
Toxicology and Applied Pharmacology Insights(TAPI)
ISSN: 2641-0451 | DOI: 10.33140/TAPI

Research Article - (2020) Volume 3, Issue 1
Sinonasal Inverted Papilloma: Epidemiological and Pathological Profile from 15 Cases
2Otolaryngology department, Morocco
3Radiology department, Morocco
Received Date: Jan 21, 2020 / Accepted Date: Jan 27, 2020 / Published Date: Feb 14, 2020
Copyright: ©Copyright: ©2020 Imane Boujguenna, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Inverted papilloma is a rare benign Sino nasal tumor marked by strong local aggressiveness, a high rate of recurrence after surgery and an unpredictable risk of association with squamous cell carcinoma. We retrospectively investigated 15 cases of inverted papilloma that were treated between January 2004 and December 2018, diagnosed at the pathological anatomy department, CHU MOHAMMED VI of Marrakech. The objective of this work was to study the epidemiological and anatomopathological profile of these polyps. The sex ratio of 2.75 was clearly predominate in males with an average age of 40 years. Its main clinical symptoms was manifested by nasal blockage. The radiological assessment using CT and nasosinus MRI couple constituted a very important means of the positive diagnosis of the inverted papilloma and of the choice of the operating method. Histological examination showed a papillomata’s polypoid respiratory mucosa, at the level of the chorion, with signs of low grade dysplasia in only one case. Their high potential for local aggressiveness, the fear of a recurrence and the possibility of the occurrence of a malignant tumor require radical management.
Keywords
Sino Nasal Papilloma, Pathology
Introduction
The inverted papilloma represents 0.5 to 4% of Sino nasal tumors [1]. It is a benign slow-growing tumor [2]. The inverted papilloma is mainly characterized by a slow local evolution, an osteolytic potential, a tendency to recurrence and a malignant transformation potential [3]. The anatomical starting point is most often the latero- nasal wall, more particularly at the level of the middle meatus [4]. It is one of the tumors developed from the Schneiderian membrane of which there are 3 types: inverted, fungiform and cylindrical [4]. The histological aspect of the nasolabial polyps is very characteristic, their name is derived from either the epithelium from which they are formed or the Schneiderian membrane or from the endophytic character of the epithelial proliferation. Many studies have sought to explore various etiological hypotheses (allergic, viral, inflammatory, etc.), the main cause currently is believed to be of viral origin, with the involvement of the human papillomavirus frequently found [5]. Other viruses such as the Ebstein Barr virus are also believed to be implicated in the pathogenesis of the reverse polyp [6].
The objective of our work is to study the epidemiological and anatomopathological characteristics of Sinonasal inverted papilloma.
Material and methods
This is a retrospective study spread over 14 years (January 2004- December 2018) of 15 cases of inverted polyp, diagnosed at the anatomical pathology department CHU MOHAMMED VI of Marrakech.
Results
The average age of our patients was 40 years with age extremes ranging from 11 years to 70 years with 11 men (73%) and 4 women (27%). The sex ratio (men / women) is 2.75.
Figure 1: Gender Distribution of the Sinonasal inverted papilloma
The reasons for consultation in the patients in our series were essentially: nasal obstruction, rhinorrhea, epistaxis, dysosmia and facial pain and the involvement was unilateral in all our patients.
The clinical examination was carried out systematically and bilaterally from the first consultation, and which was carried out firstly without preparation of the nasal cavities and secondarily after preparation based on wicks soaked in xylocaine naphazoline 5%. This examination made it possible to show: a gray, unilateral, multi-lobed and bleeding tumor process on contact in all patients. All cases underwent facial CT visualized a unilateral tumor process extending to the maxillary sinus (Figures 2, 3, 4).
