
Archives of Case Reports: Open Access(ACROA)
ISSN: 3065-7598 | DOI: 10.33140/ACROA


Research Article - (2024) Volume 1, Issue 1
Revisioning Healthcare in a Different Key
Received Date: May 30, 2024 / Accepted Date: Jul 02, 2024 / Published Date: Jul 10, 2024
Copyright: ©Â©2024 Julian Ungar-Sargon. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Ungar-Sargon, J. (2024). Revisioning Healthcare in a Different Key. Arch of case Rep: Open, 1(1), 01-07.
Abstract
The doctor is effective only when he himself is affected. Only the ‘wounded physician’ heals. But when the doctor wears his personality like a coat of armour, he has no effect. (Jung [1961] 1963:134) [1].
Preamble
After decades working in the field of chronic degenerative neu-rological disorders I turned my attention to interventional pain management strategies in an effort to become more effective as a healer. I discovered that the same intangible issues were behind the symptoms of acute pain disorders as were chronic and that the hu¬man dimension of pain and suffering and the human experience of disease was as much a factor in the diagnostic and healing process of chronic as much as acute processes. Nowhere more did I discov¬er these factors than in the chronic disorder known as PTSD. Here, in seeing my brothers-in-arms in the military as well as in civilian practice, the influence of past trauma, and the coping mechanisms learned or inherited, played as important a role in predicting out¬come as any intervention, physical or psychological.
Over the decades my approach to hard core neurological disease has evolved yet centered around listening to the patient, what the focus of his or her concern is, what bothers him more than others, and how does his or her experience of the disease affect the way they view themselves, the future and their decline. For instance, disorders such as Parkinson’s or Alzheimer’s strike fear and dread into the hearts of patients and their caregivers yet calling them by a different taxonomy often does not carry the same emotional nor social cultural stigma [2].
In listening to the patient and understanding their cultural, socioeconomic resources and spiritual heritage I am able to conjure an inner landscape where I might empathize better with what the patient is experiencing.
By appreciating the inner dimension of the human suffering and anguish I am become a better healer since I am able to tailor treat¬ment, taking into account the fear and anxieties that might oth¬erwise be overlooked when administering this or that therapeutic regime. If the patient is deadly afraid of side effects, for instance, I might be more sensitive to a lower dose of the drug regime because of my concern about compliance.
In listening to each patient closely like a “sacred text”, I must “in-terpret” and engage in hermeneutics the way I do when reading the subtext with such nuances as grammar, prosody, syntax, and liter¬ary constructs. My research into Midrash helped me understand the very history as presented to me, was a narrative, so I had to pay closer attention to the stylistics of speech as well as specifics of the verbal content. All this must be interpreted and mined for inconsistencies, gaps, emphasis, rhythm, repetitions etc the way I would read a sacred text and engage in hermeneutics.
This emphasis on listening and communication has its roots, of course, in medicine itself. Medicine has since developed many tools, instruments, technologies, measures, laboratory tests and methods. But the most basic of all its historical measures was al-ways language. For anything to happen between caregiver and pa¬tient, anything at all, there must be communication, each speaking to the other. And because doctor and patient often start from such different places, cultures and biases of speaking, healing becomes an act, or multiple acts, of translation.
The healing language of which I speak can be at times in tension with the medical language and assumptions that doctors and many other health-care professionals become fluent in, in the course of their training. The language of medicine, paradoxically, keeps the patient at a distance. Most patients never learn to speak the Latin jargon of medical terms, and typically find it very removed from their own experience, sometimes traumatically so we learn to speak of the patient’s body as an object to be known and dis¬sected and disciplined and fought, not as of them, belonging to them. But as comforting as it can be to feel that our illnesses have comprehensible, treatable, even mechanical causes, to have our in¬dividual suffering knowable and classifiable in this totalizing way can evoke for the sufferer, as the medical sociologist Arthur Frank argues in “The Wounded Storyteller: Body, Illness, Ethics,” a du¬ality of sensibility, a conflictual experience of the body as, simulta¬neously, an object to be known, and the subjectively felt collection of sensations which we alone experience as ourselves [3].
