
International Journal of Clinical and Medical Education Research(IJCMER)
ISSN: 2832-7705 | DOI: 10.33140/IJCMER
Impact Factor: 0.93


Research Article - (2024) Volume 3, Issue 4
Smartphones as a Multimodal Communication Tool for Interprofessional Communication among Optometrists in Ghana
2Cardiometabolic Epidemiology Research Laboratory, University of Cape Coast, Cape Coast, Ghana
3Department of Population Health Sciences, Duke University, North Carolina, USA
4Accra Medical Centre, Accra, Ghana
5Theresienkrankenhaus Mannheim, Mannheim, Germany
Received Date: Apr 15, 2024 / Accepted Date: May 18, 2024 / Published Date: Jun 10, 2024
Copyright: ©Â© 2024 Ebenezer Oduro Antiri, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Antiri, E. O., Hammond, F. A., Armah, C. G., Nimo, T. K. A. O., Perbandt, E. O. (2024). Smartphones as a Multimodal Communication Tool for Interprofessional Communication among Optometrists in Ghana. Int J Clin Med Edu Res, 3(4), 01-10.
Abstract
Purpose: The ascertain the preferred mode(s) of smartphone-based interprofessional communication, and their perceived effects on clinical outcomes.
Method: Through a purposive sampling method, 344 Optometrists in Ghana were recruited in this cross-sectional study. Modified and validated questionnaires were used to assess the preferred mode(s) of smartphone communication and its effect on clinical outcomes.
Results: The prevalence of Optometrists who use smartphones for their interprofessional communication was 95.2% and a larger percentage of the participants (41.6%) indicated that they were more likely to use all three modes of smartphone-enabled interprofessional communication (speech, images, and image annotation) simultaneously rather than just one or two. Participants who had practiced between 1-5 years were found to subscribe to smartphone-enabled interprofessional communication more [χ2 (3, N = 336) = 24.03, p = .000]. Also, participants working in private facilities were found to subscribe to smartphone- enabled interprofessional communication more [χ2 (3, N = 336) = 12.27, p = .007].
Conclusion: The outcome of this study indicated that, participants preferred using all smartphone-enabled modes of communication simultaneously and had a positive perception about how multi-modal smartphone-enabled interprofessional communication improved clinical outcomes.
Keywords
Smartphone, Multimodal, Interprofessional Communication, Optometrists
Introduction
Interprofessional communication is a critical component of a well-functioning health-care system. It is particularly important because of how it can significantly enhance patient care. Poor communication amongst health professionals has a history of increasing financial costs and worsening clinical outcomes, which is even worse in developing countries like Ghana [1].
Poor healthcare information management, poor healthcare delivery, wrong diagnoses, and inability to afford appropriate treatment regimens are all issues that developing countries face [2,3]. As a result, developing countries must use concepts and technologies that are readily available and inexpensive in order to attain improved health results in a cost-effective manner. Research has shown that frequent and improved communication between healthcare professionals improves knowledge transfer and, as a result, improves patient health outcomes [4-6]. Key health stakeholders in developing countries have thus taken steps to incorporate digital health technologies into strengthening health systems and achieving Sustainable Development Goals related to health (SDGs) [7]. Mobile digital technology is an example of these widely accessible, affordable, and simple-to-use technologies. Although most people in these poor countries face difficulty in accessing basic amenities such as good road networks, electricity, water supply, or cable internet connection, they still have access to mobile technology.
In clinical settings, communication and consultation are crucial, and the specific techniques of interaction between health workers are dictated by the unique characteristics of the clinical nature of their work [8]. In the distant past, most interprofessional communication and knowledge transfer took place face to face, but with recent technological advancements, clinicians have had to adapt to communicating using virtual communication devices like smartphones, especially with the recent global pandemic and the scattering of expertise around the world. However in utilizing these techniques, they must attempt to replicate face-to-face communication to be highly effective [9].
Pimmer et al. (2013) suggest that the most popular ways of communication in clinical health settings utilizing smartphones were speech or text only, speech plus images, and voice, photos, and image annotation otherwise known as guided noticing.