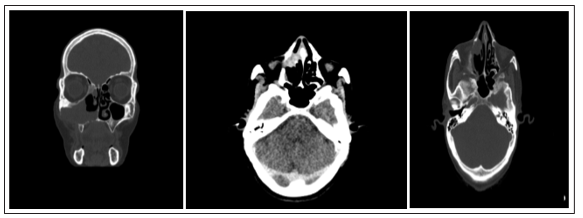
Figures 2, 3, 4: Naso-ethmoido-maxillary lesional process with moderate bone
aggressiveness increases heterogeneously after injection of the contrast product (facial TDM) Total tumor removal was the therapeutic alternative chosen for all patients. The macroscopic examination of the samples received at the pathology service was fragmented material in all cases, measuring between 0.5 and 5 cm. It was brownish in color, firm in consistency and the site of hemorrhagic changes. Histological examination showed a papilllomatous polypoid respiratory mucosa, invading the level of the chorion with signs of low grade dysplasia in only one case (Table I), (figures 5, 6, 7).
Table 1: Dysplastic characteristics
|
Presence / absence of dysplasia |
Number of cases |
percentage |
|
No signs of dysplasia |
14 cases |
93% |
|
Low grade dysplasia |
1 case |
7% |
|
High grade dysplasia |
0 case |
0% |
|
Association with squamous cell carcinoma |
0 case |
0% |

Figure 5: Benign proliferation of endophytic architecture (HEX10)
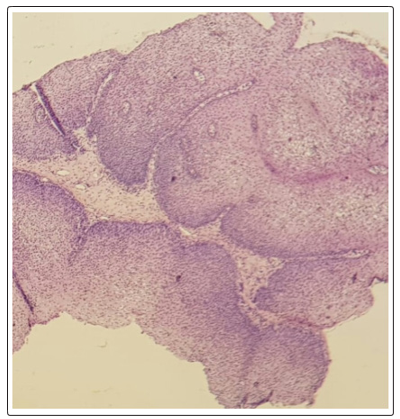
Figure 6: Benign proliferation of endophytic architecture (HEX20)
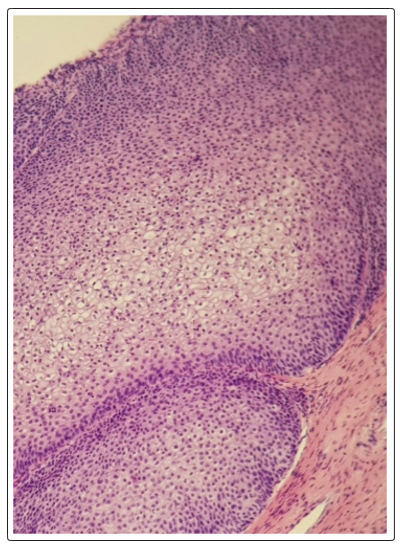
Figure 7: The surface epithelial coating is sometimes of the transitional type, sometimes of the hyperplastic squamous type and focalily covered with keratosis (HEX40)
Discussion
The inverted nasal sinus polyp is a benign sinonasal tumor, which has a high potential for local and regional aggressiveness. It also hace a high degree of recurrence and an unpredictable risk of association and / or malignant transformation [7]. It is rare and accounts for 0.5 to 4% of all nasal tumors [8]. Its pathogenesis is still poorly understood. The viral hypothesis is currently the most accepted. The association with the human papilloma virus (hPv) has been demonstrated since 1987 [9, 10]. Syrjanien [11] reports that 33% of reverse polyps are associated with HPV.
In other studies, the Epstein Barr virus had been found and it seems that there is a synergistic action between these two viruses [12, 13]. Other factors have been suggested: trauma to the nasal cavity seems to be a factor triggering or favoring the genesis of these tumors, certain industrial pollutants or tobacco [14]. The reverse polyp affects men more than women with a predilection age between 50 and 70 years. Exceptionally, it occurs in children. The clinical symptomatology is dominated by unilateral nasal obstruction which can be associated with rhinorrhea, epistaxis, and disturbances of smell or facial pain. Other signs can be found in the neighboring organs: facial deformation, eye signs such as exophthalmos or diplopia [10], hearing or neurological damage [15]. The clinical examination is based on nasal endoscopy. Macroscopically, the tumor appears as a unilateral formation of grayish or pinkish color, of firm consistency, with irregular surface, achieving the classic muri form or cauliflower pact appearance [7]. Nasal endoscopy makes it possible to study the site of the tumor which is in 80% of cases at the expense of the lateral wall of the nasal fossa at the level of the root of the middle horn [8]. A biopsy must be performed at the same time, it must be wide, deep and multiple due to the variability of the histological samples.
