
Journal of Economic Research & Reviews(JERR)
ISSN: 2771-7763 | DOI: 10.33140/JERR
Impact Factor: 1.3


Research Article - (2025) Volume 5, Issue 2
Socio-Economic Related Inequalities in the Utilization of Family Planning Services among Women in Zambia
2Bergen Centre for Ethics and Priority Setting, Bergen, Norway
3Chr. Michelson Institute, Bergen, Norway
Received Date: Sep 17, 2025 / Accepted Date: Nov 08, 2024 / Published Date: May 09, 2025
Copyright: ©©2025 Ndhlovu Simangaliso, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Simangaliso, N., Bulawayo, M., Mweemba, C., Hangoma, P. (2025). Socio-Economic Related Inequalities in the Utilization of Family Planning Services among Women in Zambia. J Eco Res & Rev, 5(2), 01-12.
Abstract
Background While a large literature documents inequality in healthcare utilization in Zambia, and the rest of sub-Saharan Africa, there has been limited focus on the examination of inequalities in family planning use and in general has increased, health inequalities persist. Similarly, despite the increase in utilization of family planning services from 15% in 1992 to 48% in 2018, the increase has not been equally shared in the population. We examine drivers of socio-economic related inequalities in utilization of family planning services among women of childbearing age in Zambia.
Methods Using secondary data from the 2018 Zambia Demographic and Health Survey (ZDHS), concentration curves are applied to examine how pro-poor and pro-rich the distribution of family planning is. A Blinder-Oaxaca decomposition analysis is conducted to decompose the rural-urban differences in the utilization of family planning services among women of reproductive age.
Results Use of family planning services was unequally concentrated. The results are mainly driven by inequalities among rural women of childbearing age as the distribution of family planning use was more concentrated among the urban women of childbearing age. In addition to family planning use being more unequal in rural areas, the proportion of women who use family planning services is 2.069 percentage points lower than in urban areas. The factors accounting for the gap between rural and urban use of family planning, with a tendency to increase it, include richest wealth group (79.76%), richer wealth group (41.63), secondary education (49.69%) and age-group of 45-49 years (48.60%). Some factors act to moderate, or reduce this gap and have negative contribution on family planning use. These include women with 7 and more children (-47.61%), being married (-26.04%), 40-44 years (-94.80%), primary education (-99.51%) and poorer wealth group (-40.20%).
Conclusion Despite progress in the utilisation of family planning services, socioeconomic inequalities have persisted, primarily in rural areas. Interventions to increase family planning use should aim at addressing rural socioeconomic disadvantage, with programs targeting poor women and those with low levels of education. Narrowing the rural-urban gap in family planning use should focus on improving wealth and education of rural women.
Keywords
Family Planning, Socio-Economic, Inequalities, Women of Childbearing Age, ZambiaBackground
Family Planning refers to working out a plan by a couple on when and how many children to have and how to prevent unwanted pregnancies. It saves the lives of both the woman and the new born and preserves their health (UNFPA, 2018). Despite advances in the provision of effective modern family planning services to women of childbearing age living in sub-Saharan Africa, Zambia inclusive, the prevalence of modern family planning was at 43% (WHO, 2011). Limited use of family planning services is attributable to low levels of education among women of reproductive age, lack of women’s empowerment or due to scarce financial resources and poverty (UNFPA, 2018).
Despite the increase in modern contraceptive use in Zambia from 15% in 1992 to 48% in 2018, it is not certain if everyone or only the well-offs are benefiting from this progress. Despite efforts by the Zambian government to intergrate family planning services into reproductive health services, maternal and child health services and safe motherhood, socioeconomic inequalities in family planning use have persisted primarily in rural areas [1,2]. Globally, the greatest burden of socioeconomic inequalities in family planning utilization lies on the disadvantaged and poor populations of women of reproductive age. There are significant differences in the use of family planning services between urban and rural areas of sub-Sahara Africa because family planning information and services were more often used by the urban women, wealthier households and empowerment less important in determining family planning utilization. Some of the prominent factors among the rural-urban variations in family planning use include low levels of education and lack of wealth [3-5].
Most studies have documented inequalities in healthcare utilization in Zambia, and the rest of sub-Saharan Africa (Phiri & Ataguba (2014). There is limited literature focusing on inequalities and decompostion of the factors driving differences in family planning use. The literature further shows that there has been major improvement in healthcare utilization in Zambia in many dimensions, but also with increase in inequalities (Phiri & Ataguba (2014). An examination of socioeconomic related inequalities in utilization of family planning services is necessary to fully understand why the rural women of childbearing age were using less family planning services compared to their urban counterparts. This is despite the various strategies and policy measures that the Zambian government implemented, such as strengthening integrated reproductive health services, as well as supporting, promoting and strengthening health education and promotion [6,7]. Such examination of socioeconomic related inequalities is essential to inform the design of effective policy interventions seeking to improve and promote increase in utilization of family planning services. Further, this study through the Ministry of Health will help policy makers to come up with deliberate policies to monitor the delivery of family planning services such as monitoring and evaluation strategies and measures for all health facilities as a supervisory tool for improving access and utilization of family planning services. The aim of the present study is to examine socioeconomic related inequalities in utilization of family planning services among women of childbearing age in Zambia.
