. In Southamerica, regulations regarding the prevention of the use of asbestos as a coating on roofs and in civil constructions are very poorly developed. This is reflected in the lack of a record of incidence, only existing a law passed in 2000. In this year, the use of asbestos was prohibited in Chile (Decree 656106). However, asbestos-related illnesses are long- lasting, so exposed workers remain at risk of illness. Today the main cause of occupational exposure to asbestos is removal or demolition activities of asbestos in Houses, which increase in relation to emergencies or disasters and may also affect the nearby population. On the other hand, a non-working population can be exposed in their homes or places where asbestos was used, when the materials deteriorate or exceed their useful life, although this risk is much less than that faced by workers [1].
To prevent and monitor Asbestos exposition, a Mesothelioma National Register (Decreto Registro Nazzionale Mesoteliomi, 2002, Rename-Legislative Decree 277/1991 & Decree president of the council of Ministers 308/2002) was introduced by italian authorities and launches at nationwide “Asbestos mapping project” (Law 93/2001 & Ministerial decree 101/2003), which, today has identified more than 100.000 contaminated sites [3].
Materials containing Asbestos
In Chile, Asbestos has been used from 1920 to 2001 in the manufacture of multiple products, for a total amount 250 metric tons in 1930 [4]. Due to asbestos containing fire and heat resistant characteristics, it was used in many construction products such as fireproof insulation, in plumbing, in electrical products, and in structural uses. Unfortunately, the ubiquitous nature of construction products containing asbestos means that asbestos still has a significant presence in our lives.
Asbestos Consumption, Production and Exports in Latin America and the World:
The use of asbestos dates back to the time of the Romans. They used it as an important source of insulation and coating for their shops and ceramics, as well as their roofs and military weapons for their non-flammable character and for their high thermal resistance [5].
However, it was not until the industrial revolution that it became widespread and was used to cover pipes, floors, exterior walls, ceramics, flameproof suits for military use, among others. It was the origin of a number of occupational diseases and as described by Vogel (1960) "Asbestos, a mass crime in peacetime. Toxicity in the real economy”, accurate medical data on asbestosis has been available since the 1930s. The first research on the link between asbestos and lung cancer was carried out during the 1940s, while the link with mesothelioma was established in the early 1960s. As a matter of fact it has been known for more than seventy years that Asbestos is linked to fatal pathologies, which appear on a large scale [3].
Italy was one of the first countries to use it industrially in the world and it was the Latin American countries that were used as a source of raw materials, founding the asbestos market in South America encouraging the purchase and design of asbestos farms such as in the Piemonte region [8,9]. Despite this, mass production and use as suppliers of raw materials to countries from the third world increased by up to 3232% in Brazil between 1920 and 1960 and in countries such as Argentina this increased by a value of 19718 % . While Chile, Peru and Bolivia maintained a stable form despite the existing underreporting and the scarce historical information available regarding its use and naturally existing levels of asbestos [5].
In South America, the asbestos industry in South America did not begin to matter in world markets until the 1960s. Before that time, there was little production or consumption of asbestos (Figure 1). The little production that exists to fill market niches instead of satisfying the growing global applicants. Argentina, Brazil, Chile, Peru, Uruguay and Venezuela were the main South American consumers of asbestos during the first part of the 20th century. In 1960, consumption in South America was approximately 38,100 t (Figure 1). Brazil had just started production to supply its own markets, but South America depends on imports for about 65 percent of its fiber consumption. However, Brazil stood out as one of the main producers in Latin America despite the limited specialized development of the asbestos industry in each region. After a rapid rise between 1960 to 1971, the peak in its production was controlled in 1991, decreasing its production by the year 2000 and growing again in 2003 despite the restrictions imposed by various countries from the year 2000 to 2003. Meanwhile Argentina and Colombia followed in the production of asbestos, Chile and the rest of the Latin American countries extracted it and with very little processing made technologies covered with asbestos and coatings of concrete exterior walls [6]. By 1970, Argentina, Brazil, and Colombia had the most active of the asbestos-manufacturing industries in South America. Even at that, consumption was estimated to be only 99,200 t.
This study aims to describe the characteristics of the asbestos market and the measures to reduce asbestos exposure and its impact on mortality reduction compared with Italy and use these data to promote public policies regarding environmental hygiene and risk attributable to the population and exposure to asbestos.