A distinction is made between inverted papilloma of the nasal lateral walls and the para-nasal sinuses and exophytic or fungiform papilloma of the nasal septum. The remaining 3% is represented by the cylindrical cell papilloma of the lateral walls of the nasal cavity. A classification drawn up in 1971 by Hyams was then taken up by the WHO, it organizes nasal papillomas into 3 anatomopathological categories.
Our study is mainly focused on inverted papillomas which represent on average 50 to 70% of nasosinus papillomas depending on the series. Their histology was identified by Ringertz in 1938, who defined them as "tumors formed by an intense epithelial proliferation which penetrates inside the stroma to form crypts.
The epithelium is of the stratified cylindrical or transitional type. The basement membrane is still intact and the atypia exceptional. Inverted papillomas of ectopic topography may exist by heterotopic migration of this Schneiderian membrane during embryogenesis, one can thus occasionally find oropharyngeal inverted papillomas, of the posterior wall of the pharynx or of the lacrimal sac [16-18]. Macroscopically the inverted polyps have an irregular polyploid shape whose consistency can be hard or softer, they are generally opaque to trans-illumination as opposed to inflammatory nasal and sinus polyps which are trans illuminable. Their color is variable rather pink or even hemorrhagic with a soft consistency [1]. They can completely invade the nasal cavity and exteriorize via the nasal vestibule or later in the nasopharynx. Histologically, the tumor epithelium is thickened, hyperplastic and invades the underlying stroma. Epithelial proliferation is the main histological constant of these inverted polyps, the cell type is variable; there are 4 main types [19]:
(a) Cylindrical pseudo stratified respiratory type.
(b) Squamous stratified squamous type.
(c) Transitional made up of stacked basal cells.
(d) The Malpighian type is generally the most frequently encountered.
A combination of these different cell types can be found within the same tumor, in variable proportion. We sometimes find the presence of mitosis, even cellular atypia, especially in the deepest epithelial layers, without there being any malignant transformation. The basement membrane is still intact [20]. It separates the inverted hyperplastic epithelium from the underlying connective stroma. It is generally fine (a thickening of the basement membrane being more frequently found in cases of simple polyps in the nasal cavity or in chronic inflammatory conditions). However, its thickness can increase in the event of an inflammatory reaction occurring on contact. Involvement of the basement membrane should evoke the presence of neoplastic cells raising suspicion of a coexisting carcinoma.
The chorion often appears compact, thickened, fibrous but sometimes edematous and loose. The invagination of the epithelium in the underlying chorion induces the formation of subepithelial crypts. The mucous secreting glands usually present are replaced by pseudo- glands resulting from epithelial invagination and the sectional appearance of which gives an appearance of microcystic formations with mucous contents, trapped below the surface due to obstruction, by proliferation epithelial, excretory canaliculi of the tubuloacinous glands.
Dysplasia and malignant transformation into squamous cell carcinoma are histological signs described in the literature and to be investigated [21].
Conclusion
The Sino nasal inverted papilloma is most often a benign tumor. The clinical symptomatology is not specific. Before any therapeutic treatment, a radiological exploration is essential.
The treatment is exclusively surgical. Its high potential for local aggressiveness, the fear of recurrence and malignant transformation require radical management and a good anatomic-clinical correlation.
References
- Momose KJ, A L Weber, M Goodman, A S MacMillan Jr, G H Roberson(1980) Radiological aspects of inverted papilloma. Radiology 134:73-79.
