
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2019) Volume 4, Issue 2
Single Versus Continuous TAP blockage Technique for Management of Postoperative Hysterectomy Pain
2Anesthesia and ICU Department, Faculty of Medicine; Al Azhar University, Egypt
3Anesthesia and ICU Department, Faculty of Medicine; Ain Shams University, Egypt
Received Date: Jul 15, 2019 / Accepted Date: Jul 25, 2019 / Published Date: Aug 08, 2019
Copyright: ©Nancy Mohamed Ali Rund. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Transversus abdominis plane blockage technique is performed by administration of local anesthetic agent between the abdominal muscle anatomical planes to block the somatic nervous innervation. Value of continuously infused local anesthetic agents via indwelling catheters in TAP blockage is an area of growing research interest.
Aim: To compare the analgesic efficacy of single shot versus continuous transversus abdomin is plane (TAP) block in cases undergoing total abdominal hysterectomy.
Methodology: All research study subjects enrolled had provided a written informed consent. The research study involved 60 cases having ASA scoring status 1 to 2(according to American society of Anesthesiologist scoring system), aged 35 to 60 years and scheduled to undergo total abdominal hysterectomy cases. All patients were categorized into two research groups in a random manner; single shot TAP research group (n=30 cases) and continuous TAP research group (n=30 cases).
Results: VAS scoring (Visual Analog Scale for Pain) was statistically significantly lower among continuous TAP block research group in comparison to single shot TAP block research group at different time intervals,baseline,1 hour,12 hours 24 hours,36 hours 48 hours 60 hours (p values =0.000, 0.001, 0.001, 0.002, 0.026 consecutively).
Conclusion and Recommendations: TAP blockage prolong the analgesic duration, reduces the VAS scoring particularly in continuous approach more than single shot postoperatively and reduces the requirements for Opioid consumption overall.
Key Points
TAP blockage, Hysterectomy, Postoperative Pain
Introduction
Effective post-operative pain management in gynecological surgery is considered of paramount requirement to enhance recovery process. Minimization of the analgesic medication dosage is of cornerstone importance reducing over dosage toxicity issues [1,2,3].
Transversus abdominis plane blockage technique is performed by administration of local anesthetic agent between the abdominal muscle anatomical planes to block the somatic nervous innervation located between internal oblique and transversus abdominous muscle that innervates the dermal, parietal peritoneum and muscular structures of the anterior abdominal wall the since nerves originating from the ventral ramus of T6 to L1 are situated at the surgical incision sites lowering thepain scoring levels till 24hours postoperatively [4,5,6].
Prior research groups of investigators have shown that Transversus Abdominis Plane blockage is of great value in pain management in the abdominal surgery procedures [7,8,9,10].
Most research studies investigating Transversus abdominis plane blockage have used the single-shot approach. On the other hand,the characteristic sensory blockade duration after a single-shot Transversus abdominis plane blockage is about 6 to 12 hours, with a mean analgesic impact around 9 and half hours. Value of continuously infused local anesthetic agents via indwelling catheters in TAP blockage is an area of growing research interest [8,12,13].
Aim of the Work: To compare the analgesic efficacy of single shot versus continuous transverses abdominis plane (TAP) block in cases undergoing total abdominal hysterectomy.
Methodology
This study was carried out in Saudi Arabia, in Jeddah at a private hospital (Bugshan Hospital) for a period starting from October 2014 to November 2018. The research was conducted in a prospective manner on 60 cases candidates for total abdominal hysterectomy. All the patients were provided with an informed consent after receiving a full explanation of the nature and protocol of the study.
The research study involved 60 cases having ASA scoring status 1 to 2, aged 35 to 60 years and scheduled to undergo total abdominal hysterectomy cases were categorized into two research groups in a random manner single shot TAP research group (n=30 cases), continuous TAP research group (n=30 cases).