Materials & Methods
Study in 34000 hospital outbreaks and de-functions in history Cohort study design of analytical, longitudinal and observational type during 1930 to 2018. The databases from the website were used by WHO & Virta’s to carry out this study. Before entering them, the CIE 10 coding manual was reviewed by verifying that the variable encoding was adequate. To do this, the number of incomplete data was counted, leaving out all those individuals who graduated from a hospital that did not provide information of the planned type and those cases where the forecast was not reported. For mortality analysis, we used data from death certificates recorded by WHO database incidence and mortality. WHO ’s database contains in South America deaths from 1983 to 2018 and population censuses from 1961 to 2001. In the considered period (1970-2009) causes of death were coded by 8th, 9th, and 10th versions of ICD, respectively. For selecting PT (Pleural tumor), we extracted codes 163.0 (ICD-8) for the period 1970-1979; 163.0-163.9 (ICD-9) for the period 1980- 2002; C38.4 (ICD- 10) for the period 2003-2009. For PM, code C45.0 (ICD- 10) for the period 2003-2009 was extracted. Incidence data were extracted from ReNaM. Classification and coding either of diagnoses or of exposure are defined by the Decree of the Prime Minister No. 308/2002 and national guidelines.1
To assess changes in incidence and hospital mortality, a interrupted and deslapsed time series analysis of praise-weinstein was carried out, the construction of an auto-regression function for the period 4 and , determining regression coefficients and to determine the secular trend or reject it with a value of 0.1 and a p < 0.05, all hospital discharges were considered during the year 1983 to 2018 with the diagnosis C45.0, 163.0-163.9 dividing it into 4 cohorts and compared to the diagnosis C45.0- C34.9, dividing it into four cohorts 1983-1993/ 1994-2004/ 2005-2015 and compared to the previous levels of Asbestos and periods to see if there were statistical differences between the 4 groups.
To determine the impact of the use of asbestos in Latin America and Italy and compare both regions, an epidemiological table was prepared with the data corresponding to the nominal variables of sex and region and the continuous variables of male and female mortality, as well as accumulated industrial production. from 1920 to 2000 of asbestos in world markets Virta 2003.
Subsequently, a univariate analysis was carried out where the percentiles, deciles and quartiles were calculated in order to characterize the sample under study and create a map of cataloging and impact of occupational exposure to asbestos in the countries studied. A quartile and decile variable was designed. In order to determine and calculate the point estimator and the regression coefficient between the very high exposure countries with respect to the very low exposure countries respectively, the numbers described were assigned for each of them.
And from the data prepared, a negative binomial, Poison, generalized linear and double-scale regression analysis for the best adjustment, was carried out in order to determine the causal relationship between asbestos exposure and the Latin American countries and Italy. To compare their results, a third variable was constructed whose value is the quotient between the mortality adjusted by age and sex of pleuritic mesothelioma in the Latin American country, with respect to Italy, each of these values was regressed according to the Poisson model which was adjusted using a generalized linear model to adjust the error and the optimal standard deviation for the model that will best fit the of the quartiles of asbestos consumption, based on the Asbestos consumption described later.
|
Second level classification |
Country |
Production intervals |
|
South American countries with very low level of exposure: |
Ecuador Paraguay Venezuela Bolivia |
Very low consumption (< 75.87 tons)=1 |
|
South American countries with low levels of exposure: |
Colombia Argentina |
Low consumption (between 75.87 and 453.681 tons)=2 |
|
South American countries with medium level of exposure: |
Chile Perú |
Moderate consumption (between 453,681 and 2955,078 tons)=3 |
|
South American countries with a high level of exposure: |
Brasil Uruguay Italia* |
High consumption (> 2955,078 tons)=4 |
*Italy is not a Latin American country but it is the reference point used in this business.