Today as never before, both the experience of illness and the ex-perience of treating affliction take place within social conventions and expectations and often within a complex series of relation¬ships. In their reliance on witch doctors, oracles, shamen, priests, as well as in the family-wide and community-wide experience of illness, our forebears well understood this, and the modern sci¬entific reductionism whereby severance of the simultaneous con¬nections of spiritual and social bonds to the body has resulted in alienation of the patient to his or her own inner self in the race to more and more precision.
This split in pain and illness is a recent development, another ar-tifact of the modern situation of the body within the biomedical model and the inattention to soul.
Intuitive Practice of Medicine
A 2002 study investigated real cases of physician intuition. Eigh¬teen family medicine doctors were interviewed about their intui¬tive decision-making processes with patients [2]. Their responses were sorted into three different types of intuitions: “gut feelings,” which triggered a sense of alarm that spurred them to take action “recognitions,” decisions made in the face of conflicting informa¬tion or a lack of evidence; and “insights,” occurring as a rapid flash of inspiration that connected the dots to a correct diagnosis when no symptom interpretation was obvious.
I am sure all three of these types play a role in analyzing patient’s complaints but there is another intangible dimension of the inter¬action. It is a spiritual connection whereby my ego has to get out of the way as I am listening intently. I become lost in their narrative, exploring their inner landscape engaged fully without even aware¬ness of myself.
This kind of self- nullification is the mirror image of what I was trained to do, which was to examine the patient as an object and provide an objective analysis of the symptoms and signs, looking for patterns that compare this case with the known reported cases in the medical literature for common threads allowing for a diag¬nosis to emerge.
My model is a project that somehow integrates this intuitive ho¬listic approach with conventional scientific objective analysis all the while making use of state of art techniques without sacrificing either, to in effect bridge the gap between the inner experiential and outer objective evidence based scientific analysis.
Wounded Healer
The key to interact with patients has been connecting my vulner¬ability, fears and anxieties with theirs in a mutual bond of trust. This opens channels deeper than the therapeutic encounter where vulnerability allows for sharing and an intangible sense of the sa¬cred presence of soul.
There are various studies researching the concept of the wounded healer, most notably that by British counselor and psychotherapist Alison Barr who studied the significance of psychological wounds on people who decide to train as counsellors or psychotherapists. Barr used a pluralistic approach to her research, with the quan¬titative data analyzed using descriptive and inferential statistics and the qualitative data analyzed using thematic analysis, with a grounded theory approach. An on-line questionnaire was conduct¬ed with 253 respondents. Pilot and verification studies were per¬formed, and opportunities for further research highlighted.
Barr’s results showed that 73.9% of counselors and psycho-therapists have experienced one or more wounding experienc¬es leading to career choice. She also noted the following:
• In relation to the significance of the event(s) on career choice, when merging the categories ‘probably chosen career regardless’ with ‘possibly chosen career regardless’, and ‘unlikely chosen ca-reer regardless’ with ‘not considered career otherwise’, there is a slight majority in relation to the former. There are no significant differences in relation to demographic factors.
• In relation to whether one or more psychologically wounding experiences led to the choice of a career as a therapist, there is a significant difference within designation, gender, grouping gender and ethnicity, and grouping gender and age. There are no signifi-cant differences within approach, ethnicity or age.
• The majority of the wounds were caused by events experienced directly by the respondents (65%) as opposed to indirectly or both. Within demographic factors, the causes of the wounding experi-ences leading to career choice are not statistically significant.
• The exact causes of the wounds vary enormously. The main cat¬egories are abuse, family life as a child, mental ill-health (own), social, family life as an adult, bereavement, mental ill-health (others), life-threatening, physical ill-health (others), physical ill-health (own) and other.