- Bonfils P (2007) Tumeurs bénignes du nez et des sinus. Le papillome inversé nasosinusien. EMC-Oto-rhino-laryngologie 20: 400-410.
- Francois M, Isabelle de Gaudemar, Monique E (1994) Tumeurs bénignes du nez et des sinus. EMC-Oto-rhino-laryngologie 20: 400-410.
- Duruisseau O, Yona L, Wagner I, Baglin AC, De Dieuleveult T, et al. (2001) Papillome inversé: chirurgie endonasale sous guidage endoscopique versus chirurgie par voie externe, à propos de 28 cas. Oto-rhino-laryngologie et pathologie cervico- faciale 118: 344-351.
- Respler DS, Jahn A, Pater A, Pater MM (1987) Isolation and characterization of papillomavirus DNA from nasal inverting (Schneiderian) papillomas. Ann Oto-Rhino-Laryngol 96: 170-173.
- Macdonald, MR, Le KT, Freeman J, Hui MF, Cheung RK, et al. (1995) A majority of inverted Sino nasal papillomas carries Epstein-Barr virus genomes. Cancer 75: 2307-2312.
- Eggers G, Hling J, Hassfeld S (2007) Inverted papilloma of paranasal sinuses. Journal of Cranio-Maxillofacial Surgery 35: 21-29
- Lawson W, Ho BT, Shaari CM, Biller Hf (1995) Inverted papilloma: a report of 112cases. Laryngoscope 105: 228–88.
- Arends MJ, Wyllie Ah, Bird CC (1990) Papilloma viruses and human cancer. Hum Pathol 21: 686-698.
- Hizem A (2008) Le papillome inverse nasosinusien: du diagnostic au traitement.Thèse pour le diplôme d’état de doctorat en médecine. Monastir.
- Syrjanen KJ (2003) HPV infections in benign and malignant Sinonasal lesions. JClin Pathol 56: 174-81.
- Gaffey MJ, Frierson HF, Weiss LM, Barber CM, Baber GB,et al.(1996) human papilloma virus and Epstein Barr virus in Sino nasal Schneiderian papillomas. Am J Clin Pathol 106: 454-82.
- Michael R Macdonald MD, Kien T Le MD, Jeremy Freeman MD, May F Hui, Roy K Cheung,et al. (1995) A majority of inverted Sino nasal papillomas carriesEpstein-Bar virus genomes. Cancer 75: 307-12.
- Deitmer T, C Wiener (1996) Is there an occupational etiology of inverted papilloma of the nose and sinuses? Acta Otolaryngology 116: 762-5.
- Lee JT, Bhuta S, Lufkin R, Castro DJ (2003) Isolated inverting papilloma of the sphenoid sinus. Laryngoscope 113: 41-44
- Macdonald, MR, Le KT, Freeman J, Hui MF, Cheung RK, et al. (1995) A majority of inverted Sino nasal papillomas carries Epstein-Barr virus genomes. Cancer 75: 2307-2312.
- Myers EN, Fernau JL, Johnson JT, Tabet JC, Barnes EL(1990) Management of inverted papilloma. Laryngoscope 100: 481- 490.
- Peters BW, O'Reilly RC, Willcox TO Jr, Rao VM, Lowry LD, et al. (1995) Inverted papilloma isolated to the sphenoid sinus. Otolaryngology Head Neck Surg 113: 771-777.
- Suh KW, Facer GW, Devine KD, Weiland LH, Zujko RD (1997) Inverting papilloma of the nose and paranasal sinuses. Laryngoscope 87: 35-46.
- Outzen KE, Grøntveld A, Jørgensen K, Clausen PP, Ladefoged C (1996) Inverted papilloma: incidence and late results of surgical treatment. Rhinology 34: 114-118.
- A Refass, MA Hessissen, H Nadir, M Detsouli, Y Benchakroun. Transformation maligne d’un papillome inversé nasosinusien parmi une série de 11 cas.The Letter of Otorhinolaryngology and Head and Neck Surgery- no 294 - September-October 2004.