Results
The statistical trend of Asbestos consumption in the world has highlighted a sustained exponential increase between the years 1900 and 1980, a period which coincides with the first 2 world wars. The countries that had the highest production of asbestos in the world were, for more than 80 years, Russia, Canada, China, Italy and the United States, which represented 92.75% of world production (Canada is the country which contributed the most to global asbestos production). production with 42.60%) therefore the countries that have presented by far the highest mortality rate and incidence of mesothelioma and incidence of tumors are the countries with the highest degree of industrialization, in this particular case Russia and Canada have the highest rates of Lung Cancer, Breast Cancer, Ovarian Cancer and Mesothelioma (GLOBOCAN; 2020). On the other hand, the country of Italy has one of the highest cumulative mortality and incidence rates in all of Europe; since the major asbestos mining activities in Europe were located in Piedmont, Veneto and Lombardy, replaced starting from the 1950s by the chrysolite mines of Canada, which reached historic world productions (66672965 tonnes) well above those of Italy, a which had been delegated fourth place in the production of asbestos in the world market. Table 1.
The asbestos market in South America underwent very late changes in the production and exploitation of asbestos, maintaining the artisanal production of chrysolite fibers in mines associated with the exploitation of other types of metals such as Nickel, Chromium, Copper, which did not present regular and industrial-scale exploitation as first and second world countries have done, however, they have shown mortality and incidence rates that are not as high as those of industrial countries but significant in the number and severity of cases detected. It should be noted that many of these Latin American countries do not report all of their asbestos production, so there is under-reporting of production, imports and exports in the asbestos market. Indeed, it must be taken into account that when comparing existing data on the levels of consumption, import and export of this mineral, it is necessary to take into account this existing under-recorded data (Figure 3).
Therefore, Brazil has developed an economic doctrine based on the T-Ford model with an industrial development similar to that of European countries, demonstrating mortality and incidence levels similar to those of industrialized countries but not higher than them; being that Brazil has 89% of the historical production of asbestos compared to Italy, (See table N°1) and Figures 2 and 3.
Italy contributes 2% to the world production of asbestos, a figure that earned it among the countries that most developed the asbestos industry until 2003, the year in which the production of asbestos and its derivatives was banned. throughout the national territory. high incidence and mortality rate of pleural mesothelioma in that country. Countries that have reported low exposure to asbestos, such as Bolivia, Venezuela and Ecuador, have presented an artisanal industrial development of asbestos, with the aim of exporting the raw material.
Venezuela presented the highest incidence of pleural mesothelioma in men with 10 deaths. An industrial production of 75.87 ktons and with an Odds Ratio of 0.3492 with a confidence interval of [0.347 - 0.350], while in women there were 11 deaths, the incidence of pleural mesothelioma had an Odds Ratio of 0.8991 with a range of [0.8994 - 0.90], while other mesothelioma tumors had an Odds Ratio of [0.59-0.76]. General mortality of 16 deaths at once Ecuador had an industrial production of 31.09 kton and the female incidence in pleural mesothelioma, 10 deaths, an Odds Ratio of S with a confidence interval of [0.255 - 0.258], the male incidence in pleural mesothelioma had had 9 deaths, an Odds Ratio of 0.2468 with a confidence interval of [0.245 - 0.248].
Paraguay had an industrial production of 4.96 kton and a female incidence of pleural mesothelioma with 1 death, an Odds Ratio of 0.44 in a confidence interval of [0.438 - 0.442], the male incidence of pleural mesothelioma had 2 deaths, an Odds Ratio of 0.0743, and a confidence interval of [0.0726 - 0.0756].
Bolivia had an industrial production of 227,836 kton, the female incidence of pleural mesothelioma had an Odds Ratio of 0.5756 and a confidence interval of [0.574 - 0.577], the male incidence had an Odds Ratio of 0.257 and a confidence interval of confidence level of [0.255 - 0.258]. Argentina had an industrial production of 453,681 ktons. female incidence for pleural mesothelioma 188 deaths for Odds Ratio 0.6831 and confidence interval [0.681 - 0.684] in male incidence in the same disease with 187 deaths and Odds Ratio of 0.6285 and confidence interval of [0.626 - 0.630]. Colombia had an industrial production of 342.9312 ktons with a female incidence in pleural mesothelioma of 234 deaths and Odds Ratio of 0.571 and confidence interval [0.569 - 0.572], in male incidence in the same disease with 352 deaths Odds Ratio of 0.5663 and confidence interval of [0.564 -0.567].
