


Case Report - (2023) Volume 1, Issue 2
Riga-Fede Syndrome : A Rare Case Report With Literature Review
2Department of Periodontics and Endodontics, India
3Department of Restorative dentistry, India
4Department of Oral Pathology and Microbiology, Private dental practice, India
Received Date: Jul 25, 2023 / Accepted Date: Aug 26, 2023 / Published Date: Sep 15, 2023
Copyright: ©Ã?©2023 Saurabh R. Nagar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Nagar, S. R., Deshmukh, Z. S. K., Fernandes, G., Bhandare, P. R., Shah, P. (2023). Riga-Fede Syndrome : A Rare Case Report With Literature Review. Transl Med OA, 1(2), 50-55.
Abstract
Riga-Fede syndrome is characterised as an ulcerative lesion that originates on the ventral surface of a neonate’s tongue due to vigorous back and forth movements of the tongue over the precociously erupted mandibular anterior teeth. This condition has been receiving discernible attention as a progressing condition with escalating case reports over the years. The aetiology of this issue is not precisely deduced; however, there have been multiple treatment options dis- covered that have secured success with higher precision. The purpose of this research paper is to exhibit various case reports and aetiologies responsible for this disease, as well as an explanation of different treatment plans depending on the status of the tooth, that is, the mobility of the tooth and the precarious chances of aspiration. Moreover, radiographic study to visualise if it is a supernumerary or a primary regular tooth and if it is associated with hindrance in breast-feed- ing causing soft tissue injuries and the state of the child’s health. A 28-day-old female infant was presented to the oral pathology clinic with a natal tooth exhibiting grade 2 mobility along with a lesion on the ventral surface of the tongue, leading to the clinical diagnosis of Riga-Fede disease. The treatment performed, consisting of the extraction of natal teeth, was selected as the treatment of choice over more conservative treatments for the rapid resolution of the lesion and the limited risk of inadequate nutrient intake since the tooth was interfering with the feeding process. Following the extraction of the tooth, it underwent microscopic studies to identify diverse changes associated with the erupted tooth. There was regular monitoring of the patient, and complete wound healing was observed after 4 weeks. The proposed treatment was successful, and the patient is still in follow-up without recurrence of the lesion after one year. This paper presents a concise review of the literature about neonatal teeth and their role in Riga-Fede disease.
Keywords
Riga-Fede Syndrome; Tongue; Oral Pathology
Background
A chronological sequence is generally associated with normal eruption that involves the eruption of lower anterior as the first primary tooth at around 6 months of age. Rarely, teeth can appear in the oral cavity at birth and these teeth are called natal teeth. Natal tooth/teeth are defined as those which are present at birth and neonatal tooth/teeth are those which are seen within 30 days of life in an infant’s oral cavity. Teeth which erupt before the normal eruption time are often called as congenital teeth, predeciduous teeth, fetal teeth, dentitia pracoex, dens canntalis, infancy teeth, precocious dentition and although the cause is yet unknown, it is often attributed to . The prevalence of natal teeth is presently found to be between 1 in 2000 to 3500 live births with a general predilecition towards the female gender. The exact cause of such tooth / teeth is still unknown but factors such as infections, febrile and pyretic conditions, trauma during delivery, malnutrition, hormonal imbalance, environmental toxins, maternal exposure to chemicals and tooth germ anomalies often pose as associated risks. These teeth can cause ulcers on the ventral surface of the tongue, lip, and the mother’s breast characterizes the rare pediatric condition called Riga-Fede Disease.