• There are many implications for the future of the therapeutic world, focusing mainly on supervision and training.
The largest prevalence study on lived experience within the mental health field by Victor et al. (2022), found that 82% of clinical psy¬chology, counselling psychology, and school psychology graduate students and faculty members in United States and Canada expe¬rienced mental health conditions at some points of their lives [3].
What is a Wounded Healer?
In Greek mythology, the centaur ‘Chiron’ was known as the ‘Wounded Healer’.Chiron was poisoned by one of Hercules’ arrows, but because he was not able to heal himself he suffered thereafter from an incurable wound. Based on the Greek myth of the centaur Chiron and popularized by the psychiatrist Carl Jung, the wounded healer is a paradoxical concept The mythical healer heals all others but is never fully able to heal their own person¬al wound [4]. This creates an interpersonal paradoxical dynamic where within the creation of wounds, healing can occur. As heal-ers, we are expected to be whole and to find and fix wounds in our patients. However, if we can embrace our own woundedness, we can find relatedness. We avoid suffering only at the greatest cost of distancing ourselves from life. To live fully, we may need to look deeply and respectfully at our own suffering and at the suffering of others. Jung, developed this phenomenon by stating that:
“a good half of every treatment that probes at all deeply consists in the doctor’s examining himself…it is his own hurt that gives a measure of his power to heal. This, and nothing else, is the mean-ing of the Greek myth of the wounded physician.”
Latterly, the term ‘Wounded Healer’ has expanded from Jung’s original concept to cover the study of any professional healer who has been psychologically wounded, including counsellors, psy¬chotherapists, doctors and nurses.
A radically fresh interpretation of how we can best serve oth¬ers from the bestselling author of The Return of the Prodigal Son, hailed as “one of the world’s greatest spiritual writers” by Christianity Today “In our own woundedness, we can become a source of life for others.” In this hope-filled and profoundly simple book, Henri Nouwen inspires devoted men and women who want to be of service in their church or community but who have found traditional outreach alienating and ineffective. Weaving keen cultural analysis with his psychological and reli¬gious insights, Nouwen presents a balanced and creative theol¬ogy of service that begins with the realization of fundamental woundedness in human nature.
According to Nouwen, ministers are called to identify the suffering in their own hearts and make that recognition the starting point of their service. Ministers must be willing to go beyond their professional, somewhat aloof roles and leave themselves open as fellow human beings with the same wounds and suffering as those they serve. In other words, we heal from our wounds.
S. Philip Nolte and Yolanda Dreyer write as follows:
THE WOUNDED HEALER Nouwen ([1972] 1979) presents his perspective on the wounded healer in his book, the wounded healer: Ministry in contemporary society, by using four narratives. Each narrative is used to show how pastors can, in a compassionate and authentic way, assist people on their life journey. To develop an appreciation for Nouwen’s perspective, I shall give a short descrip- tion of the arguments in his book. Nouwen ([1972] 1979:3-5) calls his first narrative the ‘predicament of nuclear man’. Nouwen uses this epithet to give expression to his conviction that the people of his time have lost their trust in technological progress because they have realised that the creative powers of the human race have the potential to destroy our planet [4].
Nouwen’s choice for the phrase ‘nuclear generation’ probably re-sults from the destructive consequences of nuclear power as it was illustrated by the bombings of Hiroshima and Nagasaki at the end of the Second World War. The nuclear race between the world’s super powers in the wake of these bombings has played a signif¬icant role in strengthening this distrust of positive progress. This generation can therefore also be called a post-nuclear generation which in itself is almost a cognition of the ability of the human race to destroy itself and the earth. The acknowledgement of this destructive ability gives rise to emotions of anxiety and despon¬dency.
This tendency to cause destruction manifests itself in our current postmodern world in phenomena such as air pollution, depletion of natural resources, inter alia fossil fuels, the endangerment and extinction of large numbers of animal, birds, fish and reptiles, the destruction of rain forests, threat to plant species, and the depletion of the ozone layer with the concomitant increase in earth tempera¬tures.