Chile had an industrial production of 845,882 ktons with female incidence in pleural mesothelioma of 96 deaths Odds Ratio of 0.613 and confidence interval [0.612 - 0.615] and confidence interval in male incidence in the same disease with 219 deaths and Odds Ratio of 0.577 and interval confidence level of [0.575 - 0.579], its crude mortality rate is 3.04 in men and 2.06 in women. Peru had an industrial production of 844,586 ktons with female incidence in pleural mesothelioma with 59 deaths with Odds Ratio of 0.46 and confidence interval [0.461 - 0.464], in men with incidence in the same disease 55 deaths with Odds Ratio of 0.429 and confidence interval of [0.427 - 0.431].
Brazil had an industrial production of 2925537 ktons with female incidence in pleural mesothelioma with 214 deaths and Odds Ratio of 0.657 and confidence interval [0.656 - 0.659], in male incidence in the same disease with 367 deaths and Odds Ratio of 0, 6329 and confidence interval of [0.631 - 0.634].
Uruguay had an industrial production of 30374,964 ktons with female incidence in pleural mesothelioma with 20 deaths and Odds Ratio of 0.408 and confidence interval [0.406 - 0.409], in male incidence in the same disease with 34 deaths and Odds Ratio of 0.378 and confidence interval of [0.376 - 0.379].
Italy has an industrial production of 3289492 ktons, this is the reference country therefore it has no associated Odds Ratio and confidence interval, its APC is 0.3 in men and 1.51 in women. In men there were 11,329 deaths and in women 3,379 deaths.
From Price-Weinstein time series analysis, a secular trend in female mesothelioma mortality in Chile of 41.7% per year was observed with a p-value <0.004 and a confidence interval of [0.14 - 0, 68], the secular trend has remained constant. Regarding mortality from male mesothelioma in Chile, a break in the secular trend was observed with a Rho = -0.023 with an increase of 116.39% with up value < 0.0001 and a confidence interval of [0.75 - 1.57], comparing it with the female mortality from As regards cancer, in Italy an increase of 329.16% per year was observed and with a p value < 0.0001, while in males the mortality from pleuritic mesothelioma is of 767.2% with a p value < 0.0001 and a confidence interval of [5.82 - 9.51]. See attachment 1.
Regarding the table of the value of incident cases of Pleural Mesothelioma from 2018 to 2040, an increase of 17.3% will be observed in the group of countries with the highest production of asbestos (Brazil, Italy, Uruguay).


Table Nº1: Historic Asbestos’s Production in World
Figure 2: Virta’s Production World Mundial production Asbestos. The peak of production in 1980 of Asbestos Generate Breakout
South American countries with very low level of exposure:
Ecuador
Paraguay
Bolivia
The Odds Ratio of these countries was 0.02849 with a confidence interval of [0.015 - 0.041], the constant of 1.3c with t <0.007, the chi square is very significant and the R square is 63.75%. In the generalized linear model of male deaths, the Poisson coefficient is 0.028, the Regression coefficient of Asbestos consumption according to deaths was 34.04% (significant) with a confidence interval of [31.4% - 36.6%]. In the case of women, the general linearized model showed a regression coefficient of Asbestos consumption of 13.05% (not significant), the Poisson coefficient is 0.018 with a confidence interval of [0.0034 - 0.033]. the p value is 0.016 for the Poisson Constant and the Regression Coefficient.
South American Countries with Low Level of Exposure
Colombia
Argentina
In Women, the Poisson Regression Coefficient for these countries is 0.0088 and the confidence interval is [0.0066 - 0.011]. In Men, the Poisson's Ratio is 0.0057 with a confidence interval of [0.0041 - 0.0073].
Latin American countries with medium level of exposure:
Chile
Perú
In Men, the Poisson Regression Coefficient is 1.346 and the confidence interval is [1.0500 - 1.634]. In Women, the Poisson's Ratio is 0.474 with a confidence interval of [0.158 - 0.790].
Latin American countries with high level of exposure:
Brasil
Uruguay
In Men, the Poisson Regression Coefficient is -0,0056 and the confidence interval is [-0,0065 - -0,0048]. In Women, the Poisson's Ratio is -0,0056 with a confidence interval of {-0,0077 - -0,0045].
Italia* demostrate too high incidence of the all countries with a acumulate incidence 13381 cases both male and female and a letalithy and mortality 2500 cases, approximately (2500/13381) and 2,02 mors/100000habs.
Graph Nº1 Historic Brazilian Production Asbesto

Figure 1: The Growth Rate and Increase in Asbesto Production Market Response a Political Brazilian Goals and Bases Program, the Industry Received a Boost bout $9.2 Million was Invested by the Government to Increase Production (Clifton, 1973).