In Africa, there have been studies that have explored the use of smartphones in healthcare, but few have focused on smartphone-based interprofessional communication. A study done by Achampong et al. (2018) which investigated the effects of mobile phone use in the clinical practice of medical students, showed that 98% of them owned smartphones with their main activity being searching for medical information on the internet. Yahya (2019) in his study identified that 45.3% of doctors that participated in the study used smartphones in communicating with other professionals. The study by Ogundaini et al (2021) was a qualitative study that assessed the use of mHealth technology in clinical settings with some health professionals indicating remote communication as their main use of mHealth technology. These studies explore to some extent the ownership, adoption and use of smartphones for interprofessional communication in healthcare, but they do not assess the level of interprofessional communication done, the reasons for doing so and the frequency at which it is done. They also do not investigate the precise modes of communication utilized by health professionals and its perceived effect on health outcomes [1-18].
There is a surprising dearth of evidence supporting the utility of mobile technology for successful interprofessional collaboration, knowledge exchange, and learning, especially in developing countries(8). Although there is an increased need for interprofessional communication due to the COVID-19 pandemic and advancements in telemedicine all over the world, there is little known about the effectiveness of smartphone-based interprofessional communication in developing countries like Ghana. Till date, there is no information on the use of multi-modal smartphone-enabled interprofessional communication among eyecare professionals worldwide. This study intends to bridge that gap by exploring the use of multi-modal smartphone-enabled interprofessional communication among Optometrists in Ghana.
Methods
Research Design
A descriptive cross-sectional study was carried out among Optometrists in Ghana to explore the usage of smartphones for multimodal communication among optometrists in Ghana.
Ethical Consideration
Ethical clearance was obtained from the Technische Hochschule Deggendorf and the Ghana Optometric Association. Before the commencement of the administration of the questionnaire, informed consent was be obtained from participants after telling them the purpose and details of the study. The study adhered strictly to the tenets of the declaration of Helsinki. Participants were told about the voluntary nature of the study and their right to withdraw anytime from the study.
Setting and Participants
This study was conducted in all of the 16 administrative regions of Ghana. The regions are Ashanti, Brong-Ahafo, Ahafo, Bono East, Central, Eastern, Greater Accra, Northern, Upper East, Upper West, North East, Northern, Volta, Oti, Western and Western North. As at July 2021, Ghana had an estimated population of 32,372,889 with an estimated annual growth rate of 2.26%. The total area of Ghana is 238,533 sq km (19). The physician density in Ghana is estimated to 0.14 physicians/1,000 population (2017 est.) with the current health expenditure of Ghana pegged at 3.5% (2018 Est). This study targeted the main primary eye care practitioners in Ghana. This consists of licensed and registered optometrists in Ghana. There are an estimated 407 optometrists in the country.
Sample Size and Sampling
Procedure A total of 344 optometrists participated in this study. The sample size was determined using the fisher’s formula,
Where,
N = minimum sample size,
Z = the standard normal deviation, usually set at 1.96 which corresponds to the 95% confidence interval,
P = estimated prevalence of 50%,
w = confidence interval = 95%.
Per this equation, the sample size was found to be 286 and this was increased to 344 to adjust for attrition rate and non-responses. Purposive sampling was used to select the participants consecutively to enable the researcher answer the research objectives and test the hypothesis.
Procedures and Data Collection tools
Before the commencement of the main data collection for this study, a pre-test was carried out to validate the questionnaire. The questionnaire was tested to ensure that participants understood every item on them and also to identify any weaknesses that should be addressed before the main data collection. The Cronbach alpha (Internal Consistency) was run on the scaled responses and this indicated a high level of internal consistency (0.805). In this descriptive cross-sectional study, 344 registered and duly licensed Optometrists practicing in Ghana were recruited. The questionnaire consisted of four different sections that assessed the demographic characteristics of the participants, their general smartphone usage, their smartphone usage in clinical practice and finally, smartphone-enabled Interprofessional Communication among the participants.
Data Processing and Statistical Analysis
Data collected from participants was initially entered into an Excel Spread sheet. The entries were then checked to ensure accuracy and consistency with the data collated from the respondents. Questionnaires were coded after administration to facilitate easy tabulation and analysis. Statistical analysis was done using R version 4.2.3 for display and analysis. Descriptive statistics was used to ascertain the prevalence of Optometrists who use mobile devices for interprofessional communication and to ascertain the common mode(s) of mobile device communication used for interprofessional communication. Inferential statistics was used to ascertain the relationship between the usage of smartphone multimodal interprofessional communication and some demographic characteristics of the participants.
