
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Case Report - (2016) Volume 1, Issue 1
Single Umbilical Artery
Received Date: Aug 01, 2016 / Accepted Date: Aug 11, 2016 / Published Date: Aug 16, 2016
Copyright: ©Carlo Pafumi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
The Umbilical Artery Unica is found in 0.2 to 1.1% of all fetuses. Their presence of AOU in itself does not cause any harm to the fetus and newborn. Sometimes, however, this abnormality occurs associated with chromosomal abnormalities and other abnormalities Structural.
Introduction
The Umbilical Artery Unica is found in 0.2 to 1.1% of all fetuses. Their presence of AOU in itself does not cause any harm to the fetus and newborn. Sometimes, however, this abnormality occurs associated with chromosomal abnormalities and other abnormalities Structural. The chromosomal abnormalities account for about 5-10%; the most common are trisomy 13, 18 and 21. The non-chromosomal anomalies associated together account for about 22%: heart disease is the most frequent. 4-6% of fetuses with AOU in isolation have minor abnormalities at birth, whose ultrasound diagnosis is difficult or impossible. 25-30% of fetuses with AOU are suffering from intrauterine growth retardation (IUGR), and about a quarter of these born prematurely. Fetuses with AOU also feature a higher risk of death intrauterine and / or intrapartum.
Embryogenesis
The umbilical arteries develop from the allantois, a diverticulum of the yolk sac. Between 3 and 5 weeks of gestation, a transient common umbilical artery is normally present in all embryos, replacing a plexus of arteries around the allantois [1]. Subsequently, the common umbilical artery becomes shorter and right and left umbilical arteries advance within the body stalk, SUA can result from one of three mechanisms: primary agenesis of one of the definitive umbilical arteries, a secondary atrophy or atresia of a previously normal umbilical artery, or persistence of the common allantoic/umbilical artery.
Case
The clinical case we are referring to is for a 21 year old patient, primigravida at 37 weeks who is hospitalized at the Clinic of Obstetrics and Gynecology Santo Bambino Hospital of Catania for pelvic pain. The patient had no nothing to detect family history and personal. Morphological ultrasound had diagnosed the presence of AOU. The patient had refused to undergo amniocentesis and later he had executed a flow meter examination that was normal. The VII month the fetus had begun to show signs of IUGR characters
Results
The patient underwent a cesarean section because the fetus was in presentation Breech. The postoperative course was uneventful and the patient was discharged in IV day in good condition. The newborn, male, birth weight 2350 grams, which presented the 1st and 5th minute Apgar 9/10 Index, he has been hospitalized at the NICU for then be discharged after a few days without any problems.
Conclusion
There diagnosis of AOU, performed through a scan ultrasound transverse the cord, imply only that a percentage of fetuses the cord has a one artery can be bearer of some gender of malformation or chromosomopathy; not is, then, synonymous of alterations.
The management obstetrician is today very discussed is expected ultrasound detailed for exclude their presence of abnormalities associated, echocardiography, an advice genetics is the careful surveillance with controls ultrasound every 3 weeks for evaluate the growth fetal is, in third quarter, for evaluate the welfare fetal with their velocimetry. Amniocentesis is helpful mostly in presence of other abnormalities fetal.
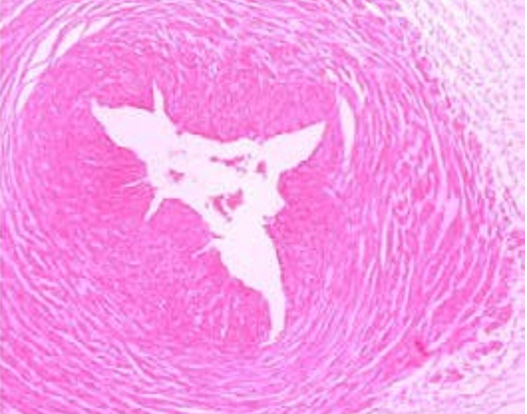
Figure 1: Single Umbilical Artery
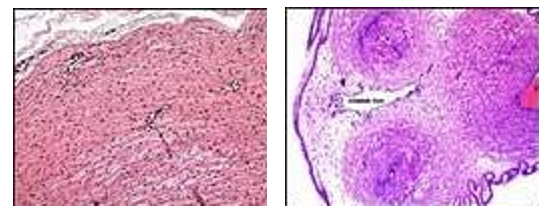
Figure 2 and 3: Histopathology.
References
- Granese R, Coco C, Jeanty P (2007) The value of single umbilical artery in the prediction of fetal aneuploidy: findings in 12,672 pregnant women. Ultrasuond Q 23: 117-121.
- Bianchi DW (2000) Diagnosis and management of fetal patient. McGraw Hill, New York: 827.
- Persutte WH, Hobbins J (1995) Single umbilical artery: a clinical enigma in modern prenatal diagnosis. Ultrasound in Ostetrics & Gynecology 6: 216.
- Naeye RL (1992) Disturbi del cordone ombelicale”. In: Disturbi della placenta, feto e neonato. Mosby-Year Book Inc, St Louis, MO 92.
- AIUM Practice Guideline for the Performance of Obstetric Ultrasound Examinations (2013).
- Gornall AS, Kurinczuk JJ, Konje JC (2003) Antenatal detection of a single umbilical artery: does it matter?. Prenat Diagn 23: 117-123.