Figure 2: Global Distribution and Production in Market of Asbesto 1970-1979
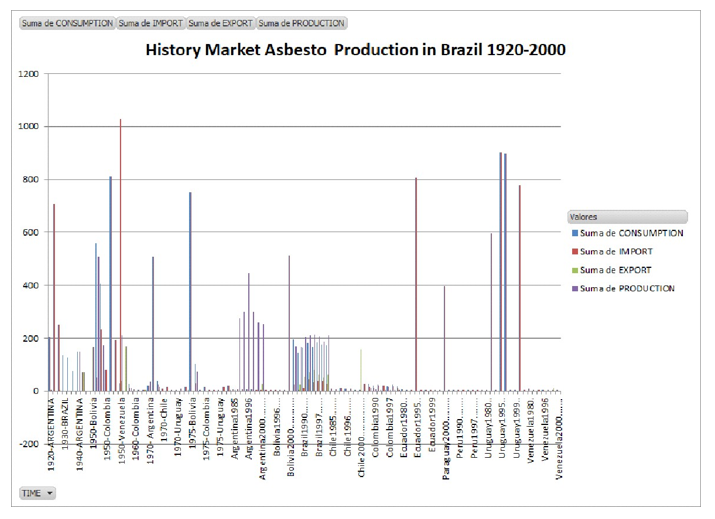
Figure 3: Historical Production of Asbestos in Latin America between 1920 and 2000
|
Yea r |
Brazil, Goiania : Male |
Brazil, Goiania : Female |
Chile, Valdi via : Male |
Chil e, Val divi a : Fem ale |
Colo mbia, Cali : Male |
Colombi a, Cali : Female |
Ecuado r, Quito : Male |
Ecuado r, Quito : Female |
|
198 3 |
- |
- |
- |
- |
23.59 |
9.83 |
- |
- |
|
198 4 |
- |
- |
- |
- |
22.59 |
7.41 |
- |
- |
|
198 5 |
- |
- |
- |
- |
18.40 |
6.03 |
8.52 |
2.13 |
|
198 6 |
- |
- |
- |
- |
23.43 |
12.58 |
9.31 |
5.39 |
|
198 7 |
- |
- |
- |
- |
25.00 |
10.72 |
7.88 |
3.85 |
|
198 8 |
- |
- |
- |
- |
22.51 |
9.57 |
7.49 |
2.05 |
|
198 9 |
- |
- |
- |
- |
24.12 |
9.09 |
12.62 |
5.72 |
|
199 0 |
- |
- |
- |
- |
21.08 |
8.59 |
9.17 |
3.55 |
|
199 1 |
- |
- |
- |
- |
23.90 |
9.29 |
10.23 |
2.55 |
|
199 2 |
- |
- |
- |
- |
22.96 |
10.58 |
13.56 |
4.78 |
|
199 3 |
18.53 |
9.63 |
- |
- |
21.49 |
8.57 |
7.78 |
2.78 |
|
199 4 |
19.92 |
6.44 |
- |
- |
22.19 |
8.28 |
8.61 |
4.79 |
|
199 5 |
26.47 |
8.53 |
- |
- |
22.98 |
10.01 |
7.12 |
4.69 |
|
199 6 |
18.21 |
8.30 |
- |
- |
25.06 |
8.95 |
8.79 |
4.88 |
|
199 7 |
22.30 |
7.95 |
- |
- |
17.95 |
9.76 |
11.61 |
4.95 |
|
199 8 |
21.99 |
8.16 |
9.34 |
5.50 |
19.49 |
7.75 |
6.48 |
5.34 |
|
199 9 |
23.79 |
10.93 |
8.61 |
7.56 |
27.34 |
11.39 |
5.58 |
4.23 |
|
200 0 |
22.46 |
10.53 |
18.34 |
3.61 |
19.10 |
8.71 |
9.56 |
4.36 |
|
200 1 |
22.55 |
10.26 |
12.09 |
2.44 |
21.68 |
10.40 |
7.68 |
3.14 |
|
200 2 |
22.05 |
12.71 |
7.71 |
4.20 |
20.03 |
8.88 |
9.92 |
3.66 |
|
200 3 |
28.23 |
7.62 |
10.23 |
3.35 |
18.54 |
8.99 |
7.89 |
6.03 |
|
200 4 |
24.59 |
12.34 |
12.63 |
3.19 |
18.08 |
9.29 |
7.55 |
5.56 |
|
200 5 |