Methods
The setting of this study is Zambia, a country in sub-Saharan Africa with an estimated population of 17million of which 40 percent is urban. We conducted a cross-sectional analysis using data from the 2018 Zambia Demographic and Health Survey (ZDHS). The sample comprised of 9, 128 women of childbearing age from 15 – 19 years in Zambia. The sample included non-pregnant women who were sexually active (n = 9,128) because they are likely to use family planning services. It excluded women of childbearing age from 15–49 years who were not sexually active (3,628) because they were not using family planning at the time of the survey. Family planning use was constructed from the question that asks women that reported using any form of family planning during the 2018 Zambia Demographic and Health survey. Demographic factors of interest included type of residence (urban vs. rural), age (15-19, 20-24, 25-29, 30-34, 35-39, 40-44, 45-49), number of children (none, 1-3, 4-6, 7+), and marital status (married, not married). Socioeconomic factors included educational attainment (no education, primary, secondary, tertiary), and quintile of socioeconomic status (poorest, poor, middle, richer, richest).
We began by first assessing the factors associated with family planning use. A logistic regression model was used, reporting marginal effects. In this instance, point estimates are reported as the probabilities and percentages along with the corresponding 95 percent confidence intervals. To examine inequalities in family planning use, we employed a number of methods. First, concentration curves and indices were calculated to explain the distribution of family planning use between the rural and urban populations. The concentration curve shows the cumulative share of family planning utilization between the rural and urban women of childbearing age. If the concentration curve lies above the 45° line, the distribution of family planning use is said to be and examined how pro-poor. If it is below the 45° line, then the distribution is pro-rich, or favoring the rich.
Second, we assessed the gap in family planning use between the rural and urban women of reproductive age. The Oaxaca-blinder decomposition method was employed to examine what factors accounted for this rural-urban gap. The gap was decomposed into that part that was due to group differences in the magnitudes or levels of the factors determining family planning use (determinants) and the differences in the effects or impact, as opposed to level, of these determinants. The part which looks at levels is called the endowment effect. The differences due to effects can be seen as the coefficient effect. It looks at how even if rural and urban area may have the same level of determinants, say health workers, but the effective of these determinants could be different between rural and urban areas. There is also an interaction term which measures the simultaneous effect of differences in the endowments and coefficients. Concentration curves and Oaxaca-blinder decomposition were generated using Stata version 14 (Stata, College Station, TX, USA).
Ethical Review
Ethical clearance and approval were obtained from the University of Zambia Biomedical Research Ethics Committee (UNZABREC, Ref: 013-08-18) and permission was sought from the Zambia Statistics Agency (ZSA), Lusaka. The clients did not accrue any direct benefit from this study. However, the results of their responses would be used to come up with recommendations to guide resource allocation decisions for health planners, administrators and policy makers. The results will also offer insights on the need to ensure the provision of effective family planning services through developing appropriate structures and instituting enduring management capabilities as a platform for effective utilization.
Results
Socio-Demographic Data
The participants for this study included 9, 128 women of childbearing age out of which 7, 398 (81.05%) were married and 6, 684 (73.23%) reported using family planning. A total of 5, 889 (64.52%) of these women were from the urban region. About 31.44% of the study participants had at least attained secondary school. Table 1 below provides a summary of these results.