The negative impact of progress and development on the envi-ronment has been sustained for centuries by a variety of master narratives, especially the narrative that science will progressively improve people’s lives. Although science led to many positive de-velopments, such as combatting illness and poverty, the vast ar-ray of negative consequences cannot be denied. Nouwen ([1972] 1979:8−9) further describes this generation as one without histor-ical continuity, by which he means that those belonging to this generation do not have a connection with meaningful values from their past and have no hope for the future.
A typical feature of this type of society is what Nouwen calls a ‘fragmented ideology’ (Nouwen [1972] 1979:9−12). Because peo-ple are overwhelmed by a wide variety of disparate values, ideas, religious beliefs and lifestyles, they find it difficult to accept one thought system or belief as answer to their dilemmas. The era during which the Christian church could present a solution to hu-manity’s primary predicament (as interpreted and formulated by the church) with a single, comprehensive master narrative, is gone and the church is now continuously challenged by a pluralistic, fragmented society.
Wounded Pastors Facilitate Healing
It is important to realise that there is a relationship between an external healer’s therapy and the internal or intra-psychic healer of the wounded person. Healing takes place when the inner healer is activated and working together with the external healer in the healing process. In this process a relationship is created between doctor and patient, a relationship in which the phenomenon of transference/countertransference is activated, and forms part of a deep, unconscious psychological process.
Groesbeck (1975) formulates this phenomenon as follows: Because of his illness, the patient activates his ‘inner physician or healer’. This, however, is not integrated into consciousness, but is projected onto and constellated by the persona of the doctor. So, too, in the doctor, his inner wounded side, his own unresolved illnesses, psychic, somatic or both are activated by his contact with the sick person [4].
This opposite side of the archetypal image is projected onto the patient, rather than being contained within himself. If the rela¬tionship remains like this, no movement to a real cure occurs, though remedies, physical and psychological, are applied. Real cure can only take place if the patient gets in touch with and receives help from his ‘inner healer’. And this can only hap¬pen if projections of the healer’s persona are withdrawn. This presupposes that the physician-healer is in touch with his own wounded side. If the projection remains, both doctor and pa¬tient attempt, …. to ‘heal the split through power’. Each at¬tempts to manipulate the other to conform to stereotyped roles.
Groesbeck 1975:125
The idea of the wounded healer is one of the staples of shamanism, as Joan Halifax and Donald F. Sander and Steven H. Wong have shown: the training of shamans involves an "initiatory crisis" - a prolonged stage of deliberate physical illness and/or psychological crisis that the initiated has to undergo as part of the training pro¬cess [4].
Such afflictions and their eventual cure serve as evidence that the shaman-to-be was indeed chosen by the spirits. In the tradition¬al African Xhosa culture, becoming a healer is a process that in¬volves experiences of illness, physical injury and pain. One of the Xhosa rites of initiation is Thwasa, a state of illness. The person experiencing it will undergo ailment and pain of body and mind and be made to suffer stomach aches, nervousness, and severe ache in the back, as well as possible periods of unconsciousness.
During these attacks, this person might also become emotionally withdrawn and be troubled by dreams (see Wreford). Thwasa is crucial for becoming a healer. Illness is regarded in this case as the state through which communication from the person's ancestors occurs. In Xhosa culture, it is believed that a person is chosen to protect and heal people by becoming an igqira (healer), and his ability to enter a state of Thwasa is both a part of his training and an indication that the ancestors have preferred him. The process of Thwasa demonstrates how close this tradition is to the Western concept of the wounded healer: the interpretation of illness in Xho¬sa society is based on the rationale that it is from experiencing ill-ness that the person undergoing training will learn how to observe, diagnose and treat other people's illnesses.