Results
Socio-Demographic Characteristics A total of 344 Optometrists from all the 16 Ghanaian administrative regions attempted the questionnaire with 336 consenting to complete the questionnaire with a response rate of 97.67%. As shown in table 4.0, majority 264 (78.6%) of the participants were males and the remaining 72 (21.4%) were females. Majority 237 (70.5%) of the total number of participants had practiced between 1-5 years and most of them 215 (64.0%) were trained in the University of Cape Coast (UCC) with the rest 121 (36.0%) being trained at the Kwame Nkrumah University of Science and Technology (KNUST). Majority 179 (53.3) of the Optometrists worked in private practices with most of them 303 (90.2%) having no additional qualification in addition to their Doctor of Optometry degree. The prevalence of Optometrists who use smartphones for their interprofessional communication was 95.2% (336). The socio-demographic characteristics of the respondents are presented in Table 1.
|
Demographics |
Frequency (n) |
Percentage (%) |
|
Gender |
||
|
Male |
264 |
78.6 |
|
Female |
72 |
21.4 |
|
Years of Practice |
||
|
Less than a year |
60 |
17.9 |
|
1-5 years |
237 |
70.5 |
|
6-10 years |
19 |
5.7 |
|
Over 10 years |
20 |
6.0 |
|
Training School |
||
|
UCC |
215 |
64.0 |
|
KNUST |
121 |
36.0 |
|
Type of Health Facility |
||
|
Primary (community health center) |
29 |
8.6 |
|
Secondary (district and regional hospital) |
68 |
20.2 |
|
Tertiary (e.g., teaching, University hospital) |
60 |
17.9 |
|
Private practice |
179 |
53.3 |
|
Additional Qualifications |
||
|
Postgraduate (PHD) |
9 |
2.7 |
|
Postgraduate (Masters) |
9 |
2.7 |
|
Fellowship or Residency |
2 |
0.6 |
|
Diploma |
13 |
3.9 |
|
No other qualification |
303 |
90.2 |
|
Smartphone for Interprofessional Communication |
||
|
Yes |
320 |
95.2 |
|
No |
16 |
4.8 |
*Percentages may not total 100 due to rounding
UCC – University of Cape Coast
KNUST – Kwame Nkrumah University of Science and Technology
Table 1: Demographic Characteristics of the Respondents
Use of Smartphones in Clinical Settings
Most (92.9%) of the participants indicated that they use their smartphones to search for health information, and 92.3% of this number preferred using search engines like Google and PubMed to search for health information in their practices. Majority (74.4%) of the participants indicated that they searched for health information daily. Most (90.5%) indicated that they did communicate with patients using their smartphones, and 91.9% out of this number preferred using phone calls to communicate with their patients.
When asked about how often they did this with their smartphones, a large number [141 (42.0%)] of the participants disclosed that they communicated with their patients weekly. Majority (92.9%) indicated that they communicated with other professionals using their smartphones and 90.1% of this number preferred the usage of phone calls to communicate with other professionals. When asked about how often they did this with their smartphones, majority 117 (37.5%) of the participants disclosed that they communicated with other professionals daily. This is further illustrated in Table 2.
|
Use of Smartphones in clinic settings |
Frequency (n) |
Percentage (%) |
|
Means for Searching for Health Information |
||
|
Through Apps for smartphones |
153 |
49.0 |
|
Search engines (Google, PubMed etc.) |
288 |
92.3 |
|
Social media (Facebook, Twitter) |
119 |
38.1 |
|
Video services (YouTube) |
221 |
70.8 |
|
Frequency of health information search |
||
|
Daily |
232 |
74.4 |
|
Weekly |
72 |
23.1 |
|
Monthly |
8 |
2.6 |
|
Yearly |
0 |
0 |
|
Smartphone Communication with patients |
||
|
SMS |
89 |
29.3 |
|
|
34 |
11.2 |
|
Social Media (Facebook, Twitter) |
16 |
5.3 |
|
Messenger Apps (like WhatsApp, Telegram, Signal) |
256 |
84.2 |
|
Phone calls |
271 |
91.9 |
|
Frequency of Smartphone Communication with patients |
||
|
Daily |
79 |
23.5 |
|
Weekly |
141 |
42.0 |
|
Monthly |
84 |
25.0 |
|
Yearly |
0 |
0 |
|
Smartphone Communication with other professionals |
||
|
SMS |
107 |
34.3 |
|
|
64 |
20.5 |
|
Social Media (Facebook, Twitter) |
16 |
5.1 |
|
Messenger Apps (like WhatsApp, Telegram, Signal) |
272 |
87.2 |
|
Phone calls |
281 |
90.1 |
|
Frequency of Smartphone Communication with other professionals |
||
|
Daily |
117 |
37.5 |
|
Weekly |
93 |
29.8 |
|
Monthly |
94 |
30.1 |
|
Yearly |
8 |
2.6 |
*Percentages may not total 100 due to rounding
Table 2: Smartphone Usage in Clinical Practice
Assessing the Common Mode(S) of Smartphone Communica-tion Used for Interprofessional Communication
Majority (86.9%) of the participants stated that they employed images in their interprofessional communication followed by speech or text [263 (82.2%)]. Asked on which communication mode(s) they would prefer to use most, most of the participants [133 (41.6%)] indicated that they were more likely to use all (Speech, images, and image annotation) simultaneously. This is shown in table 3.