|
Variable |
Category |
Proportion (%) |
|
Age |
Age range (years) |
|
|
|
15 – 19 years |
465 (5.09%) |
|
|
20 – 24 years |
1, 571 (17.21%) |
|
|
25 – 29 years |
1, 709 (18.72%) |
|
|
30 – 34 years |
1, 688 (18.49%) |
|
|
35 – 39 years |
1, 554 (17.02%) |
|
|
40 – 44 years |
1, 228 (13.45%) |
|
|
45 – 49 years |
913 (10.00%) |
|
Level of Education |
No education |
998 (10.93%) |
|
|
Primary |
4, 783 (52.40%) |
|
|
Secondary |
2, 870 (31.44%) |
|
|
Tertiary |
477 (5.23%) |
|
Marital status |
Not married |
1, 730 (18.95%) |
|
|
Married |
7, 398 (81.05%) |
|
Religion |
Roman Catholic |
1, 535 (16.82%) |
|
|
Protestants |
7, 447 (81.58%) |
|
|
Muslim |
51 (0.56%) |
|
|
Others |
95 (1.04%) |
|
Number of children |
0 children |
322 (3.53%) |
|
|
1-3 children |
4, 244 (46.49%) |
|
|
4-6 children |
3, 041 (33.32%) |
|
|
7 & more children |
1, 521 (16.66%) |
|
Wealth index |
Poorest |
2, 204 (24.15%) |
|
|
Poorer |
1, 945 (21.31%) |
|
|
Middle |
1, 866 (20.44%) |
|
|
Richer |
1, 619 (17.74%) |
|
|
Richest |
1, 494 (16.37%) |
|
Provinces |
Central |
935 (10.24%) |
|
|
Copperbelt |
984 (10.78%) |
|
|
Eastern |
1, 144 (12.53%) |
|
|
Luapula |
952 (10.43%) |
|
|
Lusaka |
1, 132 (12.40%) |
|
|
Muchinga |
845 (9.26%) |
|
|
Northern |
886 (9.71%) |
|
|
North Western |
659 (7.22%) |
|
|
Southern |
916 (10.04%) |
|
|
Western |
675 (7.39%) |
|
Region |
Rural |
5, 889 (64.52%) |
|
|
Urban |
3, 239 (35.48%) |
Table 1: Demographic Characteristics of Study Participants
Average Marginal Effects
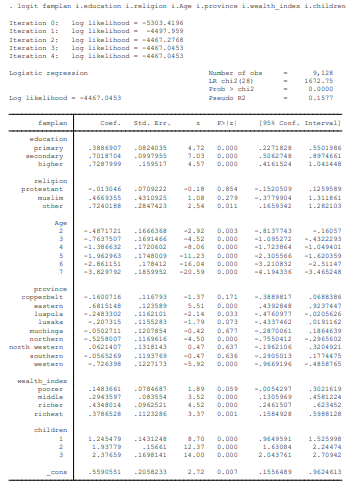
The logistic output below relates the socio-economic related inequalities to the utilisation of family planning services among women of childbearing age in Zambia. The explanatory variables iterated were the level of education, religion, age, province, wealth index as well as number of children as in table 2 below. The successive smaller differences in the log likelihood from 5303.4196 at iteration 0, with no explanatory variables to -4467.0453, iteration 4 with all the explanatory variables is indicative of the convergence of the logit model i.e., when its loss actually moves towards a minima with a decreasing trend. Additional machine learning model training would not improve the model.
The probability of obtaining the Chi-square statistic 0.0000 is statistically significant and would result in the rejection of the null hypothesis of the independence of the seven explanatory variables (level of education, religion, age, province, wealth index, and number of children) and the dependent variable family planning services utilisation among women of childbearing age in Zambia. The six independent variables have some influence in the variations in the utilisation of family planning services among Zambian women of childbearing age.
The Pseudo R2 which is used in nominal and ordinal outcome variables and not the Coefficient of Determination (R2) as a measure of model goodness of fit. Variables like level of education, age group, wealth index, number of children are ordinal whereas religion and province are nominal. Thus, the Pseudo R2 would be a measure of the proportion of variation in the utilisation of family planning services among women of childbearing age in Zambia that is explained by the six independent variables in the Logit regression model. The Logit regression output shows that 15.77% of the variation in the utilisation of family planning services is coming from the six explanatory variables. Out of twenty-eight (28) marginal variables, twenty (20) variables influence the utilisation of family planning services as their probability values are less than 0.05. However, only eight (8) marginal variables; Protestant religion (0.854), Muslim religion (0.279), Copperbelt province (0.171), Lusaka province (0.073), Muchinga province (0.677), North Western province (0.637), Southern province (0.636) and poorer wealth index (0.059) all have p-values greater than 0.05 resulting in the non-rejection of the null hypothesis of independence of the eight (8) explanatory variables and the dependent variable, family planning services utilisation. These explanatory variables are not explaining the log odds for the utilisation of these services among Zambian women of childbearing age.
The regression coefficients of -0.4871721 (age group 20-24years) and -0.7637507 (age group 25-29years) respectively show an insignificant inverse relationship between the two variables when compared to age to age group 15-19 years. The rest of age groups, 30-34, 35-39, 40-44 and 45-49 years shows that the null hypothesis of the independence of the women age and family planning utilisation is rejected, as their p-values (0.000, 0.000, 0.000 and 0.000) are all less than 0.05. This implied that the utilisation of family planning services was depended on age. Age group 30-34 years has the least negative relationship (-1.386632) and age group 45-49 years has a strong negative relationship (-3.829792). The negative regression coefficients show that as women of childbearing age in Zambia get older, they reduce their utilisation of family planning services.