The exclusive research criteria involved allergy to any of the agents implemented in the research study, intellectual impairments or psychiatric diseases affecting sufficient communication, ipsilateral neurological lesions, hepatorenal functional impairments, participants and post-anesthetic care unit (PACU)nurses performing pain assessments were blinded to the group allocation. Study subjects have been managed by consultant gynecologists and anesthesiologists.
Pre anesthetic induction medication has been conducted using glycopyrrolate and midazolam. Noninvasive blood pressure, electrocardiography, pulse oximetryhas been monitored in a continuous manner. Induction of general anesthesia was performed by injecting thiopental sodium and remifentanil agents. After the cases had loss of consciousness, rocuronium agent has been injected and endotracheal intubation was conducted after 90 seconds of mask ventilation.
Desflurane have been used as an inhalational anesthetic agent and intravenous remifentanil have been infused and titrated for anesthesia maintenance. Besides the end-tidal carbon dioxide partial pressure has been sustained to be within 35 to 40 mmHg.
After endotracheal intubation, as the vital signs have been stable and research groups undergone TAP blockage using sonographic guidance. After positioning the case in a supine position, the intended insertion area of the catheter, have been sterilized using chlorhexidine-alcohol and covered with sterile drapes. A linear sonographic probe (5.0-13.0 MHz) has been used for identification of the external oblique abdominal muscle, internal oblique abdominal muscle and transversus abdominal muscle. Once the external oblique abdominal muscle, internal oblique abdominal muscle and transversus abdominal muscle wasvisualized at the sub costal line level located in betweenthe 8th and 10th ribs, the puncture zone and the sonographic probe have been sterilized. In single shot research group, the blockage was conducted using a 25-gauge, 100-mm nerve blockade needle(Uniever®; Unisis Corp., Tokyo,Japan) and an injection line was visualizedusing an “in-plane” sonographic-guided approach. As theneedle tip have been placed within the space between the internal oblique abdominal muscle and transversus abdominal muscle and negative aspiration have been established, 20mL of 0.2% ropivacaine was administered under direct sonographic guidance.
In the continuous research group, an 18-gaugeTuohy needle have been advanced using an in-plane approach till the anatomical plane between the internal oblique abdominal muscle and transversus abdominal muscle have been reached. After confirmation that the needle tip was situated within the plane between the two muscles, 20mL of 0.2% ropivacaine agent have been injected and a 20-gauge, three-orifice catheter (Perifix®; B. Braun Medical Inc., Allentown, PA, USA) was advanced 5-7 cm beyond the needle tip within the plane between the muscles. Then, the catheter was sutured in place with a 4-0 nylonthread. A transparent plaster (Tegaderm™; 3 M Corporation, St Paul, MN, USA) was used as an occlusive dressing. Continuous infusion Via the catheter have been started within the recovery unit by usage of 0.2% ropivacaine at a basal rate of 3mL/hour, a bolus dose of 4mL, and a lockout interval of 30 min. The catheter was removed 48 hours after the finishing the surgical procedure.
Results
Table 1 reveals the basic research criteria in which by comparing between Single-shot TAP Block and Continuous TAP Block research groups there was no statistical significant difference as regards age, ASA status I,II, weight, Height, BMI, anesthesia time (min)p values = 0.415, 0.573, 0.556, 0.814, 0.586, 0.107 consecutively.
Table 2 and Figure 1 reveal and display that there was no statistical significant difference between single shot TAP block and continuous TAP block research groups as regards SBP at different time intervals, baseline, 1 hour, 12 hours 24 hours, 36 hours, 48 hours and 60 hours (p values = 0.082, 0.112, 0.228, 0.062, 0.210, 0.393, 0.474 consecutively).
Table 3 and Figure 2 reveal and display that there was no statistical significant difference between single shot TAP block and continuous TAP block research groups as regards DBP at different time intervals, baseline, 1 hour, 12 hours, 24 hours, 36 hours, 48 hours and 60 hours (p values = 0.033, 0.878, 1.00, 0.334, 0.994, 0.611, 0.699 consecutively).