28.87 |
14.17 |
10.03 |
3.26 |
22.25 |
8.94 |
10.53 |
5.59 |
|
200 6 |
27.52 |
13.78 |
11.93 |
7.15 |
19.10 |
8.49 |
7.02 |
6.65 |
|
200 7 |
28.11 |
13.69 |
7.86 |
4.25 |
17.31 |
8.96 |
8.95 |
7.06 |
|
200 8 |
29.29 |
10.24 |
12.02 |
5.04 |
16.08 |
6.95 |
7.86 |
5.50 |
|
200 9 |
18.48 |
13.41 |
10.39 |
2.02 |
14.41 |
8.67 |
8.29 |
6.50 |
|
201 0 |
24.49 |
13.50 |
8.38 |
4.96 |
12.69 |
7.68 |
8.70 |
5.45 |
|
201 1 |
19.04 |
12.36 |
12.04 |
6.41 |
12.92 |
9.05 |
8.96 |
5.83 |
|
201 2 |
16.07 |
11.09 |
8.93 |
4.97 |
13.51 |
7.48 |
6.37 |
6.30 |
Table Nº2: Incidence Mesothelioma Cancer in South America
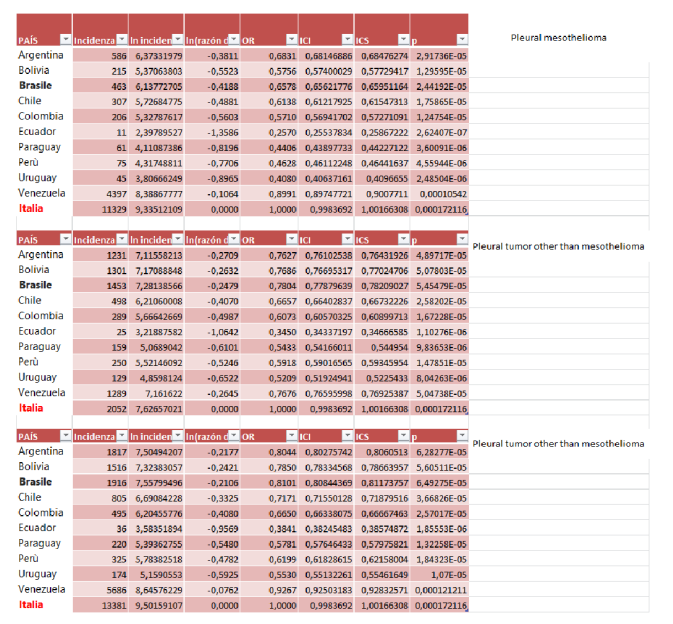
Table N°3: Incidence OR’s Poison Model from Mesothelioma in Italy and South America

Figure 3: Paris Weinstein time Series Chile-Italy Death 1996-2050. Female Mesothelioma In Italy Mortality are Increased with More Intensity Like the Male Mortality
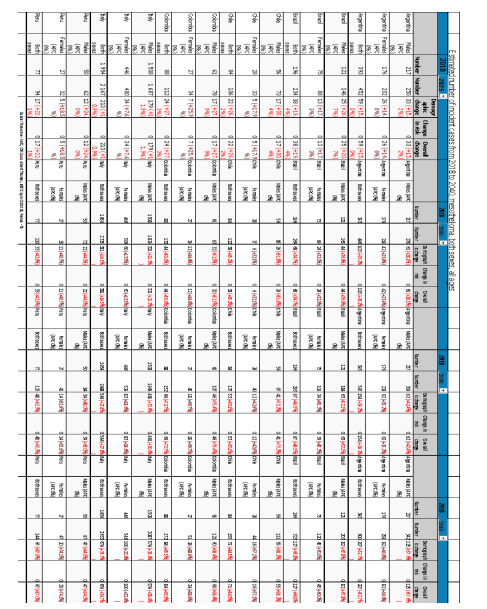
Table N°3: Incidence Forecast from Mesothelioma in Italy and South America
Countries that will have a greater impact in the coming decades are Chile, Brazil, Argentina and Peru. Provided communities with resources when necessary to completely remove asbestos from their homes and compensate families for the damages
Discussion
Despite the fact that 80 years have passed since the discovery of the association between pleuric mesothelioma and asbestos and that there are prohibitions on the production of asbestos, countries with a moderate to low level of human development such as South American countries despite presenting decrees and Laws that prohibit their production and use and force their removal continue to produce their products for other social reasons and without proper surveillance and removal of asbestos constructions [7].