This disease appears as an ulcerated area on the ventral surface of the tongue (most common site in neonates and infants) as a result of a benign ulcerative process of the tongue and frenulum, owing to repetitive trauma caused by the process of eruption of the primary lower central incisors [2]. This lesion eventually progresses to an enlarged, fibrous lesion in the form of an ulcerative granuloma. The treatment depends on the tooth’s mobility and the risk of aspiration or swallowing; whether it is supernumerary or regular primary teeth; whether it is causing interference in breastfeeding; breast and oral soft tissue injuries; and the general state of child’s health. The clinical characteristics of natal and neonatal teeth may resemble natural primary dentition or may be conical in shape but histologically it may show different enamel, dentin, cementum and pulp changes. Mostly they depict a hypoplastic enamel, dentin and pulp.
Case Presentation
A 28 days old female infant was referred to the Oral Pathology department for ulceration on the ventral surface of the tongue (13 mm diameter) and difficulty in suckling because of the natal teeth. Clinical examination revealed a tooth with sharp incisor edge and grade two mobility. The ventral surface of the tongue showed a 5 × 8 mm ulcer extending from under border of the tongue to lingual frenulum. Feeding and nutrition of the baby was getting affected (Figure 1). The extraction of natal teeth was selected as treatment of choice, over more conservative treatments, for the rapid resolution of the lesion and for the limited risk of inadequate nutrients intake. The extracted teeth underwent a macroscopic and microscopic examination except for the irregular spaces in the region close to the amelodentinal union and the histological ground section that revealed a thin enamel layer with varying degrees of mineralization to an absence of enamel in some regions.
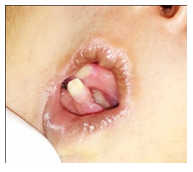
Figure 1: Ulceration on ventral surface of tongue in the index case
On ground sectioning of the tooth, it showed hypoplastic enamel with reduced thickness and loss of enamel at few places. There was presence of atubular osteodentin along with alterations in the atypical dispositions of dentinal tubules. Moreover, there existed irregular dentin in the cervical portions and interglobular dentin in the coronal region. The enamel rods showed a fish scale pattern and enamel spindles were seen focally. Predominantly tubular dentin was present. Dentinoenamel junction was not scalloped which was similar to deciduous teeth (Figure 2.1, 2.2, 2.3, 2.4). The complete healing of the lesion took 4 weeks; subsequently, the infant, revised at the 1-year follow-up visit.

Figure 2.1: Ground section of neonatal tooth showing Enamel.
Enamel is the outermost layer of the tooth, constituting tightly packed mineralized crystals.
In neonatal teeth, the enamel may appear thin and poorly mineralized, with poorly defined crystals than in mature teeth. It also exhibits irregular surface with a substantial amount of hypoplasia and enamel anomalies.
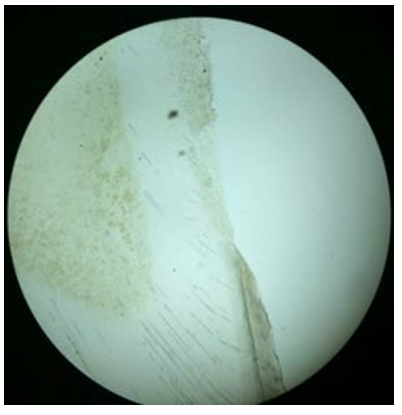
Figure 2.2: Ground section of neonatal tooth showing Dentin.
Dentin is the layer beneath the enamel, containing less inorganic content with greater porosity and leathery texture in contrast to mature teeth. The dentin in neonatal teeth may also show wider dentinal tubules (small channels that run through the dentin), indicative of rapid dentin formation, with higher amounts of mineralization.