Table 4 and Figure 3 reveal and display that there was no statistical significant difference between single shot TAP block and continuous TAP block research groups as regards HR at different time intervals, baseline, 1 hour, 12 hours, 24 hours,36 hours, 48 hours and 60 hours (p values = 0.112,0.132,0.054,0.065, 0.900,0.0.95,0.182 consecutively).
Table 5 and Figure 4 reveal and display that VAS scoring was statistically significantly lower among continuous TAP block research group in comparison to single shot TAP block research group at different time intervals,baseline,1 hour,12 hours, 24 hours,36 hours, 48 hours and 60 hours (p values = 0.000,0.001,0.001,0.002,0.026 consecutively).
Table 6 and Figure 5 reveal and display that the total narcotic usage at 48 hours and 60 hours was statistically significantly lower among the continuous TAP research group (p values=0.001, <0.001 consecutively). On the other hand, there was no statistically significant difference between both research groups as regards sedation score and nausea score levels at 48 hours post-operative (p values=0.832,0.135 consecutively).
Table 1: Basic research criteria of Single-shot TAP Block and Continuous TAP Block
|
|
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value |
P-value |
Sig. |
|
Age (years) |
48.6 ± 13.5 |
45.8 ± 12.9 |
0.821• |
0.415 |
NS |
|
ASA status |
|||||
|
I |
22 (73.3%) |
20 (66.7%) |
0.317* |
0.573 |
NS |
|
II |
8 (26.7%) |
10 (33.3%) |
|
|
|
|
Weight |
73.5 ± 19.3 |
76.4 ± 18.6 |
0.593• |
0.556 |
NS |
|
Height |
168.4 ± 12.7 |
169.3 ± 16.5 |
0.237• |
0.814 |
NS |
|
BMI |
25.9 ± 6.4 |
26.7 ± 4.8 |
0.548• |
0.586 |
NS |
*: Chi-square test; •: Independent t-test
Table 2: SBPamong Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
|
SBP |
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value• |
P-value |
Sig. |
|
|
Baseline |
Mean ± SD |
123.16 ± 5.58 |
120.56 ± 5.80 |
1.769 |
0.082 |
NS |
|
Range |
110 – 135 |
110 – 129 |
||||
|
1 hour |
Mean ± SD |
112.20 ± 7.65 |
108.92 ± 8.09 |
1.614 |
0.112 |
NS |
|
Range |
100 – 120 |
90 – 120 |
||||
|
12 hours |
Mean±SD |
114.88 ± 1.13 |
115.28 ± 1.40 |
1.218 |
0.228 |
NS |
|
Range |
112 – 117 |
112 – 118 |
||||
|
24 hours |
Mean±SD |
115.60 ± 1.04 |
115.00 ± 1.38 |
1.902 |
0.062 |
NS |
|
Range |
113 – 117 |
113 – 118 |
