
Journal of Traditional Medicine & Applications(JTMA)
ISSN: 2833-1389 | DOI: 10.33140/JTMA
Impact Factor: 1.02



Case Report - (2024) Volume 3, Issue 2
Siddha Interventions in the Treatment of Plantar Heel Pain – A Case Report
2Professor, Department of Varmam Sirappu maruthuvam, Sri Sairam Siddha Medical College, India
3Associate professor, Department of Udalkoorugal, Sri Sairam Siddha Medical College, India
4Sri Sairam Siddha Medical College and Research Center, Chennai 44 Tamilnadu, India
Received Date: Sep 03, 2024 / Accepted Date: Oct 28, 2024 / Published Date: Nov 13, 2024
Copyright: ©Â©2024 S Kanimozhi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kanimozhi, S., Amirtharaj, D., Adithya, R. S., Kavimathi, M. (2024). Siddha Interventions in the Treatment of Plantar Heel Pain
Abstract
Background: Pain is an unpleasant emotional and sensory experience linked to prospective or existing tissue injury. In the practice of orthopaedics, heel discomfort is frequently seen. One of the most typical characteristics of heel discomfort is inflammation of the plantar fascia. Calotropis gigantea, also referred to as vegetable mercury, is well recognized for its ability to reduce inflammation. Hot Fomentation, or otradam, is a typical method used to alleviate inflammation. It involves using packs containing therapeutic herbal powders heated to the proper temperature. Dispersing aggravated thodams (body components) is another benefit of otradam.
Aim & Objective: To explore the interventions available in the siddha system of medicine in the treatment of heel pain and to evaluate the efficacy of calotropis gigantea otradam for the same.
Materials & Methods: A 47-year-old female patient complained of heel pain that worsened in the morning just after she got out of bed and stood up straight after resting. pain-related sleep problems for the past month. The Calotropis gigantea leaves were fermented in heated bricks for ten days. (twice daily). Mankoski’s Pain Scale was used to evaluate the data gathered on pain perception.
Results and Conclusion: In this study calotropis gigantea leaves Fomentation on hot brick has favourable effects in reliving the pain. Pain reduced to grade 1 from grade 9 as assessed by Mankoski’s Pain scale. From the results it is proved that calotropis offers effective relief from heel pain.
Keywords
Calotropis, Pain, Fomentation, Kuthinkaalvatham, Mankoski’s Pain Scale
Introduction
One of the most prevalent foot disorders is heel pain. It is referred to by several names, including plantar fasciitis, jogger’s heel, tennis heal, and policeman’s heel. Heel pain is most frequently caused by mechanical reasons. Any pain or discomfort felt at or around the back of the foot is referred to as heel pain in general [1]. There are other terms used to refer to heel pain, including plantar fasciitis, policeman’s heel, jogger’s heel, and tennis heal [2]. Plantar fasciitis-related heel discomfort is characterized by soreness and pain behind the calcaneus’s medial tubercle on weight-bearing surfaces, especially just after rest, like when you first get out of bed in the morning. Disorders of the plantar fascia (PF) are prevalent in adulthood [3]. The plantar aponeurosis, or PF, is a robust connective tissue structure that aids in preserving the foot’s longitudinal arch [4]. The Plantar fascia is arranged as three bundles: central, lateral and medial. The central band is the thickest of all the three. It takes origin from the medial tubercle of the calcaneus. Distally, it divides into five digitations that insert into the metatarsophalangeal joints [5].
Plantar fasciitis is the most common injury of the Plantar fascia and is estimated to induce more than 1 million patients to seek treatment annually [6]. Biomechanical risk factors include things like foot abnormalities, inappropriate footwear, an elevated body mass index, and activities that entail extended walking, jogging, or standing that impose repetitive stress on the PF [7,8]. A physical examination and the patient’s clinical history are typically used to diagnose plantar fasciitis. The primary symptoms include stiffness and soreness in the morning or pain when you first start moving after a period of inactivity. Upon physical examination, there is soreness at the PF’s origin as well as reduced ankle dorsiflexion and toe extension [9].