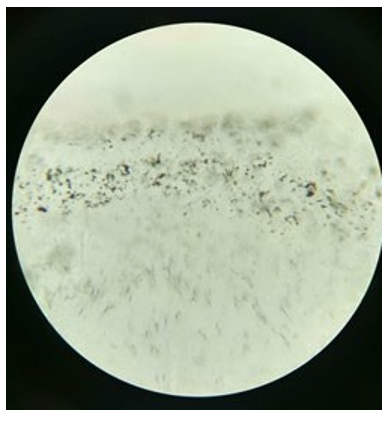
Figure 2.3: Ground section of neonatal tooth showing Tomes granular layer
A specialized layer of zone called Tomes granular layer allocated at the interface between dentin and cementum in mature teeth, is a hypomineralized area of radicular dentin; formed due to coalescing and looping of the terminal ends of the dentinal tubules. In neonatal teeth, this layer may ill-defined and disorganized compared to mature teeth, since these teeth are under developed and the dentin layer is partially mineralized. This is because neonatal teeth are still developing, and the dentin layer is not fully mineralized. Subsequently, the Tomes granular layer is yet to be entirely functional, and the dentin formation may be incomplete or irregular.

Figure 2.3: Ground section of neonatal tooth showing Pulp cavity.
The dental pulp is the most vital part of the tooth structure, filled with vascular tissue, neural tissue and connective tissue. In neonatal teeth, the dental pulp, is similar in structure and function to the pulp in mature teeth. Nevertheless, in neonatal teeth pulp tissue may be more exposed and vulnerable as a result of thinner, disorganized enamel layer. In fact, this property can en route to subsequent infections and hypersensitivity to changes in the temperature or chemical irritation, due to its high density of nerve endings.
Histopathology
Histologically, Riga-Fede syndrome is characterized by ulcerated and inflamed tissue with mixed acute and chronic inflammation. It typically exhibits a superficial necrosis of the mucosa with an inflammatory infiltrate on the tongue and sometimes the lower lip. The acute inflammation consists of neutrophils, while the chronic inflammation is characterized by lymphocytes, plasma cells, macrophages, mast cells and a predominance of eosinophils. It is, therefore, a cause of eosinophilic ulcers. Atypical histiocytic granulomas may also be seen.
The surface of the ulcerated tissue may show areas of granulation tissue with proliferating fibroblasts and new blood vessels. In some cases, there may be signs of bacterial infection, with colonies of bacteria present in the tissue. Neutrophilic infiltration presents as an integral part of the ulcer and the surrounding tissue, which is a prime indication of inflammation. The epithelium encircling the ulcer is often hyperplastic, that is an increased number of cells. Moreover, there are a few noted cases which prove the chances of these lesions being permeated with bacteria or viral infections, which can be seen in microscopic examination [2].
Following the excisional biopsy, based on the clinicopathological findings, it is mandatory to deduce the syndrome from other differential diagnosis lesions affecting the tongue, to reach the ultimate solution.
Different Conditions Include
|
Infections |
Malignancies |
Blood dyscrasias |
Neurological evaluation |
|
Ulcerative Candidiasis Bacterial infections Fungal infections Tuberculosis Primary syphilis |
Lymphoma sarcoma |
Agranulocytosis (blood condition in which there are no white blood cells) |
Riga Fede disease can be an early sign of a neurological or developmental problem. |
It is important to note that histopathological features alone cannot be used to diagnose Riga-Fede syndrome. Clinical presentation and history are critical components in making a diagnosis. A thorough examination, including a medical and dental history, is essential to rule out other potential causes of oral ulcers and lesions. In summary, the histopathology of Riga-Fede syndrome is characterized by ulcerated and inflamed tissue with mixed acute and chronic inflammation, with possible signs of bacterial infection. However, further studies are needed to better understand the histopathological features of this rare condition.
Discussion
Riga-Fede syndrome or disease (RFD) is a reactive traumatic mucosal disease that is characterised by recurrent oral mucosal ulcerations. The mandibular incisor teeth's repeated stress to the tongue during constant protrusive and retrusive movements causes it to grow. Although the symptoms can be seen right away after birth with natal and neonatal teeth, the ailment is most frequently seen in infants, and the start of the lesions typically coincides with the eruption of the primary teeth.