The Talmud (in Hebrew "instruction, learning") is a record of rabbinic discussions pertaining to Jewish law, ethics, customs, and history. The Talmud has two components: the Mishnah (ca. 200 A.D.), the first written compendium of Judaism's Oral Law, and the Gemara (ca. 500 A.D.), a discussion of the Mishnah. The Talmud is a wide-ranging document that touches on a great many subjects. Traditionally, Talmudic statements can be classified into two broad categories: Halakhic and Aggadic statements. Halakhic statements are those which directly relate to questions of Jewish law and practice. Aggadic statements are those which are not legal, but exegetical, homiletic, ethical, or historical in nature offering creative interpretations sometimes in the shape of tales, anecdotes, and parables.
The Following Story is a Talmudic Aggadah
Rabbi Hiyya Bar-Abba fell ill and Rabbi Johanan went in to visit him. He said to him: Are your sufferings welcome to you? He replied: Neither they nor their reward. He said to him: Give me your hand. He gave him his hand and he raised him. Rabbi Johanan once fell ill and Rabbi Hanina went in to visit him. He said to him: Are your sufferings welcome to you? He replied: Neither they nor their reward. He said to him: Give me your hand. He gave him his hand and he raised him. Why could not Rabbi Johanan raise himself? – They replied: The prisoner cannot free himself from jail. Rabbi Eleazar fell ill and Rabbi Johanan went in to visit him. He noticed that he was lying in a dark room, and he bared his arm and light radiated from it.
Thereupon he noticed that Rabbi Eleazar was weeping, and he said to him: Why do you weep? Is it because you did not study enough Torah? Surely, we learnt: The one who sacrifices much and the one who sacrifices little have the same merit, provided that the heart is directed to heaven. Is it perhaps lack sustenance? Not everybody has the privilege to enjoy two tables.
Is it perhaps because of [the lack of] chil-dren? This is the bone of my tenth son! — He replied to him: I am weeping on account of this beauty that is going to rot in the earth. He said to him: On that account you surely have a rea-son to weep; and they both wept. In the meanwhile, he said to him: Are your sufferings welcome to you?-He replied: Neither they nor their reward. He said to him: Give me your hand, and he gave him his hand and he raised him.
Babylonian Talmud, Tractate Berachot 5b
• This miniature story is made of three vignettes. Four Jewish scholars are introduced to the reader.
• Rabbi Johanan appears in all three vignettes, twice as a healer, and once, in the second section, as one who "fell ill" himself.
• Rabbi Hiyya Bar-Abba is the first one to become sick and Rabbi Johanan treats him.
• Then it is Rabbi Hanina who cares for Rabbi Johanan, in exactly the same way Rabbi Johanan had treated the ill scholar in the first scene.
• In the last, longer vignette, Rabbi Johanan cares again for another patient-colleague, Rabbi Eleazar.
• This time, however, it follows the time when Rabbi Johanan him¬self had been sick and was rescued by a friend. He is the same man, but not exactly the same healer.
• Something about him has changed. Rabbi Hiyya "fell ill" (the Talmud Aramaic text uses a word that might be translated as both "fell ill" and "became very weak"). Rabbi Johanan paid him a visit.
• Once there, he does not waste time on small talk. His question to Rabbi Hiyya, "Are your sufferings welcome to you," may have more than one meaning. Can I help? Do you want me to help you?
And on the less conscious level: Do you want to be healed? Are you ready to be treated? Sometimes a sick person is either too de¬pressed to be healed or feels comfortable in the role of the sick. He might produce some secondary gain from his illness. Rabbi Johan¬an wants to be sure that Rabbi Hiyya is ready for therapy. Rabbi Hiyya answers: "Neither they nor their reward."
In other words, he says: I do not like my suffering. I do not want to stay in this condition. I do not even believe or wish for a reward in heaven. I am ready to be healed. Rabbi Johanan hears these words. He gives Rabbi Hiyya his hand and raises him. Where from? Does he raise him from his bed, or from the chasm of his depression?