|
|
Frequency (n) |
Percentage (%) |
|
Communication Mode |
||
|
Speech or Text |
263 |
82.2% |
|
Images |
278 |
86.9% |
|
Annotated Images |
79 |
27.1% |
|
Preferred Mode |
||
|
Speech or Text only |
83 |
25.9 |
|
Speech and images only |
104 |
32.5 |
|
Speech, images, and image annotation |
133 |
41.6 |
Table 3: Modes of Smartphone Communication Used for Interprofessional Communication
Clinical Cases in which Optometrists Employ Interprofessional Communication
Majority (71.5%) of the participants stated that they employed interprofessional communication when they encountered Ocular Disease cases. Asked on which type of cases the participants were more likely to use their smartphones for while at work, a large number of the participants [122 (38.1%)] indicated that they were more likely to employ interprofessional communication when they encountered Ocular Disease cases. This is shown in table 4.
|
|
Frequency (n) |
Percentage (%) |
|
Contact Lenses |
126 |
40.4 |
|
Vision Therapy and Rehabilitation |
184 |
59.0 |
|
Sports Vision |
65 |
20.8 |
|
Ocular Disease |
223 |
71.5 |
|
Geriatric Cases |
47 |
15.1 |
|
Pediatric Cases |
142 |
50.7 |
|
Likely Use |
||
|
Contact Lenses |
33 |
10.3 |
|
Vision Therapy and Rehabilitation |
68 |
21.3 |
|
Sports Vision |
19 |
5.9 |
|
Ocular Disease |
122 |
38.1 |
|
Geriatric cases |
19 |
5.9 |
|
Pediatric cases |
59 |
18.4 |
*Percentages may not total 100 due to rounding
Table 4: Clinical Cases in which Optometrists Employ Interprofessional Communication
Assessing the Challenges the Participants Face Using Smartphones for Interprofessional Communication
Majority of the participants (82.2%) who engage in Smartphone- enabled interprofessional communication cited ‘internet access problems’ as the main challenge that they faced with ‘poor electricity supply’ being the least cited challenge cited by the participants. This is shown in figure 1.
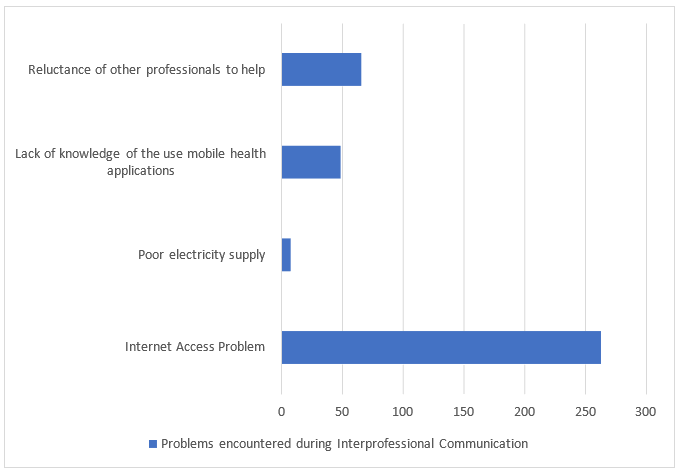
Figure 1: Problems Encountered During Interprofessional Communication
Assessing the Self-Reported Effectiveness of Multimodal Smartphone Communication in Improving Clinical Outcomes
Generally, most of the participants had a positive perception about how smartphone-enabled interprofessional communication improve their clinical outcomes by making their day-to-day clinical practice quicker, efficient and easier. A notable number [119 (37.2%)] of the participants strongly agreed that smartphone-enabled interprofessional communication made their day-to-day clinical practice quicker, 118 (36.9%) strongly agreed that smartphone-enabled interprofessional communication made their day-to-day clinical practice efficient, with 103 (32.2%) strongly agreeing that smartphone-enabled interprofessional communication made their day-to-day clinical practice easier. The participants generally believed that smartphone-enabled interprofessional communication was instrumental in diagnosing their patients, with some 87 (27.2%) strongly agreeing. This is illustrated in figure 2.