It is described as traumatic ulcerative granuloma with stromal eosinophilia (TUGSE) that appears in early life. Elzay proposed that TUGSE and Riga Fede illness might be regarded as a single entity because they share similar histologic characteristics and are frequently linked to a history of trauma. Riga Fede disease is nearly entirely limited to the tongue, whereas TUGSE has primarily been known to arise in late adulthood and is not restricted in location to the tongue but can also appear in the buccal mucosa, vestibule, gingiva, or palate. In the current review of the literature, 29 lesions were identified as ulcerations on the ventral surface of the tongue as a result of repeated trauma to the primary lower incisors, three lesions were identified on the dorsal surface of the tongue as a result of trauma to the upper incisors, and three lesions were identified on the lower lip. Seven patients experienced the symptoms within two months of delivery. These instances were all connected to (neo)natal teeth. The remaining 27 individuals, with a mean age of ten months and ages ranging from six to twenty-four months, began to experience lesions after the eruption of their lower incisors. The ratio of men to women seemed to be 1.8:1 [3].
Although the cause of the early eruption of these teeth is unknown, a number of conditions, including infections, nutritional deficiencies, fever, endocrine disorders, tooth germs in a superficial position, and osteoblastic activity in the vicinity of dental germs, have been linked to the condition. Furthermore, In Grave's disease, elevated maternal anti-TSH receptor antibody levels could lead to fetal hyperthyroidism and that could explain the premature dental eruption, it could also occur because of the exposure of mother to environmental toxins like polychlorinated biphenyls (PCB). More than 20 syndromes and abnormalities, including chondroectodermal dysplasia, congenital pachyonychia, Hallermann-Streiff Syndrome, craniofacial dysostosis, Pierre Robin Sequence, Sotos Syndrome, Syndrome of Wiedemann, and Meckel and Gruber Syndrome, may be linked to heredity and the natal and neonatal teeth. In addition to the trauma brought on by the teeth, Narang et al. listed the persistent traction created by tongue-tie as additional factor. Certain authors associate RFD exclusively with the neurological disease cerebral palsy. This is reflected in the classification by Domingo- Cruz et al who divided the disease into precocious and late. Precocious RFD occurs in the 0-6 months age and has no relation to any neurological diseases. Late RFD occurs post 6 months with the primary teeth as the causative factor and related to neurologic diseases as these patients have difficulty controlling their tongue movement/voluntary movements.
The majority of natal teeth are deciduous teeth that emerged prematurely, while some may be supernumeraries. It is more common in females than males, with an incidence of 1:2000 live births. The existence of natal and neonatal teeth may result in difficulties such as discomfort in breastfeeding, aspiration of teeth, breast nipple bruises, lingual ulcerations, and unwillingness to eat. According to Tang et al., trauma is simply one of several factors that contribute to the development of RFD. Viral and toxic substances may enter the traumatised area through the submucosa and cause an inflammatory reaction and tissue loss.Every mucosal surface in the oral mucosa can be impacted, although in cases that have been recorded, the tongue is the most frequently afflicted area. Ulcerations on the tongue's ventral surface's midline are the typical visual representation of oral lesions [4].
Histopathologically, Riga Fede disease is distinguished by an ulcerated mucosa with granulation tissue and a mixed inflammatory infiltration made up of lymphocytes, macrophages, mast cells, and a profusion of eosinophils the latter of which is the most typical of this entity. There are multiple treatment plans discovered as solution for riga-fede disease, all of which significantly focus onto terminate the source of trauma so healing can take place. The first and foremost option opted as a treatment plan for riga-fede disease has always been a conservative approach and if this initial remedy does not provide a full- fledged resolution, then extraction of the neonatal tooth is the treatment of choice. To begin with, a conventional conservative treatment relies on multiple aspects, which are to be considered such as inconveniences during breast feeding, interference during suckling, implantation and the degree of mobility, occurrence of traumatic lesions. Out of all the most significant point to be notified is that if whether the tooth belongs to the natural dentition or if it’s a supernumerary tooth, with the aid of radiographic findings. If it is diagnosed as a tooth of natural dentition, each of the above-mentioned treatment strategies are ought to be considered, unless any of this would cause injury to the new born.