||||
|
36 hours |
Mean±SD |
120.00 ± 1.35 |
120.40 ± 1.08 |
1.267 |
0.210 |
NS |
|
Range |
117 – 122 |
118 – 122 |
||||
|
48 hours |
Mean±SD |
122.64 ± 1.11 |
122.88 ± 1.05 |
0.860 |
0.393 |
NS |
|
Range |
120 – 124 |
121 – 125 |
||||
|
60 hours |
Mean±SD |
119.52 ± 0.96 |
119.32 ± 1.18 |
0.720 |
0.474 |
NS |
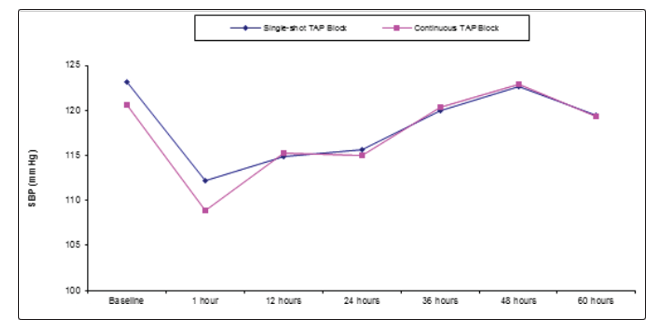
Figure 1: SBP within Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
Table 3: DBP among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
|
DBP |
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value• |
P-value |
Sig. |
|
|
Baseline |
Mean ±SD |
81.83 ± 9.51 |
76.50 ± 9.39 |
2.185 |
0.033 |
S |
|
Range |
60 – 95 |
60 – 90 |
||||
|
1 hours |
Mean ±SD |
77.83 ± 6.65 |
77.50 ± 9.80 |
0.154 |
0.878 |
NS |
|
Range |
65 – 95 |
60 – 95 |
||||
|
12 hours |
Mean ±SD |
77.50 ± 5.84 |
77.50 ± 9.63 |
0.000 |
1.000 |
NS |
|
Range |
65 – 90 |
60 – 95 |
||||
|
24 hours |
Mean ±SD |
78.79 ± 6.90 |
76.83 ± 8.46 |
0.973 |
0.334 |
NS |
|
Range |
65 – 90 |
60 – 95 |
||||
|
36 hours |
Mean ±SD |
79.60 ± 7.49 |
79.58 ± 7.65 |
0.008 |
0.994 |
NS |
|
Range |
70 – 95 |
65 – 95 |
||||
|
48 hours |
Mean ±SD |
72.67 ± 6.40 |
71.83 ± 6.23 |
0.511 |
0.611 |
NS |
|
Range |
60 – 85 |
60 – 85 |
||||
|
60 hours |
Mean ±SD |
73.83 ± 6.39 |
73.17 ± 6.88 |
0.389 |
0.699 |
NS |
|
Range |
60 – 85 |
60 – 85 |
||||
•: Independent t-test
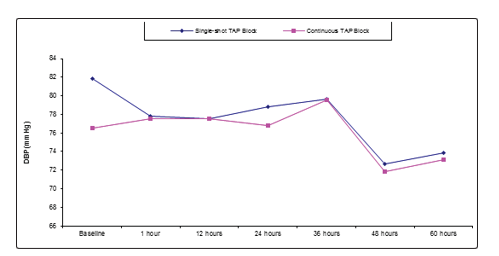
Figure 2: DBP among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
Table 4: HR among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
|
HR |
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value• |
P-value |
Sig. |
|
|
Baseline |
Mean ±SD |
87.33 ± 11.74 |
82.87 ± 9.61 |
1.613 |
0.112 |
NS |
|
Range |
60 – 110 |
66 – 110 |
||||
|
1 hour |
Mean ±SD |
84.63 ± 8.90 |
80.70 ± 10.92 |
1.529 |
0.132 |
NS |
|
Range |
59 – 100 |
65 – 110 |
||||
|
12 hours |
Mean ±SD |
84.13 ± 8.42 |
79.80 ± 8.61 |
1.971 |
0.054 |
NS |
|
Range |
62 – 96 |
65 – 100 |
||||
|
24 hours |
Mean ±SD |
85.43 ± 8.78 |
81.27 ± 8.35 |
1.884 |
0.065 |
NS |
|
Range |
60 – 98 |
64 – 100 |
||||
|
36 hours |
Mean ±SD |
86.04 ± 8.94 |
85.71 ± 9.25 |
0.126 |
0.900 |
NS |
|
Range |
62 – 102 |
72 – 115 |
||||
|
48 hours |
Mean ±SD |
81.43 ± 8.91 |
77.93 ± 6.96 |
1.696 |
0.095 |
NS |
|
Range |