Plantar fasciitis is currently treated with a variety of conventional treatments, including calf stretching, foot taping, manual therapy (joint mobilization and manipulation; mobilization of soft tissue near sites of nerve entrapment and passive neural mobilization techniques), foot orthoses, oral and injectable anti-inflammatories, and night splints [10,11]. Surgery usually occurs as an option after at least six months of unsuccessful conservative treatment [12]. Analgesic drugs are often used to relieve pain. The medicinal plants are the primary source of traditional medicine in Siddha. They include a significant number of chemical elements that serve as medications to alleviate suffering in humans [13]. Ottradam is one of 32 kinds of external medicines. Ottradam (fomentation) is the application of hot or cold packs to painful spots. It is frequently performed with materials heated to the suitable temperature. Ottradam (fomentation) is a non-pharmacological therapy in the Siddha medical system that is used to treat a variety of infectious and inflammatory illnesses.
It can be defined as a technique for rhythmically compressing and relaxing a hot or cold paste, cloth sacks, or vessels on the regions that are affected. It’s also known as otral. A single direct method uses dry heat to cause perspiration.
1. Paguthiudalotradam (localized body fomentation)
2. Mutrudalotradam (Generalized body fomentation)
Various types of otradam are mentioned in Siddha system.
Kizhiotradam or Otradapottani or Pottani
It is characterized as the forceful pressure or placement of dry or wet medicinal bundles into the afflicted area with no rhythm. In this process, dry herbal powders, dry raw pharmaceuticals, or crushed fresh leaves are wrapped in kada cloth and tied into a little bundle known as kizhi. The bundle is then immersed in hot gingelly oil, and mild fomentation is applied to the affected portions [14].
Kali Otradam [15].
Boiled rice, grains, or other seeds undergo boiling with water, milk, or juice and then converted into cataplasm. It is maintained in a cotton pouch and gently administered to the body. It is a single direct method that uses dry heat to cause perspiration. Bronze, iron, rod, sand, fabric, and mud pots are all heated and employed for fomentation to relieve pain [16]. In the present case study, we put calotropis leaves on the brick and applied fomentation directly to the afflicted area. According to the text pathartha guna vilakam moola varkam,this eruku otradam is specifically suggested for treating heel pain and vadha-dominated disorders. Calotropis gigantea is also known as milkweed (Erukku) in Tamil. It belongs to the family Apocyanaceae. Its leaves include chemical compounds such as alkaloids, glycosides, and mudarine. It has vital functions such as anti-inflammatory and analgesic [15,17]. Furthermore, the fomentation technique is one of the most widely used modalities for treating chronic aches, with little adverse effects. There have been a few published research that have looked into the usefulness of calotropis fomentation in treating plantar heel pain. Because the plantar fascia is wounded, regular practice of stretching activities followed by fomentation will improve the tone and strength of the fascia and surrounding tissue. Furthermore, the mentioned research lack rigorous scientific methodology for outcome measurement and study design. A case report is one of the greatest ways to illustrate the efficacy of any drug used in therapy. Thus, we wanted to demonstrate the siddha interventional method-Calotropis fomentation (otradam) coupled with specific exercises - in the management of plantar heel pain using a case study.
A single case study with calotropis hot fomentation experimental design was used because no clinical trials have studied the effects of fomentation on heel pain. It is a great beginning point for determining the necessity for additional investigation. The entire care of heel pain would include the diagnosis of external and internal cause factors, as well as medication aimed at relieving the pain.
Case Presentation
Basic Information of Patient
Age: 47-years
Gender: Female
Height: 5'3''
Weight: 65kg
Occupation: Mineral water supplier
Chief complaints: Severe localized pain on the right medial plantar region
History of Present Illness
A 47-year-old woman presented to the OPD of the Department of Pothumaruthuvam, Sri Sairam Siddha Medical College and Research Centre, with localized pain on the right medial plantar calcaneus that had begun more than a month earlier. The pain was described as “stabbing” and is most intense in the morning, right after getting out of bed and standing up after a time of rest. Although the pain diminished throughout the day, she continued to feel it when walking and doing weight-bearing exercises. In general, she couldn’t stand for more than an hour or walk for more than 15 minutes without experiencing agony. The patient reported no radiating pain or numbness along with the symptoms, and she denied having any recent falls or injuries.