The p-values of the three explanatory variables when compared to no education, primary education (0.000), secondary education (0.000) and higher education (0.000) are statistically significant as they are less than 0.05. The values result in the rejection of the null hypothesis of independence between the level of education and the utilisation of the family planning services. The rejection of the hypothesis implies that the level of education affects the utilisation of services. The regression coefficients show a positive relationship between the two variables. Primary education is the least explanatory vary variables at it explains 38.86907% of the utilisation of family planning services. Higher education is the most explanatory variable as it accounts for 72.87999% of the utilisation of family planning services. The regression coefficients are positive implying that the more the Zambian women of childbearing age go school the more is the utilisation of family planning services.
Women of childbearing age with children 1 to 3, 4 to 6, and 7 and above all have p-values 0.000 less than 0.05 indicating the null hypothesis of independence between the number of children and the utilisation of family planning services. The utilisation is influenced by a certain number of children that a Zambian woman has. As the number of children increase, women in Zambia become indifferent to the utilisation of family planning services.
Although the model p-value is significant (0.000) as well as the p-values of the wealth indices (0.059, 0.000, 0.000 and 0.001), the extent of influence of the marginal variable is very insignificant. When compared to the poorest, the richer wealth index has the highest influence of 43.48014% of the utilisation of family planning services while the poorer index has the least of 14.83661%. The p-values for all the wealth indices are statistically significant as shown in table 2 below.
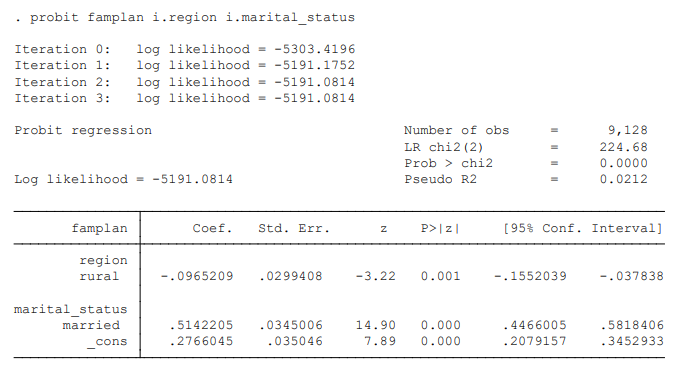
As shown in table 3; Probit model is used to model dichotomous or binary outcome variables. It models the inverse standard normal distribution as a linear combination of the predictors. The successive smaller differences in the log likelihood from 5303.4196 at iteration 0, with no explanatory variables to -5191.0814, iteration 3 with both the explanatory variables is indicative of the convergence of the probit model i.e., when its loss actually moves towards a minima with a decreasing trend. The probability of obtaining the Chi-square statistic 0.0000 is statistically significant and would result in the rejection of the null hypothesis of the independence of the two explanatory variables (region and marital status) and the dependent variable family planning services utilisation among women of childbearing age in Zambia. The two independent variables have some influence in the variations in the utilisation of family planning services among Zambian women of childbearing age. The Probit regression output shows that 2.12% of the variation in the utilisation of family planning services is coming from the two explanatory variables. Thus, the level of region and marital status as explanatory variables are only explaining 2.12% of the utilisation of family planning services, thus showing a relatively low marginal effect. The goodness of fit for the model is 2.12% implying that region and marital status of women of childbearing age in Zambia explains 2.51% of the utilisation of family planning services.
The rural variables and family planning use are dependent of each other. However, the relationship is insignificantly negative shown by the regression coefficient of -0.0965209. This could imply that the use of family planning services was higher among urban women compared to rural women. Thus from the table below, the more the rural Zambia women of childbearing age are involved in family planning programmes the lower is the utilisation of the services as shown in table 3 below.
The P-value of marital status of married women is 0.000 which is statistically significant. The regression coefficient of married women is 0.5142205 which shows that there is a positive relationship between marital status and the utilisation of family planning services among women of childbearing age in Zambia. In fact, 51.42205% of the family planning services utilisation is explained by the marital circumstances of married women of childbearing age compared to the unmarried women. The p-value of the marginal variable (0.000) result in the rejection of the null hypothesis of the independence between marital status (married) and the utilisation of family planning services. Marital status (married) has a marginal effect on the utilisation of family planning services. Thus, married woman are more likely to use family planning services compared to unmarried women as in table 3 below.
Concentration Curves
The concentration curve shows the distribution of the utilization of family planning services between rural and urban women in Zambia. Although the two lines are closer to the 450 line showing an equal utilization of family planning services by both, however the line for urban women is below the equality line implies that they are utilizing the family planning services slightly more than their rural counterparts as shown on the curve below.