58 – 98 |
66 – 94 |
||||
|
60 hours |
Mean ±SD |
82.37 ± 8.69 |
79.53 ± 7.53 |
1.349 |
0.182 |
NS |
|
|
Range |
59 – 98 |
66 – 100 |
|||
•: Independent t-test
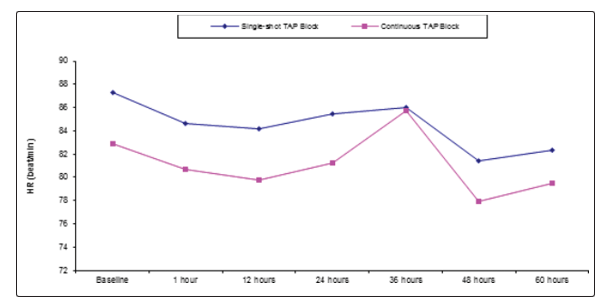
Figure 3: HR among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
Table 5: VAS among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
|
VAS |
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value• |
P-value |
Sig. |
|
|
1 hour |
Mean ±SD |
3.53 ± 1.17 |
2.40 ± 0.77 |
4.419 |
0.000 |
HS |
|
Range |
2 – 6 |
1 – 4 |
||||
|
12 hours |
Mean ±SD |
2.40 ± 0.50 |
1.82 ± 0.74 |
3.558 |
0.001 |
HS |
|
Range |
2 – 3 |
1 – 4 |
||||
|
24 hours |
Mean ±SD |
1.80 ± 0.50 |
1.33 ± 0.48 |
3.714 |
0.001 |
HS |
|
Range |
1 – 2 |
1 – 2 |
||||
|
36 hours |
Mean ±SD |
1.63 ± 0.43 |
1.10 ± 0.55 |
4.158 |
0.001 |
HS |
|
Range |
1 – 3 |
0 – 2 |
||||
|
48 hours |
Mean ±SD |
1.47 ± 0.51 |
1.03 ± 0.52 |
3.309 |
0.002 |
HS |
|
Range |
1 – 3 |
0– 2 |
||||
|
60 hours |
Mean ±SD |
1.5 ± 0.50 |
0.83 ± 0.57 |
2.287 |
0.026 |
HS |
|
Range |
1 – 3 |
0 – 2 |
||||
•: Independent t-test
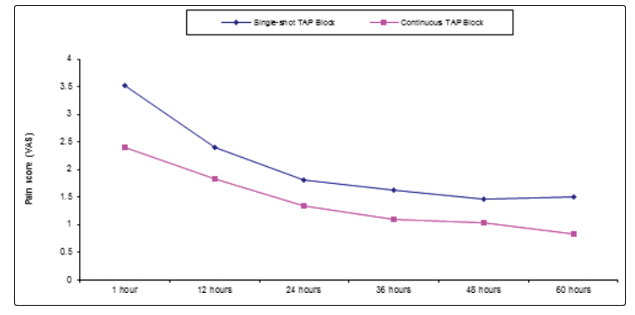
Figure 4: VAS among Single-shot TAP Block and Continuous TAP Block research groups at different time intervals
Table 6: Total narcotic usage, sedation scores and nausea scores postoperatively
|
|
Single-shot TAP Block (no. = 30) |
Continuous TAP Block (no. = 30) |
Test value• |
P-value |
Sig. |
|
|
Total Narcotic Usage at 48 Hours |
Mean ±SD |
75.87±17.82 |
3.525 |
3.525 |
0.001 |
HS |
|
Range |
40 - 85 |
30 - 70 |
||||
|
Total Narcotic Usage at 60 Hours |
Mean ±SD |
98.3±15.61 |
75.15±15.35 |
5.792 |
<0.001 |
HS |
|
Range |
60 - 125 |
50 - 105 |
||||
|
Sedation score at 48 hr postoperative |
Mean ±SD |
1.42±0.8 |
1.38±0.65 |
0.213 |
0.832 |
NS |
|
Range |
0 - 2 |
0 - 2 |
||||
|
Nausea score at 48 hr postoperative |
Mean ±SD |
1.65±0.49 |
1.45±0.53 |
1.518 |
0.135 |
NS |
•: Independent t-test
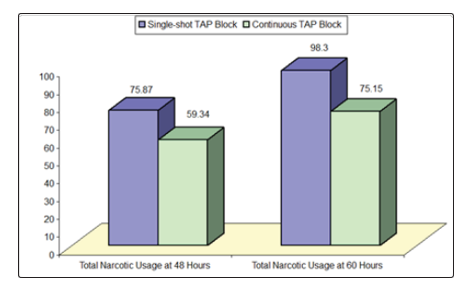
Figure 5: Total narcotic usage at 48 hours and 60 hours among research groups
Discussion
Cases scheduled to undergo total abdominal hysterectomy clinically experience severe pain issues postoperatively, requiring a multimodal approach to analgesia. The transversus abdominis plane (TAP) block seems to be an ideal approach [9-16].