Conservative treatment: these management options can be utilized alone or in combination.
• Firmly implanted – can be left in the arch instead of extraction, except when they interfere while feeding or are extremely mobile with a substantial risk of aspiration, lastly if it holds to be responsible for the occurrence traumatic lesions on the tongue of the new born.
• To prevent injury to the maternal breast while feeding, the incisal pointed edges can be smoothened, or masking the ragged incisal edges with composite resins, opting to different methods of feeding habits such as shifting to physiological nursing bottles with large holes in the nipple, placing a nasogastric tube.
• cellulose film or other protective dental appliance; oral disinfectant; corticosteroids; teething ring
If conservative treatment strategy fails to accurately resolve the condition or when the child is gravely malnourished or dehydrated then extraction is the treatment of choice to be essentially considered. Alternatively, excision of the lesion itself might be performed. An excisional biopsy is indicated if the injury persists even after the extraction of the natal teeth. In the case described, the lesion healed in fifteen days, requiring no biopsy. After one year the infant had the upper incisors and right side lower central incisor partially erupting. At the radiographic examination it was found that the permanent central incisors were with 1/3 of the mineralized crown. The close follow-up of the successor permanent tooth eruption is very important. Since destruction of the primary or natural teeth may subsequently jeopardize the relationship between the jaws and child can develop harmful tongue posture, subsequently routing to speech problems. Consequently, resulting in difficulties for the eruption of the permanent teeth [5]. Table1gives a summary of the literature regarding Riga-Fede disease.
|
Authors Name |
Age |
Gender |
Tooth |
Presentation |
Treatment |
|
Dr M Khaja Khalid Nawaz et al (6) |
1 week(tooth present no lesion ) 3 weeks (lesion observed) |
Female |
natal tooth |
Ulceration on the ventral surface of the tongue, smooth reddish and replicates the tooth form. |
Extraction of the tooth was opted as the treatment of choice |
|
Mebin George Matthew (7) |
20 days |
Male set of twins |
Natal mobile tooth in the mandibular anterior region |
Circular Ulcer (1*1cm in one twin and 2*2 cm in other)on the ventral surface of the tongue |
Extraction of the tooth |
|
Luiz Evaristo Ricci Volpato et al (8) |
1 month |
Female |
2 Natal teeth in the mandibular anterior region |
Ulcerative lesion(8mm in diameter) on the ventral surface of the tongue |
Left natal tooth extracted Right natal tooth covered with an increment of GIC |
|
R.P.S. Mohan et al (9) Case 1 |
`30 days |
Male |
Natal left and right mandibular cental incisor |
15*10mm on the internal mucosa of the lower lip |
Selective grinding of the affected tooth with triamcinolone |
|
R.P.S. Mohan et al (9) Case 2 |
42 days |
Male |
Natal left and right mandibular central incisors |
25*25mm on the ventral surface of the tongue |
Extraction and triamcinolone |
|
R.P.S. Mohan et al (9) Case 3 |
34 months |
Male |
Natal left mandibular central incisor |
20*15 mm on the ventral surface of the tongue |
Selective grinding of the affected tooth with triamcinolone |
|
R.P.S. Mohan et al (9) Case 4 |
15 months |
Male |
Natal right mandibular incisor |
10*5mm on the ventral surface of the tongue |
Selective grinding of the affected tooth with triamcinolone. |
|
R.P.S. Mohan et al Case 5 |
20 months |
Male |
Natal left mandibular central incisor and right central and lateral incisor |
8*5mm on the ventral surface of the tongue |
Selective grinding of the affected tooth with triamcinolone. |
|
R.P.S. Mohan et al (9) Case 6 |
30 months |
Male |
Natal left mandibular lateral incisor |