Figure 1: Concentration Curve for Women of Childbearing Age
Oaxaca — Blinder Decomposition
Table 4 below shows the contribution of age, marital status, level of education, number of children, wealth index and region to the component of change in the utilization of family planning services. The mean of family planning utilization was 0.7249 for rural and 0.7456 for urban, yielding family planning utilization gap of 2.069 percentage points, which was significant (P<0.032). In general, about 78.49% (0.0369294/0.0206896) of the disparity was due to the different distribution of the predictors (endowments). Adjusting urban women's endowments levels to the levels of rural women would increase urban women of childbearing age's family planning utilization by 3.69%. The coefficient effect accounted for 2.94% of the average gap in the utilization of family planning services and the contribution of the interaction effect was 1.32% as shown in table 4 below.
Table 4 below also shows how differences in the distribution of each factor contributed separately to the first part of the gap (endowment effect). This highlights the increase in family planning use among the rural populations when there are similar characteristics as compared to those in the urban populations. All the categories of these independent variables made significant contribution to explaining the rural-urban inequality gap. In the endowment effect, some factors have positive contribution to the gap, thus increasing the gap while others have negative contributions thus reducing the gap, with total percentage contributions adding up to 100 percent.
The factors that contributed positively to the gap were the richest wealth group (79.76%) and richer wealth group (41.63%). Secondary and tertiary levels of education contributed about 49.69% and 20.13% respectively. Being 45-49 and 20-24 years contributed about 48.60% and 9.45% respectively. In other words, reducing the difference of richest wealth group between the rural and urban women of childbearing age will lead to a reduction of approximately 80% in the disparity.
The differential effect of women of childbearing age with 1-3 children (0.018791/0.0206896 = 90.82%) had the greatest contribution to this part of the disparity, followed by those women with 7 and more children and married women of childbearing age. In other words, being married, having 1-3 children and having seven (7) and more children helped to reduce the gap in family planning utilization by 37.64%, 90.82% and 71.92% respectively. Other factors that also appeared to minimize the gap in the utilization of family planning services between the rural and urban population belong to the poorer wealth group (23.28%), middle wealth group (21.54%), richer wealth group (22.07%), 4-6 children (20.54%), tertiary education (8.98%) and richest wealth group (8.23%).The negative contribution of all the ages, secondary and tertiary education implies that removing the rural/urban difference in ages, secondary and tertiary education widens the disparity. Moreover, the 'interaction part' refers to the gap that is explained by the interaction between the endowment and coefficient effects.
Table 4 below also shows the part of the gap that was accounted by different effect of the factors (coefficient effect) between the rural and urban women of childbearing age. For compositional effect, a positive coefficient suggested that the change in the percentage with that characteristic between rural and urban women of childbearing age was associated with an increase in the difference in use of family planning services. On the other hand, a negative coefficient indicated that family planning use in rural women of reproductive age would have been better if their characteristics had been the same as their urban counterparts. It demonstrates that having primary and secondary education, and falling on any age group were offsetting factors in the use of family planning services which could mean that having primary and secondary education, and falling on any age group contributed in the reduction of inequalities in utilization of family planning services.