Due to the agony, the patient initially went to an orthopedic hospital and was given NSAIDs, which reduced part of the pain, but the pain persisted after ceasing the medicine. She was an energetic woman who distributed mineral water to residential areas. She used to carry the water can on her bicycle, which she rides for approximately two hours each day. Again, her regular activities became hampered. She then went to a siddha physician, where she was asked to be admitted and have an external procedure, but because she was a daily wager and the family’s sole breadwinner, she was unable to be admitted. After a month, the pain became so intense that it impeded her daily activities. Hence, sought our hospital for a better line of treatment.
History of Past Illness
No history of Diabetes mellitus, Hypertension or other systemic illness
• Family History: All family members are said to be healthy
• Menstrual history: Normal 29 days cycle
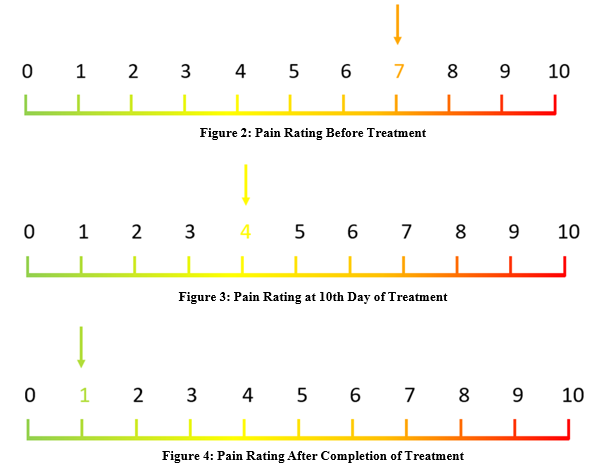
• Initial assessment: Pain was scored on Mankoski’s Pain Scale as a 9/10 in the morning and a 7/10 altogether [18].
Physical Examination
Pain was scored on Mankoski’s Pain Scale as a 9/10 in the morning and a 7/10 altogether [18]. The right arch appeared normal, and there were no obvious anomalies in either foot. Palpation revealed +3/4 severe soreness along the midline of the right heel; however, she reports that palpation provides better pain alleviation. She exhibited a normal range of motion in her feet and ankles. Her gait appeared to have a minor pronation of the right foot, causing difficulties with walking and supporting weight. The patient experienced pain in the medial plantar region of the heel, which was particularly noticeable when pressure was applied during physical examination or walking.
Findings on Examination
• Despite having flat and mobile feet, she struggled to roll in and out excessively.
• She took extremely long strides and landed much in front of his center of mass (hip/pelvis).
• Hard landing (as detected by sound).
• Weak gluteal muscles, resulting in difficulty holding a single leg bridge and difficulty when lying on her side.
• Excellent calf and big toe mobility.
Treatment Protocol
In this case as the patient was unable to get admitted and had little response with internal medicines, so external therapy was adopted as primary option and the procedure was given in the OPD.
Treatment
Calotropis – Brick Hot Fomentation
A red brick has been heated in a fire for ten minutes. 5-6 fresh Calotropis leaves are kept on the hot brick. Neem oil is administered to the foot before beginning the treatment. The patient is then asked to place her right foot on the calotropis leaves on the block, which protects the plantar skin from direct heat adverse effects. The foot is placed on the leaves until the temperature drops to normal. This technique is carried out twice a day for ten days.

Figure 1: Process of Ottradum
A: Calotropis gigantea leaves
B: Firewood
C: Heated brick (Brick heated on the fired wood)
D: Fomentation on plantar heel with heated brick and Calotropisgigantea leaves
Formulated a Home Workout Regimen that Comprised Three Key Exercises
• Increased muscle strength on the inner side of the foot.
• Strengthening hip muscles.
• Strengthening calf muscles while stretching the Plantar fascia.
We maintained track using a basic spreadsheet. Over the course of ten days, we assessed improvement every three days. After 5 days, we were able to gradually increase the intensity of the exercises and the distance she walked.