The effect of asbestos removal can be seen in the projections based on the cumulative incidence and mortality from 1997 to 2018, where deaths in both men and women will increase by 32 and 75% in South American countries while in Italy implementing a broad effective policy will increase by 18 and 32%. The country that will be most violently affected will be Chile and Peru given the high exposure to asbestos, the ineffective measures in the removal that have begun to change and the earthquakes and seismic movements that cause the dispersion and dissemination of asbestos in the atmosphere and that fall on the populations [8-10].
Analyzing in parallel and diagnostic peace through monitoring programs and professional services, it is necessary to have an account of the treatment costs and management and monitoring of health care services, which are very important for the diagnosis and health services. Therefore, it is necessary to measure concrete in the case that at its time was not constructed with asbestos: so that it is necessary to identify the construction carried out in the period in which asbestos is imported or produced in the country, when an inspection must be carried out. In this construction and quality comes the presence of asbestos exposed, implement policies to remove or isolate such materials from the home (depending on where it is located) [11]. How do they do it in South America ?
In South America is not a state policy to see the use of asbestos and how to prevent the incidence and mortality of pleuritic mesothelioma, and data obtained show that it does register an increase in the incidence and mortality of pleuritic mesothelioma (incidence and mortality) in the population. In Latin America and Italy, saying that there is no rigorous control over the prohibition of this material, because of the resistance of part of the asbestos industry to ceasing production because it is a very economical and easy material. The product is designed to resist economical asbestos removal because it is an inexpensive product. Another worker in your area is the lack of control from part of the authority of the asbestos management of buildings, but the worker who has made the greatest impact on your current problem is the lack of knowledge from part of the general population of asbestos risks, there are many constructions based on asbestos that are not in the state of still removed or sealed and of which the population is not aware of the danger it represents or of its very existence, so there is low social pressure to ask for its use to cease. of asbestos because of social ignorance. Some buildings are very old and eliminating or sealing the asbestos is a logistical and financial challenge that is often ignored by optimizing resources, abandoning this family because of technical problems in the realization of the intervention. This can also be verified because of the lack of technology to effect the removal or sealing of the asbestos in the case [7,12,13].
As regards real life, the total of 616 deaths registered in the system of the Department of Statistics and Health Information rose between 1997 and 2016; 94.6% of the total deaths are attributable to asbestos. The total number of deaths recorded in Lung Canker is estimated to be a 9:1 ratio for deaths caused by asbestos and mesothelioma and Lung Cancer; That is, of its 34,670 deaths registered between 2001 and 2016, there were a total of 3,247 deaths attributed to exposure to asbestos, of which 1/RR were preventable [6].
We avoid the fact that in Chile it is overall developing almost 1,925 causes of professional exposure to asbestos in a period of 20 years, we avoid the cost of treatment equivalent to U$ 143,110,275,000 dollars, and consider [14].
Conclusion
Death from Mesothelioma and lung cancer is attributable to all asbestos. Asbestos is not responsible only for lung cancer and mesothelioma, but also for other diseases such as laryngeal cancer or ovarian cancer, but it is likely that a fraction of deaths and incidents of these tumors are not present. This data identifies the cause if explained by exposure to asbestos.
When confronting the death of mesothelioma in Italy, it is possible to recover the death of the person who has seen a long time, with less probability of dying due to exposure to all asbestos (respect all the children have died in the past 55 and 74 years),because there is a decrease and in the rate of tests carried out. Pleura biopsy cannot be performed in peace and age over 75 years but is contraindicated. The increase in the probability of failure in mesothelioma due to exposure to asbestos is less than 30% in those who are exposed to air. The expected increase in the mortality rate in Italy and Cile should be an increase of 30.3% in Chile and 40.1% of deaths in Italy does not mean the existence of 100% restrictions on the use of asbestos in everywhere type of professional attention is necessary for the State to ensure that all asbestos is removed and treated to ensure that all asbestos is exposed to 0%. The activity that presents the largest risk is the building and civil operations that do not include agriculture as sources of professional and professional expertise.