2*3mm on the lateral left border of the tongue |
Extraction and triamcinolone application. |
|
R.P.S. Mohan et al (9) Case 7 |
46 months |
Male |
Natal right and left mandibular central incisor |
3*5mm on the right lateral border of the tongue |
Selective grinding of the affected tooth with triamcinolone. |
|
R.P.S. Mohan et al (9) Case 8 |
34 months |
Male |
Natal right mandibualr central incisor |
2*5mm at the tip of the tongue and the granulomatous tissue at the alveolar ridge |
Selective grinding of the affected tooth with triamcinolone. |
|
R.P.S. Mohan et al (9) Case 9 |
50 months |
Male |
Natal right and left mandibular central incisors |
15*10mm at the ventral surface of the tongue |
Selective grinding of the affected tooth with triamcinolone. |
Table1. Summary of the literature regarding Riga-Fede disease:
Conclusion
Early detection of Riga Fede disease is recommended since such lesions may produce deformity or mutilation of tongue, dehydration, inadequate nutrients intake by the infant and growth retardation. Furthermore, these teeth are generally present in syndromic children and it is important to rule out this during diagnosis. The treatment in these cases often requires an interdisciplinary approach of paediatrician and maxillofacial surgeon as it is concerned with the child’s health and future dentition. Extraction of the teeth may prove to be a good and viable treatment option in such cases since it can alleviate feeding. In case of mild to moderate irritation of the tongue, conservative treatment such as smoothing the incisal edge with an abrasive instrument is advocated. Alternatively a small increment of composite may be bonded to the incisal edge. In the present case, we performed extraction of the natal teeth and this offered improvement and normalization of feeding. In conclusion, as Riga Fede disease often mimics many oral malignant and benign disorders, the differential diagnosis is important [6-9].
List of Abbreviations
RFD: Riga-Fede syndrome or disease
Declarations
Ethics Approval and Consent to Participate
The article does not contain any studies with human participants or animals performed by any of the authors
Consent for Publication
The parent of the infant gave consent for publication of this case report and accompanying images.
Availability of Data and Materials
Not applicable
Competing Interests
All the authors declare the absence of a competing interests related to this study.
Funding
No funding obtained
Acknowledgements
Not applicable
References
- Rao, R. S., & Mathad, S. V. (2009). Natal teeth: Case report and review of literature. Journal of oral and maxillofacial pathology: JOMFP, 13(1), 41.
- Ceyhan, A. M., Yildirim, M., Basak, P. Y., Akkaya, V. B., & Ayata, A. (2009). Traumatic lingual ulcer in a child: Riga–Fede disease. Clinical and experimental dermatology, 34(2), 186-188.
- Çavus,S,, & Özmen, B. (2017). Riga-F ede disease in the upper jaw in an infant. Dermatologic Therapy, 30(5), e12517.
- Kumari, A., & Singh, P. K. (2019). Diagnosis of Riga–Fede Disease. The Indian Journal of Pediatrics, 86(2), 191-191.
- Costacurta, M., Maturo, P., & Docimo, R. (2012). Riga- Fede disease and neonatal teeth. Oral & implantology, 5(1), 26-30.
- Nawaz, M., Krishnamurthy, S., Sivaraman, G. S., & SivakumarS, N. N. (2016). Riga Fede Disease-A Case Report. JMSCR, 4(6), 11089-11091.
- Mathew, M. G. (2022). Riga Fede disease in twins. BMJ Case Reports, 15(11), e252226.
- Volpato, L. E. R., Simões, C. A. D., Simões, F., Nespolo, P. A., & Borges, Á. H. (2015). Riga-Fede Disease associated with natal teeth: two different approaches in the same case. Case reports in dentistry, 2015.
- Mohan, R. S., Verma, S., Gill, N., & Singh, U. (2014). Riga- Fede disease (Cardarelli's aphthae): A report of nine cases. South African Journal of Child Health, 8(2), 72-74.