Pain Assessment Tool
Pain is assessed using Mankoski’s Pain scale. In this the intensity of pain is marked in a 10cm line between Two ends refers no pain and extreme pain. This is done before and after treatment.
|
Score |
Symptoms |
|
0 |
Pain free |
|
1 |
Very minor annoyance – occasional minor twinges |
|
2 |
Minor annoyance – occasional major twinges |
|
3 |
Annoying enough to be distracted |
|
4 |
Can be ignored if you are really involved in your work , but still distracted |
|
5 |
Can’t be ignored for more than 30 minutes |
|
6 |
Can’t be ignored for any length of time , but you can still go to work and participate in social activities |
|
7 |
Makes it difficult to concentrate, interferes with sleep. You can function with effort |
|
8 |
Physical activity severely limited. You can read and converse with effort. Nausea and dizziness set in as factors of pain |
|
9 |
Unable to speak. Crying out or moaning uncontrollably – near delirium |
|
10 |
Unconsious. Pain makes you pass out. |
Table 1: Mankoski’s Pain Scale - Numeric Pain Intensity Scale Ranging From 0 – 10
Diagnosis
Outcome of Therapy
Her pain levels had significantly decreased at the end of the ten days—mostly to 0/10, sometimes to 1/10, and on one occasion to 2/10 following an exceptionally long day of standing. She was pleased with the outcome. She was instructed to continue her fitness regimen for an additional three weeks. It is crucial that we continue to follow up in order to maintain the progress we have made in terms of strength gains and other areas even after the treatment session has ended.
Discussion
The results of this study have demonstrated thatfollowing a treatment protocol of Calotropis fomentation andcombined exercises for a patient, with plantar heel pain, had improvements in function, pain and strengthening of gluteal muscles.
|
S.No |
Etiology |
Associated Symptoms |
|
1. |
Neuropathies |
Diabetes mellitus, alcohol abuse, vitamin deficiency |
|
2. |
Tarsal Tunnel syndrome |
Burning sensation in medial plantar region |
|
3. |
Acute calcaneal fracture |
Direct trauma, unable to bear weight |
|
4. |
Calcaneal stress fracture |
Insidious onset of pain, repetitive loading |
|
5. |
Achilles tendinitis |
Posterior calcaneal/tendon pain |
|
6. |
Heel contusion |
Direct fall on heel with bone/fat pad pain |
|
7. |
Plantar fascia rupture |
Sudden plantar heel pain and ecchymosis |
|
8. |
Posterior tibial tendinitis |
Posterior medial ankle/foot pain |
|
9. |
Retrocalcaneal bursitis |
Pain in the retrocalcaneal region |
|
10. |
Systemic arthritis (e.g., rheumatoid arthritis, Reiter syndrome, psoriatic arthritis |
Multiple joint pain, bilateral heel pain |
Table 2: Differential Diagnosis of Plantar Heel Pain [12].
The findings of this study show that following a therapy schedule of Calotropis fomentation and combination exercises for a patient with plantar heel pain improved function, discomfort, and gluteal muscular strength. Plantar fasciitis is the most common plantar fascia condition and a leading cause of heel pain in the general population [9]. Plantar fasciitis is a low-grade inflammatory process in which repeated microtrauma causes microtears that trigger an inflammatory response. This stress-related kind of plantar fasciitis is common in sports, obese people, and those who work standing or walking for long periods of time. Other plantar fascia diseases include fibromatosis, xanthoma, rheumatoid nodule, and clear cell sarcoma. Heel pain can also result from prolonged weight bearing. Painful heel fat pad is frequently misdiagnosed as plantar fasciitis, despite the fact that the discomfort is slightly more posterior in location. In certain circumstances, edema and fibrosis of the heel fat pad are present in the absence of plantar fascial modifications.