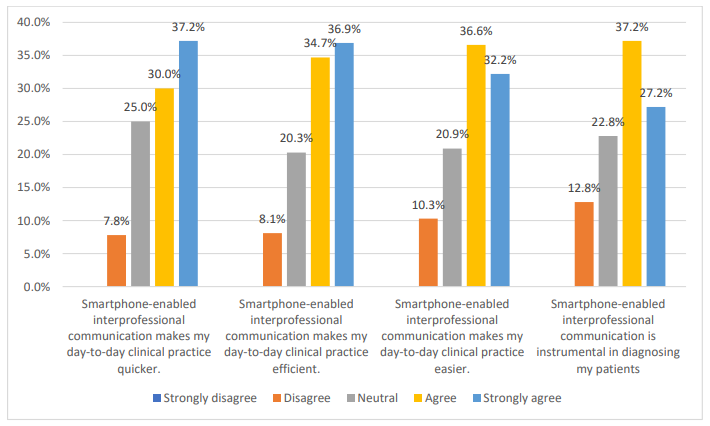
Figure 2: Self-Reported Effectiveness of Smartphone-Enabled Communication in Improving Clinical Outcomes
Relationship between Demographic Characteristics and the Use of the Smartphone for Interprofessional Communication
The number of participants that used the smartphone for interprofessional communication differed by gender, [χ2(1, N = 336) = 10.56, p = .003], number of years of practice, [χ2(3, N = 336) = 24.03, p = .000], and place of work, [χ2(3, N = 336) = 12.27, p = .007]. This is further shown in Table 5
|
|
Smartphone for Interprofessional Communication |
χ2 |
p-value |
|
|
|
Yes |
No |
|
|
|
Gender |
||||
|
Male |
256 |
8 |
10.561 |
0.003 |
|
Female |
63 |
9 |
|
|
|
Years of practice |
||||
|
Less than a year |
56 |
4 |
24.027 |
0.000 |
|
1-5 years |
232 |
5 |
|
|
|
6-10 years |
15 |
4 |
|
|
|
Over 10 years |
16 |
4 |
|
|
|
Training Institution |
||||
|
UCC |
207 |
9 |
1.004 |
0.313 |
|
KNUST |
112 |
8 |
|
|
|
Place of Work |
||||
|
Primary (community health center) |
24 |
5 |
12.274 |
0.007 |
|
Secondary (district and regional hospital) |
64 |
4 |
|
|
|
Tertiary (e.g., teaching, University hospital) |
56 |
4 |
|
|
|
Private practice |
175 |
4 |
|
|
UCC – University of Cape Coast
KNUST – Kwame Nkrumah University of Science and Technology
Table 5: Relationship between Demographic Characteristics and the Use of the Smartphone for Interprofessional Communication
Discussion
Interprofessional communication is an important constituent of functional health care systems because of how it remarkably improves patient care, as poor communication between health professionals has the tendency to result in massive financial losses and the worsening of clinical outcomes. In this study, the prevalence of Optometrists who use smartphones for their interprofessional communication was 95.2%. This rate of use recorded in this study was as expected, with a previous study by Baumgart (2011)(20) finding smartphone usage in clinical settings to be 98%. Ghana generally has a high uptake of smartphones (21) and so it is expected that health professionals would own and use smartphones in their daily interaction with other professionals and patients.