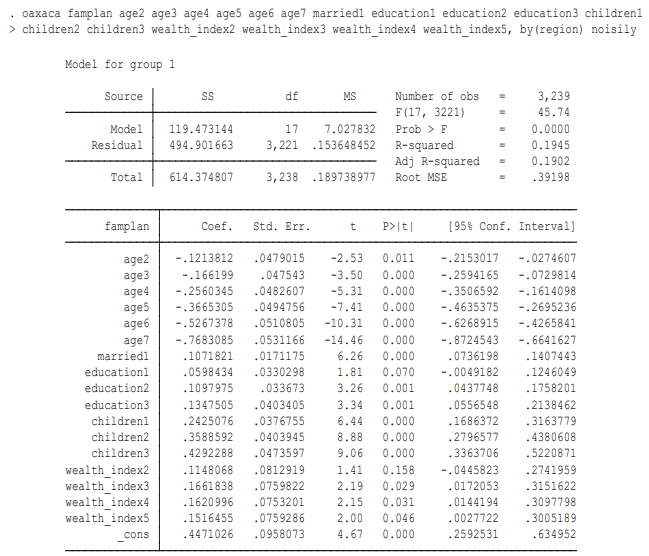
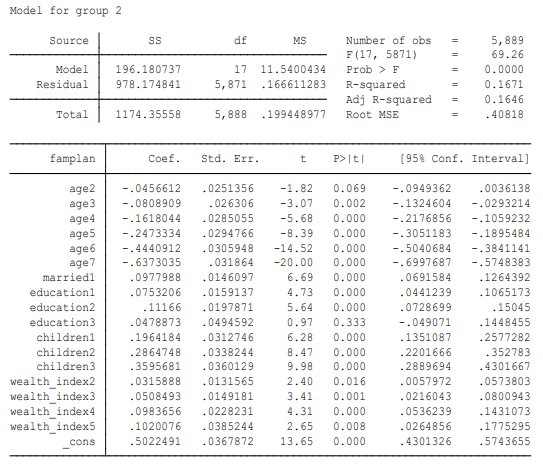
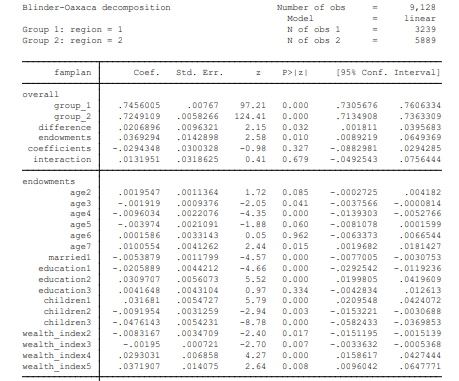
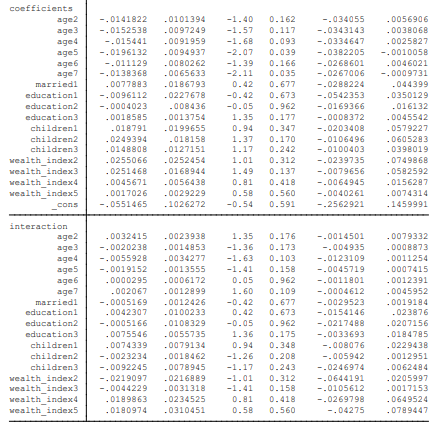
Table 4: Oaxaca – Blinder Decomposition
Discussion
Family planning utilization in Zambia has increased in the past years, from 15% in 1992 to 48% in 2018 (CSO, 2018). There is uncertainty if this progress is cross cutting or only specific to certain socio-economic groups. This study therefore, sought to examine socio-economic related inequalities of family planning service utilization amongst women age 15-19 years oldof reproductive age (15 - 49 years) in Zambia.
This study shows that family planning use declines beyond age 35 and continues to decline until menopause at age 49 years which could be because of satisfied parity and onset of menopause. This is in line with other studies that found that as women approached menopause, loss of partner or acquired the desired number of children, the use of family planning services decreased (Atuahene et al., 2016; Irani et al., 2012). This represents an inverse U-shaped association between age and family planning utilization with the probability of use attaining a maximum in the age range 20-29 years and gradually decline at older ages. These results are anticipated as it reflects a decreasing need for family planning services among older women entering menopause.
This study also revealed that married women were more likely to use family planning services because they were more sexually active. It is likely that unmarried women were less keen to use family planning services because of fear of stigmatization in society as they were not married and unlikely to be given priority by healthcare providers (United Nations, 2017). The positive average marginal effect reinforces this conclusion that moving from not married to married, a woman’s likelihood of family planning utilization is increased. This finding however, contradicts results from a another study in Zambia which showed that married women used less family planning compared to the unmarried because they had a childbearing obligation (Lemba et al., 2014). In addition, Lemba and other (2014) asserted that men have continued desiring having a lot of children, despite their economic status, because it is deemed to improve their status in the society. The differences between the current study and Lemba et al., 2014 study may be due to differences in the sample sizes and the geographical location of the studies. The study by Lemba and colleagues (2014) looked at a more localized population in Kazungula district of Southern province, with a sample of 137 men and women of reproductive age, while this study used data from the 2018, nationally representative, ZDHS, with a sample of 9, 128 women of reproductive age.
Further findings from this study reveal that women with an education, and those whose ideal number of children is met, were more likely to utilize family planning services. This could be attributed to the fact that women with higher education and those with more children are more likely to make rational decision on reproductive health issues and to achieve satisfied parity, respectively (Jafari et al., 2017). In addition, the educated ones are more likely to be engaged in some economic activities, which may require them to use family planning relatively more. The findings of this study are similar to some previous studies that revealed that education is important in utilization and improvement of family planning services (Larsson & Stanfors, 2014; Amentie, 2015). Our study also found that women with relatively more children were more likely to use family planning services because of their achieved satisfied parity. In other words, those without children were not likely to use family planning services as they needed to conceive compared to those with children. This is in disagreement with Blackstone et al. (2017), who found that men in the rural areas for instance, despite their economic status, appreciate having a lot of children which to them is a status in society and would only use family planning services when there is parity satisfaction.