Calcaneal stress fractures are a prevalent cause of chronic heel discomfort. Patients with calcaneal stress fractures and plantar fasciitis may have similar histories, as both conditions are caused by overuse and exacerbated by weight bearing activities. In such circumstances, MRI is extremely sensitive and can provide a definitive diagnosis [19-24]. Hot fomentation transmits heat across the region that is affected. This heat promotes the release of bradykinin and nitric oxide, which function as vasoactive mediators and enhance blood flow at the site of tissue damage, resulting in healing by improving the supply of nutrients and oxygen [25]. The analgesic effect of heat Accelerates leucocyte and antibody trafficking to the damaged area [26]. Heat allows oxygen to be more easily released from hemoglobin and delivered to tissues in need [27]. Heat application inhibits Aδ fibers and C type fibers, which cause acute and chronic pain, respectively [28]. Fomentation (Ottradam) activates the temperature-sensitive nerve endings (thermoreceptors) that create signals that prevent the transfer of pain signals to Brain and spinal cord [29]. Lupeol, a pentacyclic triterpenoid found in the latex of Calotropis gigantea leaves, works as an anti-inflammatory drug by inhibiting the generation of pro-inflammatory mediators [30,31].
Conclusion
Heel pain can make it difficult to walk and participate in regular activities. Inaddition to internal medicines various external inerventional therapies are available in siddha system. This Calotropis fomentation successfully controls heel pain. Reliability and treatment adherence are key for achieving positive outcomes. The calotropis fomentation resulted in an improvement in the patient’s symptoms and overall health. A mix of fomentation and hip strengthening exercises could potentially aid with plantar heel pain. The single case study design restricts generalizability, but the findings indicate that more controlled studies are needed to determine the efficacy of calotropis fomentation for heel pain.
References
- DeMaio, M., Paine, R., Mangine, R. E., & Drez, D. (1993). Plantar fasciitis. Orthopedics, 16(10), 1153-1163.
- Soundberg, S., & Johnson, K. (1991). Painful conditions of the heel. Disord Foot Ankle Med Surg Manag, 2, 1382-1396.
- Thomas, M. J., Roddy, E., Zhang, W., Menz, H. B., Hannan,M. T., & Peat, G. M. (2011). The population prevalence of foot and ankle pain in middle and old age: a systematic review. Pain, 152(12), 2870-2880.
- Jeswani, T., Morlese, J., & McNally, E. G. (2009). Getting to the heel of the problem: plantar fascia lesions. Clinical radiology, 64(9), 931-939.
- Stecco, C., Corradin, M., Macchi, V., Morra, A., Porzionato, A., Biz, C., & De Caro, R. (2013). Plantar fascia anatomy and its relationship with A chilles tendon and paratenon. Journal of anatomy, 223(6), 665-676.
- Riddle, D. L., & Schappert, S. M. (2004). Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors. Foot & ankle international, 25(5), 303-310.
- Huang, Y. C., Wang, L. Y., Wang, H. C., Chang, K. L., & Leong, C. P. (2004). The relationship between the flexible flatfoot and plantar fasciitis: ultrasonographic evaluation. Chang Gung medical journal, 27(6), 443-448.
- Van Leeuwen, K. D. B., Rogers, J., Winzenberg, T., & van Middelkoop, M. (2016). Higher body mass index is associated with plantar fasciopathy/‘plantar fasciitis’: systematic review and meta-analysis of various clinical and imaging risk factors. British journal of sports medicine, 50(16), 972-981.
- Goff, J. D., & Crawford, R. (2011). Diagnosis and treatment of plantar fasciitis. American family physician, 84(6), 676-682.
- McPoil, T. G., Martin, R. L., Cornwall, M. W., Wukich, D. K., Irrgang, J. J., & Godges, J. J. (2008). Heel pain—plantar fasciitis. journal of orthopaedic & sports physical therapy, 38(4), A1-A18.
- Crawford, F., Thomson, C. E., & Cochrane Bone, Joint and Muscle Trauma Group. (1996). Interventions for treating plantar heel pain. Cochrane Database of Systematic Reviews, 2009(4).
- Thomas, J. L., Christensen, J. C., Kravitz, S. R., Mendicino,R. W., Schuberth, J. M., Vanore, J. V., ... & Baker, J. (2010). The diagnosis and treatment of heel pain: a clinical practice guideline–revision 2010. The Journal of Foot and Ankle Surgery, 49(3), S1-S19.
- Kumar, D., & Kumar, S. (2015). Calotropis gigantea (L.) Dryand-A review update. Indian Journal of Research in Pharmacy and Biotechnology, 3(3), 218.