References
- Florida Department of Environmental Protection. Asbestos FAQ. (2019, January 25). Retrieved from https://floridadep. gov/air/permitting-compliance/content/asbestos-faq National Cancer
- National Cancer Institute. (2017, June 7). Asbestos Exposure and Cancer Risk.
- Hernandez-Blanquisett A, Alvarez-Londono A, Martinez- Avila MC, Covo-Camacho S, Quintero-Carreno V.Asbestos and cancer in Latin America and the Caribbean: we may zhave won some battles, but definitely not the war. J Public Health Res. 2021 Nov 28;11(2):2549. doi: 10.4081/ jphr.2021.2549. PMID: 34839650; PMCID: PMC8958443..
- El, Asbesto D, Diputado C, Dowling CV. Informe de Apoyo político y [Internet]. Ciperchile.cl. [cited 2023 Nov 3].
- Virta RL. Asbestos [Internet]. Kirk-Othmer Encyclopedia of Chemical Technology. Wiley; 2002.
- Fibras Grises de Muerte [Internet]. Avida.es.
- Cogliano, V. J., Baan, R., Straif, K., Grosse, Y., Lauby- Secretan, B., El Ghissassi, F., ... & Wild, C. P. (2011). Preventable exposures associated with human cancers. Journal of the National Cancer Institute, 103(24), 1827- 1839.
- Martini D. LE MALATTIE ASBESTO CORRELATE[Internet]. Inail.it. 2023 [citado el 1 de enero de 2024]. Disponible en.
- Ministro Montes encabeza lanzamiento del plan de recambio de techumbres de asbesto en la región de Valparaíso [Internet].
- Ministro Montes lanza plan para retirar techumbres de asbesto en mil blocks de viviendas sociales [Internet].
- Ramos-Bonilla, J. P., Cely-García, M. F., Giraldo, M., Comba, P., Terracini, B., Pasetto, R., ... & Silva, Y. A. (2019). An asbestos contaminated town in the vicinity of an asbestos-cement facility: The case study of Sibaté, Colombia. 108464.
- Algranti, E., Ramos-Bonilla, J. P., Terracini, B., Santana,V. S., Comba, P., Pasetto, R., ... & Marsili, D. (2019). Prevention of asbestos exposure in Latin America within a global public health perspective. Annals of global health, 85(1), 49.
- Accinelli, R. A., & López, L. M. (2017). El asbesto, una epidemia todavía por controlar. Gaceta Sanitaria, 31, 365- 367.
- Pasetto, R., Terracini, B., Marsili, D., & Comba, P. (2014). Occupational burden of asbestos-related cancer in Argentina, Brazil, Colombia, and Mexico. Annals of global health, 80(4), 263-268.
- Federica, P., Sergio, M., Sergio, B., Taddei, D., Lonigro, I., & Massaro, C. (2021). Guidelines for classifying and managing asbestos-containing waste.
- Martini D. LE MALATTIE ASBESTO CORRELATE[Internet]. Inail.it. 2023 [citado el 1 de enero de 2024]. Disponible en: https://inail.it/cs/internet/docs/alg-pubbl- le-malattie-asbesto-correlate-2023_6443200144304.pdf Ministro Montes encabeza.
- Ministro Montes encabeza lanzamiento del plan de recambio de techumbres de asbesto en la región de Valparaíso [Internet]. Radio Festival. [citado el 1 de enero de 2024]. Disponible en: https://www.radiofestival.cl/ministro- montes-encabeza-lanzamiento-del-plan-de-recambio-de- techumbres-de-asbesto-en-la-region-de-valparaiso/
- Suarez Hernandez, P. (2000). La problemática del asbesto en Chile (Doctoral dissertation, Universidad Academia de Humanismo Cristiano).
- Chu, Q. S., Piccirillo, M. C., Greillier, L., Grosso, F., Lo Russo, G., Florescu, M., ... & Seymour, L. (2023). IND227 phase III (P3) study of cisplatin/pemetrexed (CP) with or without pembrolizumab (pembro) in patients (pts) with malignant pleural mesothelioma (PM): A CCTG, NCIN, and IFCT trial.