Our study also found that women from richer households used family planning more, which could be because they were more likely to have more access to reproductive health knowledge and therefore have an enhanced ability to make decisions regarding their fertility. Their economic status could also give them means and access to reproductive health services that others may not access. In addition, urban women were more likely to utilize family planning services compared to their rural counterparts which could be due to high literacy levels, and availability and accessibility of family planning services as the health facilities were within reach, as was found by Aslam and others (2016).
This study’s findings further revealed that underutilization of family planning combined with lack of wealth and lack of education are some of the key factors that determine the rural-urban gap. The argument is that, the rural poor have less income compared to their urban counterparts leading to the parallel disparities that exists between them in family planning utilization. This finding supports the findings of a previous study that showed that socio-economic gap or differences in family planning utilization exists and had persisted among women and this had disadvantaged the poor (Aslam et al., 2016).
Urban women of childbearing age were engaged in economic activities that could give them the ability and power to purchase the family planning commodity. Some urban women would utilize family planning services as they could be in employment, and due to career development. Thus, moving from rural areas to urban areas increases the probability of family planning utilization. This finding of this study is similar to Kabonga et al. (2010) who found that rural women had little or no income compared to their urban counterparts and this meant that fertility was high in the rural compared to urban areas.
The concentration curve results showed that utilization of family planning services are in favour of or advantaging wealthier and urban women. This is not surprising since wealth is correlated with education which facilitates the increase to use (Ortayli & Malarcher, 2010). This finding supports previous studies that showed that higher socioeconomic status improves the use of family planning services (Aslam et Al., 2016). Studies show that economically self-sufficient women are more likely to utilize contraception as it enhances their ability to make rational decisions on reproductive health issues (Ortayli, 2010). Regarding the right to use family planning services, while economic status does prevent women from making sole decision about their reproductive health, it could, however, initiate a demand for contraception (Hindin et al., 2014; Amalba et al., 2014).
The Oaxaca – Blinder decomposition results showed that education had a bigger effect in urban than in rural which could imply that the urban population is much better off than their rural counterparts as the disparity in education is in favour of the urban women. The findings of this study are similar to that of the previous studies that revealed that there was low utilization of family planning services which could have been attributed to low education levels. This could be influenced by the ability of individuals to judge when care should be sought (Ashraf et al., 2009). Furthermore, Hindin et al., (2014) found that educational level and higher income lead to an increase in demand for the resources involved in acquiring contraceptives. Other studies also revealed massive socioeconomic gap in health and health care utilization among women of reproductive age due to lower secondary and tertiary levels of education (Aslam et al., 2016; Groot et al., 2018).
Our study found that religion has no effect on family planning use. This could imply that belonging to a particular religion or denomination did not have an influence on family planning use. This result is not in support of some empirical evidence which has demonstrated that religious influences may lead low uptake of family planning despite high knowledge and awareness among women of reproductive age (Kabonga et al., 2010; Mubita-Ngoma and Kadantu, 2010).
Implications for Policy and Practice
This study shows that socioeconomic inequalities in the utilisation of family planning services have persisted, primarily in rural areas despite the policy by the Ministry of Health to integrate family planning services into Mother and Child Health services. The policy was inadequate to increase family planning service utilization to about 58% by 2020 in Zambia. Therefore, there was need for the government to integrate family planning services into every stage of service delivery at Primary Health Care. Additionally, there is need by the government to intensify on interventions such as awareness about importance of utilization of family planning services in the community. This is easier said than done, but can be introduced slowly in line with the existing capacity in the health facilities.
Integration at all levels can be the beginning, and then slowly increase the capacity to handle the increase in family planning services utilization. Further, there was need for all health care workers to under-go training in family planning services. This was to ensure provision of all types of contraceptives in all health facilities to reduce family planning inequalities. Practice (service provision at primary level) was one way of reducing inequalities in family planning service utilization thus by increasing capacity of the health care providers who trained on how to offer different types of family planning services in order to match a woman’s fertility intentions. Furthermore, there is also need to offer family planning services at all points of health service delivery at all times in order to increase uptake.
Limitations
Our study had a number of limitations. First, the study opted to use data on sexually active women of childbearing age as data was readily available. Second, even though data was readily available, the variables were limited as the data was not meant for this research. Third, the limitation in the number of covariates chosen had an effect on the power and robustness of the results. This study did not measure some variables such as side effects, cultural expectations or beliefs and accessibility which might also affect the rural-urban gap in the use of family planning services. However, the broader picture was still clear and the most imperative factors explaining use of family planning have been captured.