- Karthi, S., Visweswaran, S., Sivakkumar, S., Mariappan, A., & Banumathi, V. (2022). Integrative health care for siddha system in chronic pain management. Int. J. Adv. Res. Biol. Sci. 9(10): 103-105.
- J Jeyavenkatesh1, G Senthilvel2, P Saravanapandian3, S Rojaramani4, AKarthikeyan. SiddharSamanaMarutthuvam (Siddha balancing therapies) –Anovel way for treatingdiseases.Int J of Allied Med Sci and Clin Res 2018; 6(3): 713-722.
- S Sankaranarayanan. S.Praveena, D.Thabashini, A.P.Uma. Medical taxonomy of Angiosperms, Detailed Discrimination of Fomentation (Ottradam) in Siddha System. International Journal of Current Research in Medical Sciences 2017. 3(7): 108-111.
- Mandal, S. (2023). Calotropis gigantea: A brief Study on Phytochemical and Pharmacological Profile. Asian Journal of Pharmaceutical Research, 13(1), 34-40.
- Douglas, M. E., Randleman, M. L., DeLane, A. M., & Palmer,G. A. (2014). Determining pain scale preference in a veteran population experiencing chronic pain. Pain Management Nursing, 15(3), 625-631.
- Theodorou, D. J., Theodorou, S. J., Farooki, S., Kakitsubata, Y., & Resnick, D. (2001). Disorders of the plantar aponeurosis: a spectrum of MR imaging findings. American Journal of Roentgenology, 176(1), 97-104.
- Leach, R. O. B. E. R. T., Jones, R. O. B. E. R. T., & Silva, T.H. O. M. A. S. (1978). Rupture of the plantar fascia in athletes.JBJS, 60(4), 537-539.
- Narváez, J. A., Narváez, J., Ortega, R., Aguilera, C., Sánchez, A., & Andía, E. (2000). Painful heel: MR imaging findings. Radiographics, 20(2), 333-352.
- Theodorou, D. J., Theodorou, S. J., Kakitsubata, Y., Lektrakul, N., Gold, G. E., Roger, B., & Resnick, D. (2000). Plantar fasciitis and fascial rupture: MR imaging findings in 26 patients supplemented with anatomic data in cadavers. Radiographics, 20(suppl_1), S181-S197.
- Grasel, R. P., Schweitzer, M. E., Kovalovich, A. M., Karasick, D., Wapner, K., Hecht, P., & Wander, D. (1999). MR imaging of plantar fasciitis: edema, tears, and occult marrow abnormalities correlated with outcome. AJR. American journal of roentgenology, 173(3), 699-701.
- Rosenberg, Z. S., Beltran, J., & Bencardino, J. T. (2000). MR imaging of the ankle and foot. Radiographics, 20(suppl_1), S153-S179.
- Freiwald, J., Magni, A., Fanlo-Mazas, P., Paulino, E., Sequeira de Medeiros, L., Moretti, B.,... & Solarino, G. (2021). A role for superficial heat therapy in the management of non-specific, mild-to-moderate low back pain in current clinical practice: A narrative review. Life, 11(8), 780.
- Nurcan, Ç., & Karadag, M. (2015). Superficial heat and cold applications in the treatment of knee osteoarthritis. Osteoarthritis-Progress in Basic Research and Treatment In Tech, 249-64.
- Sembulingam, K., & Sembulingam, P. (2012). Essentials of medical physiology. JP Medical Ltd.
- D. Amarnath, A. Nithya Sri, S. Uthrapathi et al. Mechanism of ottradam(Fomentation). European Chemical Bulletin 2023. 12(7): 1186-1192.
- Fernández, M. A., de las Heras, B., Garcia, M. D., Sáenz, M. T., & Villar, A. (2001). New insights into the mechanism of action of the anti-inflammatory triterpene lupeol. Journal of Pharmacy and Pharmacology, 53(11), 1533-1539.
- Kumar, H., Sharma, S., & Vasudeva, N. (2021). Pharmacological profile of Calotropis gigantea in various diseases: A profound look. Int J Creat Res Thoughts, 9(2), 2987-96.
- Dr. U. Satyanarayana, Dr. U. Chakrapani - Biochemistry (with clinical concepts and case studies ), Elsevier publisher, 6th edition –2021. Pg no - 436.