In this study, 92.9% of the participants indicated that they use their smartphones to search for health information. This was relatively higher than the study among British surgeons by Patel et al. (2015) (22) who recorded an equally high percentage of participants (86.2%). In searching for health information, 92.3% preferred using search engines like Google and PubMed to search for health information in their practices, with 74.4% indicating that they did this daily. This was similar to the study by Osei-Bonsu (2016) (23) whose participants had the same preferences for the search of health information. Patel et al. (2015)(22) also had majority of their participants (76.7%) preferring Google and other search engines, despite recording a relatively lower percentage.
This study discovered that 90.5% communicated with patients using smartphones, with 91.9% of this number preferring phone calls to communicate with their patients. Patient-physician communication has been found to be a very important factor in the improvement of health outcomes and Dash et al. (2016)(24) found that physicians preferred phone calls over email and text messages, because they could choose when to call, avoid miscommunication and engage in real time two-way conversations. The study revealed 141 participants (42.0%) communicated with their patients weekly, since they were more likely to meet particular patients on a weekly basis than on a daily basis.
Majority of the participants (92.9) indicated that they communicated with other professionals using their smartphones. This was backed by Niazkhani et al. (2009)(25) who believed that practitioners relied on the skills, knowledge, and competence of their coworkers, hence the need to communicate with other professionals. Out of the number that communicated with other professionals, 281 (90.1%) preferred using phone calls to communicate with other professionals, with 117 (37.5%) of the participants disclosing that they communicated with other professionals daily. This was similar to a study by Hampshire et al. (2017)(26) who reported that health workers in Ghana felt the need to contact colleagues by phone for a consult when managing a patient.
The clinical cases that required Optometrists to contact another professional was explored, and majority (71.5%) stated that they employed interprofessional communication when they encountered Ocular Disease cases, followed by vision therapy and rehabilitation (59.0%). This was similar to a study done by Mansoor et al. (2021)(27) who discovered that eye professionals were likely to contact colleagues on cases of red eye than anything else. However, it is important to conduct further studies because there is a paucity of research on the subject.
Majority of the participants (41.6%) indicated that they were more likely to use all modes of smartphone communication (Speech, images, and image annotation) simultaneously. This makes sense as Pimmer et al. (2013)(8) suggested that when speech (typological representations) is linked with images (topological representations) in the form of annotation, the less knowledgeable actor is able to recall and transfer more information after the communication.
Majority of the participants (82.2%) citied ‘internet access problems’as the main challenge that they faced with ‘poor electricity supply’ being the least cited challenge. The CIA World Factbook purports that there are around 40,857,077 mobile subscriptions in Ghana, with 39% (10,959,964) of the population utilizing the internet in 2018(21). This shows that even though there is a high uptake of mobile phone device use, the usage and ready access to internet connectivity remains a problem. Osei-Bonsu (2016) (23) states that professionals who are in underdeveloped areas are more likely to initiate interprofessional communication, having the need to engage other professionals or refer them for further management. These underdeveloped areas, however, are usually plagued by internet connectivity problems.
Concerning how smartphone-enabled interprofessional communication made their day-to-day clinical practice quicker, 119 (37.2%) strongly agreed with 96 (30.0%) agreeing. Timely communication inside the healthcare system remains critical to reducing medical errors and smartphones play a huge role in making healthcare communication quicker. A review done by Ozdalga et al. (2012) (28) on the usage of smartphones in medicine showed that nurses and other allied health professionals spent less time attempting to contact physicians when they used smartphones. 118 (36.9%) strongly agreed that smartphone-enabled interprofessional communication made their day-to-day clinical practice efficient with 111 (34.7%) agreeing. This was comparable to a study by Spurck et al. (1995)(29) who discovered that when nurses were given portable phones to carry, they believed their hospital's telecommunication system was more effective. About 117 (39.4%) agreed that smartphone-enabled interprofessional communication made their day-to-day clinical practice easier with 103 (32.2%) strongly agreeing. Again in the same review by Ozdalga et al. (2012)(28), a greater number of articles described how smartphones are boosting communication in health care.
The participants generally believed that smartphone-enabled interprofessional communication was instrumental in diagnosing their patients, with majority 119 (37.2%) agreeing and some 87 (27.2%) strongly agreeing. Literature backs this finding as smartphones have been shown to be more suitable for usage in remote assessment and diagnosis of ailments when compared to other channels of communication (30–32).