Conclusion
Despite efforts by the Zambian government to increase the availability of family planning services, this study has showed that inequality in the use has persisted. Socio-economic inequalities were mostly to the disadvantage of the rural women and in favour of the urban women. These disparities were mainly due to rural-urban differences in the level of education, ages, level of wealth and number of children. If the country is to bridge the gap between the rural and urban women of reproductive age in utilization of family planning services, the problem of low education should be addressed. In addition, health-promotion awareness programs, and economic and non-formal educational empowerment among the rural population should be implemented to enhance the rural women’s ability to make rational decisions on reproductive health issues. Furthermore, improving the way health care systems effectively interact with illiterate women could be a favourable solution in reducing inequality in family planning use.
Competing Interest
The authors declare that they have no competing interests.
Funding
Funding was sourced from the Ministry of Health.
References
- Agadjanian, V., Hayford, S. R., Luz, L., & Yao, J. (2015). Bridging user and provider perspectives: family planning access and utilization in rural Mozambique. International Journal of Gynecology & Obstetrics, 130, E47-E51.
- Amalba, A., Mogre, V., Appiah, M. N., & Mumuni, W. A. (2014). Awareness, use and associated factors of emergency contraceptive pills among women of reproductive age (15-49 years) in Tamale, Ghana. BMC women's health, 14, 1-6.
- Amentie, M., Abera, M., & Abdulahi, M. (2015). Utilization of family planning services and influencing factors among women of child bearing age in Assosa district, Benishangul Gumuz regional state, West Ethiopia. Sci J Clin Med, 4(3), 52.
- Aslam, S. K., Zaheer, S., Qureshi, M. S., Aslam, S. N., & Shafique, K. (2016). Socio-economic disparities in use of family planning methods among Pakistani women: findings from Pakistan demographic and health surveys. PloS one, 11(4), e0153313.
- Blackstone, S. R., Nwaozuru, U., & Iwelunmor, J. (2017). Factors influencing contraceptive use in sub-Saharan Africa: a systematic review. International quarterly of community health education, 37(2), 79-91.
- MOH, C. (2013). ICF international. Zambia demographic and health survey, 2014.
- Central Statistics Office (CSO), Ministry of Health (MOH) [Zambia], ICF International, 2018. Zambia Demographic and Health Survey 2018. Lusaka, Zambia.
- Chanda, M. M., Ortblad, K. F., Mwale, M., Chongo, S., Kanchele, C., Kamungoma, N., ... & Oldenburg, C. E. (2017). Contraceptive use and unplanned pregnancy among female sex workers in Zambia. Contraception, 96(3), 196-202.
- Collins, D., & Gilmartin, C. (2016). Scaling up family planning in Zambia—Part 2: The cost of scaling up family planning services.
- Ogundele, O. J., Pavlova, M., & Groot, W. (2018). Examining trends in inequality in the use of reproductive health care services in Ghana and Nigeria. BMC pregnancy and childbirth, 18, 1-19.
- Hindin, M. J., McGough, L. J., & Adanu, R. M. (2014). Misperceptions, misinformation and myths about modern contraceptive use in Ghana. Journal of Family Planning and Reproductive Health Care, 40(1), 30-35.
- Kabonga, R. M., Baboo, K. S., & Mweemba, O. (2010). Factors influencing utilization of natural family planning among child bearing women in Chilonga Northern Province Zambia. Medical journal of Zambia, 37(4), 223-233.
- Larsson, C., & Stanfors, M. (2014). Women’s education, empowerment, and contraceptive use in sub-Saharan Africa: findings from recent demographic and health surveys. African Population Studies, 1022-1034.
- Lemba, R. (2014). Contraceptives Use among Rural Men and Women of Kazungula (Doctoral dissertation, University of Zambia).
- Ministry of Health, 2012. National Health Strategic Plan 2011-2015. “Towards attainment of health-related Millennium Development Goals and Other National Health Priorities in a clean, caring and Competent environment” in Zambia.
- Mubita-Ngoma, C., & Chongo Kadantu, M. (2010). Knowledge and use of modern family planning methods by rural women in Zambia. Curationis, 33(1), 17-22.
- Newman, K., & Feldman-Jacobs, C. (2015). Family planning and human rights–what’s the connection and why is it important. Washington, DC: Population Reference Bureau.
- Ortayli, N., & Malarcher, S. (2010). Equity analysis: identifying who benefits from family planning programs. Studies in Family Planning, 41(2), 101-108
- UNFPA, UNAIDS, UNICEF, UN Women, WHO, TheWorld Bank Group, 2016. H6 Partnership Annual Report 2016. Harnessing the collective strengths of the UN system to improve the health of women, children and adolescents everywhere H6.
- United Nations, D., & Affairs, S. (2017). World FamilyPlanning 2017—Highlights (ST. ESA/SER. A/414).