A prior research study revealed and displayed that sonographic guided continuous TAP Blockage have similar analgesic impact as regards somatic pain and less analgesic effects concerning visceral pain issues than does IV- patient controlled analgesia with or without single-shot TAP blockage [9,17].
Besides, prior investigators have shown that continuous TAP blockade reduced in a statistically significant fashion postoperative urinary retention occurring from the usage of IV- patient controlled analgesia. Prior research studies have shown among their findings that pain occurring after laparoscopic cholecystectomy typically involves various constituents e.g. somatic incisional pain, visceral pain, and shoulder pain because of carbon dioxide pneumoperitoneum [12,19].
Various randomized controlled research studies have displayed the analgesic effectiveness of TAP blockage as an effective analgesic substitute to intravenous - patient controlled analgesia for postoperative pain management after abdominal surgery procedures [16].
On the other hand, most of those research efforts previously performed chiefly focused on analgesic issues regarding somatic incisional pain after single-shot TAP blockage technique. Furthermore in an interesting manner prior research teams of investigators have revealed and displayed that sonographic-guided TAP blockage supplies an efficient analgesic management concerning somatic originating pain, on the other hand it does not provide adequate analgesia as regards visceral originating pain [15,16].
Besides prior investigators have revealed and displayed among their findings that, nausea scoresas regards somatic pain 24 hours after surgical procedure have shown, that continuous TAP blockage had a somatic analgesic impact similar to that of intravenous - patient controlled analgesia with or without single-shot TAP blockage technique. Investigators have denoted that, sonographic-guided continuous TAP blockage is more valuable than intravenous - patient controlled analgesia, even though continuous TAP blockage could not effectively manage visceral originating pain [10].
Continuous TAP block is an attractive method for postoperative analgesia since it has the privilege of dermatomal coverage for the site of incision required for total abdominal hysterectomy incision (T10-L1dermatomes) besides it is simple to practice within the pre-operative period. In an interesting fashion a previous research study to the current study similar in approach and methodology have shown that the total anesthetic time was not statistically significantly different among the investigated research groups, since the technique is characterized by being simple and did not consume much time [1,10,14].
An important anatomical fact that, fewer blood vessels are situated within the transversus abdominal plane, that could result in delayed clearance of local anesthetic agent from the tansversus abdominal anatomical plane and therefore could decrease the clinical risk of systemic toxicity issues that could arise from rapid systemic absorption of local anesthetic agents[3,12].
Conclusion and Recommendation
TAP blockage prolongs the analgesic duration, reduces the VAS scoring particularly in continuous approach more than single shot postoperatively and reduces the requirements for opioid consumption overall. On the other hand, further research studies are needed in future research efforts to be performed on larger sample sizes and in multicentric fashion to elucidate our research study findings and verify them taking in consideration weight differences and anatomical variabilities among patients.
References
- Sharkey A, Borglum J, Blanco R, McDonnell J (2014) TAP block: past, present, and future. Am Soc Reg Anesth Pain Med 12: 15-17.
- Lee AR, Yi HW, Chung IS, Ko JS, Ahn HJ, Gwak MS, et al. (2012) Magnesium added to bupivacaine prolongs the duration of analgesia after interscalene nerve block. Can J Anaest 59:21-27.
- Ghatak T, Chandra G, Malik A, Singh D, Bhatia VK (2010) Evaluation of the effect of magnesium sulphate vs. clonidine as adjunct to epidural bupivacaine. Indian J Anaesth 54: 308-313.