The number of participants that used the smartphone for interprofessional communication differed by gender, number of years of practice, and place of work. People who had practiced for fewer years were more likely to initiate and engage in interprofessional communication because they were more likely to be the less knowledgeable in the professional relationship. This is in line with previous studies (1,8), that showed that less knowledgeable actors were more likely to take full advantage of opportunities to communicate with more knowledgeable actors. Concerning the place of work of the Optometrists, it is to be noted that most private facilities that provide ophthalmic care in Ghana usually have just one cadre of eye care providers. As a result, they are more likely to engage in smartphone-enabled interprofessional communication as opposed to general healthcare facilities who have a myriad of professionals that promote face-to-face interactions.
Conclusion
The outcome of this study indicated that the most utilized modes of smartphone-enabled interprofessional communication were all three (Speech, images, and image annotation) simultaneously. The participants generally had a positive perception about how multi¬modal smartphone-enabled interprofessional communication improved their clinical outcomes. The findings of the study provide a foundation for future studies, as there is a deficit of studies on multi-modal interprofessional communication worldwide, and no studies exploring the effect of multi-modal smartphone-enabled interprofessional communication on clinical outcomes in sub-Saharan Africa. Prior to this study, there was minimal evidence in Ghana on the subscription and benefits of using mHealth technologies in interprofessional communication. This study shows that smartphones, and consequently mHealth technologies can have a positive impact on clinical outcomes, especially when health professionals do not have certain expertise physically available. it is recommended that healthcare establishments facilitate the usage of smartphones by healthcare providers to search for health information, communicate with patients and also communicate with other professionals to improve the health outcomes of patients.
Funding Statement: This study was carried out without external funding
References
- Sutcliffe KM, Lewton E, Rosenthal MM. Communication failures: an insidious contributor to medical mishaps. Acad Med. 2004;79(2):186–94.
- Anyangwe S, Mtonga C. Inequities in the global health workforce: the greatest impediment to health in sub-Saharan Africa. Int J Environ Res Public Health. 2007;4(2):93–100.
- Qiang CZ, Yamamichi M, Hausman V, Altman D. Mobile Applications for Health Sector. 2011.
- Sheehan J, Laver K, Bhopti A, Rahja M, Usherwood T, Clemson L, et al. Methods and Effectiveness of Communication Between Hospital Allied Health and Primary Care Practitioners: A Systematic Narrative Review. J Multidiscip Healthc. 2021;14:493–511.
- Stewart MA. Stuck in the middle: the impact of collaborative interprofessional communication on patient expectations. Shoulder Elb. 2018 Jan;10(1):66–72.
- Hansson A, Svensson A, Ahlström BH, Larsson LG, Forsman B, Alsén P. Flawed communications: Health professionals’ experience of collaboration in the care of frail elderly patients. Scand J Public Health. 2018 Nov;46(7):680–9.
- World Health Organization. Millenium Development Goals (MDGs). 2018 [cited 2021 Aug 11]. SDG 3: Good Health and Wellbeing. Available from: https://www.who.int/health-topics/sustainable-development-goals#tab=tab_1
- Pimmer C, Mateescu M, Zahn C, Genewein U. Smartphones as multimodal communication devices to facilitate clinical knowledge processes: randomized controlled trial. J Med Internet Res. 2013;15(11):e263.
- Ahlsén E, Lindström NB. Multimodal communication in intercultural health care interactions. In: Proceedings of the 4th Nordic Symposium on Multimodal Communication. 2012. p. 39–46.
- Jennings L, Ong’ech J, Simiya R, Sirengo M, Kussaye S. Exploring the use of mobile phone technology for the enhancement of the prevention of mother-to-child transmission of HIV program in Nyanza, Kenya: a qualitative study. BMC Public Health. 2012;13:1131.
- Oyeyemi SO, Wynn R. Giving Cell Phones to Pregnant Women and Improving Services may Increase Primary Health Facility Utilization: A casecontrol study of a Nigerian project. Reprod Health. 2014;11(1):8.
- Crankshaw T, Corless IB, Giddy J, Nicholas PK, Eichbaum Q, Butler LM. Exploring the patterns of use and the feasibility of using cellular phones for clinic appointment reminders and adherence messages in an antiretroviral treatment clinic, Durban, South Africa. AIDS Patient Care STDS. 2010;24(11).