- Atim A, Bilgin F, Kilickaya O, Purtuloglu T, Alanbay I, Orhan ME, et al. (2011) The efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing hysterectomy. Anaesth Intensive Care 39: 630-634.
- Huynh TM, Marret E, Bonnet F (2015) Combination of dexamethasone and local anaesthetic solution in peripheral nerve blocks: a meta-analysis of randomised controlled trials. Eur J Anaesthesiol 32: 751-758.
- Mahgoup AAN (2015) The addition of magnesium sulfate or dexamethasone tolevobupivacaine for ultrasound-guided supraclavicular brachial plexus block for upper-limb surgery: a double-blinded comparative study. Res Opinion Anesth Intensive Care 2: 116-120.
- Milan Z, Tabor D, McConnell P, Pickering J, Kocarev M, du FeuF,et al. (2011) Three different approaches to Transversus abdominis plane block: A cadaveric study. Med Glas (Zenica) 8: 181-184.
- McMorrow RC, Mhuircheartaigh RJ, Ahmed KA, Aslani A, Ng SC, Conrick-Martin I, et al. (2011) Comparison of transversus abdominis plane block vs spinal morphine for pain relief after Caesarean section. Br JAnaesth 106: 706-712.
- El-Dawlatly AA, Turkistani A, Kettner SC, Machata AM, Delvi MB, Thallaj A,et al. (2009) Ultrasound-guided transverses abdominis plane block: Description of a new technique and comparison with conventional systemic analgesia during laparoscopic cholecystectomy. Br J Anaesth102: 763-767.
- Ra YS, Kim CH, Lee GY, Han JI (2010) The analgesic effect of the ultrasound guided transverse abdominisplane block after laparoscopic cholecystectomy. Korean J Anesthesiol 58: 362-368.
- McDonnell JG, O’Donnell BD, Curley G, Hefferman A, Power C, Laffey JG. et al. (2007) Analgesic efficacy of transverses abdominis plane (TAP) block after abdominal surgery: A prospective randomized controlled trial. AnesthAnalg 104: 193-197.
- O’Donnell BD, McDonnell JG, McShane AG (2006) The transverses abdominis plane (TAP) block in open retropubic prostatectomy. Reg Anesth Pain Med 31: 91.
- Niraj G, Searle A, Mathews M, Misra V, Baban M, Kiani S, et al. (2009) Analgesic efficacy of ultrasound guided transversus abdominis plane block in patients under going open appendicectomy. Br J Anaesth 103: 601-605
- Barrington MJ, Ivanusic JJ, Rozen WM, Hebbard P (2009) Spread of injectate after ultrasound-guided subcostal transversus abdominis plane block: a cadaveric study. Anaesthesia 64: 745-750
- Gharaei H, Imani F, Almasi F, Solimani M (2013) The effect of ultrasound-guided TAPB on pain management after total abdominal hysterectomy. Korean J Pain 26: 374-378.
- Støving K, Rothe C, Rosen stock CV, Aasvang EK, Lundstrøm LH, Lange KH.et al.(2015) Cutaneoussensory block area, muscle-relaxing effect, and block duration of the transverses abdominis plane block: a randomized, blinded and placebo-controlled study in healthy volunteers. Reg Anesth Pain Med 40:355-362.
- Farag E, Guirguis MN, Helou M, Dalton JE, Ngo F, Ghobrial M, et al.(2015)Continuous transversusabdominis plane block catheter analgesia for postoperative pain control in renal transplant. J Anesth 29: 4-8.
- Kadam RV, Field JB (2011) Ultrasound-guided continuous transverse abdominis plane block for abdominal surgery. J Anaesthesiol Clin Pharmacol 27: 333-336.
- Petersen PL, Stjernholm P, Kristiansen VB, Torup H, Hansen EG, Mitchell AU, et al. (2012) The beneficial effect of transversus abdominis plane block after laparoscopic cholecystectomyin day-case surgery: a randomized clinical trial. Anesth Analg 115: 527-533.