- Medhanyie AA, Little A, Yebyo H, Spigt M, Tadesse K, Blanco R, et al. Health workers experiences, barriers, preferences and motivation factors in using mHealth forms in Ethiopia. Hum Resour Health. 2015;13(2).
- Bos L, Schouten L, van Vught L, Wiewel M, Ong D, Cremer O, et al. ESICM LIVES 2016: part one: Milan, Italy. 1-5 October 2016. Intensive Care Med Exp. 2016 Sep;4(Suppl 1).
- Betjeman TJ, Soghoian SE, Foran MP. mHealth in Sub-Saharan Africa. Fayn J, editor. Int J Telemed Appl [Internet]. 2013;2013:482324. Available from: https://doi. org/10.1155/2013/482324
- Achampong EK, Keney G, Attah NOS. The Effects of Mobile Phone Use in Clinical Practice in Cape Coast Teaching Hospital. Online J Public Health Inform. 2018;10(2):e210.
- Yahya H. Healthcare-related smartphone use among doctors in hospitals in Kaduna, Nigeria - A Survey. Niger J Clin Pract. 2019 Jul;22(7):897–905.
- Ogundaini OO, de la Harpe R, McLean N. Integration of mHealth Information and Communication Technologies Into the Clinical Settings of Hospitals in Sub-Saharan Africa: Qualitative Study. JMIR mHealth uHealth. 2021 Oct;9(10):e26358.
- Ghana Statistical Service. 2021 Population and Housing Census: Summary Report of Final Results. Accra; 2021.
- Baumgart DC. Smartphones in Clinical Practice, Medical Education, and Research. Arch Intern Med. 2011;171(14):1294–6.
- Central Intelligence Agency. The World Factbook. 2021. Communication. Available from: https://www.cia.gov/the-world-factbook/countries/world/#communications
- Patel RK, Sayers AE, Patrick NL, Hughes K, Armitage J, Hunter IA. A UK perspective on smartphone use amongst doctors within the surgical profession. Ann Med Surg. 2015;4(2):107–12.
- Osei-Bonsu F. Assessing the use of smartphones among health professionals in Ghana: A case study 37 Military Hospital. University of Tromsø; 2016.
- Dash J, Haller DM, Sommer J. Use of email, cell phone and text message between patients and primary-care physicians: cross-sectional study in a French-speaking part of Switzerland. 2016;16:549.
- Niazkhani Z, Pirnejad H, Berg M, Aarts J. The impact of computerized provider order entry systems on inpatient clinical workflow: A literature review. J Am Med Informatics Assoc. 2009;16(4):539–49.
- Hampshire K, Porter G, Mariwah S, Munthali A, Robson E, Owusu SA, et al. Who bears the cost of ‘informal mhealth’?Health-workers’ mobile phone practices and associated political-moral economies of care in Ghana and Malawi. Health Policy Plan [Internet]. 2017 Feb 1;32(1):34–42. Available from: https://doi.org/10.1093/heapol/czw095
- Mansoor H, Khan SA, Afghani T, Assir MZ, Ali M, Khan WA. Utility of teleconsultation in accessing eye care in a developing country during COVID-19 pandemic. PLoS One [Internet]. 2021;16(1):e0245343. Available from: https://doi. org/10.1371/journal.pone.0245343
- Ozdalga E, Ozdalga A, Ahuja N. The Smartphone in Medicine: A Review of Current and Potential Use Among Physicians and Students. J Med Internet Res. 2012;14(5):e128.
- Spurck PA, Mohr MA, Seroka AM. The impact of a wireless telecommunication system on time efficiency. J Nurs Adm. 1995;25:21–6.
- Filip M, Linzer P, Šámal F, TesaÅ? J, Herzig R, Školoudík D. Medical consultations and the sharing of medical images involving spinal injury over mobile phone networks. Am J Emerg Med. 2012;30(6):961–5.
- Kumar S, Wang EH, Pokabla MJ, Noecker RJ. Teleophthalmology assessment of diabetic retinopathy fundus images: smartphone versus standard office computer workstation. Telemed J E Health. 2012;18(2):158–62.
- Tsai HH, Pong YP, Liang CC, Lin PY, Hsieh CH. Teleconsultation by using the mobile camera phone for remote management of the extremity wound: a pilot study. Ann Plast Surg. 2004;53(6):584–7.