We only know that the healing process is short and effective: the healer gives the patient his hand, there is a short but meaningful connection between them, and the patient becomes healthy. In the second section the same thing happens to Rabbi Johanan himself. The healer has become sick. We can speculate that Rabbi Hiyya's disease could be physically or psychologically infectious, which is another professional risk that the healer-therapist has to under¬take. The Talmud continues to repeat the same story: another Rab¬bi comes to visit and he asks Rabbi Johanan the same question and gets the same reply. Now it is Rabbi Hanina who gives Rabbi Johanan his hand and raises him from his illness.
However, the Talmud does not leave us with a neatly symmetrical story. The narrator stops to ask a question: "why could not Rabbi Johanan raise himself?"-in other words: if he was such a great healer, why could he not heal himself? And the narrator replies: "the prisoner cannot free himself from jail." This short state¬ment is important for the understanding of Rabbi Johanan's figure as a wounded healer.
The prisoner metaphor is simple but powerful: the keys to the cell are on the other side of the door. The prisoner cannot free himself. He needs the helping hand of someone outside of the self. He will never be able to release and free himself. Isolated "self-help" is impossible. The third section of the story is longer and different from the scheme presented in the two other vignettes.
Rabbi Johanan, healed from his own suffering, comes to visit an-other scholar, Rabbi Eleazar, who fell ill. He notices that the sick friend is lying in a dark room. Then he notices that Rabbi Eleazar is weeping. Rabbi Johanan's eyes and ears are now open and sen-sitive to the condition and suffering of the other. Rabbi Johanan starts asking Rabbi Eleazar (who is probably suffering from major depression) a series of questions. This therapeutic conversation might be described nowadays as "cognitive therapy."
He offers a series of explanations for Rabbi Eleazar's condition, and then answers each of his own rhetorical questions with a com¬forting suggestion. The first explanation he proposes for Rabbi Eleazar's condition is that he might have missed spiritual or ac¬ademic opportunities. He answers that the intention is important, not the actual degree of learning. Then he asks about the ill per¬son's economic status and answers that some people will not be wealthy in this world.
Eventually, Rabbi Johanan asks about the fact that the ill person is childless and proposes this as another explanation for his poor con¬dition. His next act is moving. He shows Rabbi Eleazar, who is in¬deed childless, the bone of his own tenth son. The healer shares his own terrible wound with the patient: Rabbi Johanan is a bereaved father, who had had ten children and lost them all. Rabbi Eleazar, triggered by the questions of Rabbi Johanan, finally replies: "I am weeping on account of this beauty that is going to rot in the earth.
" My suffering, he says, is existential. I look at your beauty, Rabbi Johanan, and I know that it is ephemeral, temporary and brief like everything else on earth. Rabbi Johanan agrees and identifies with this existential problem. Then the healer and the patient cry togeth¬er. Only after this short therapeutic intervention, valuable to care¬giver and patient alike, does Rabbi Johanan ask the question about the value of suffering for Rabbi Eleazar, gives him his miraculous hand, and raises him back to health.
Rabbi Johanan's experience of suffering and illness has certain¬ly affected his treatment style and enabled him to share his own experience and deep emotions with the patient. He has become a brother or companion to the patient rather than a paternalistic healer. Being now aware of his wounds, he is not only giving treat¬ment, but also getting help and insight. That makes him a sensitive, touching, Wounded Healer.
The wounded healer is an archetype that suggests that a healer’s own wounds can carry curative power for clients. This article re-views past research regarding the construct of the wounded heal-er. The unique benefits that a psychotherapist’s personal struggles might have on work with clients are explored, as well as the poten¬tial vulnerability of some wounded healers with respect to stability of recovery, difficulty managing countertransference, compassion fatigue, and/or professional impairment. The review also explores psychologists’ perceptions of and responses to wounded healers and examines factors relating to social stigma and self-stigma that may influence wounded healers’ comfort in disclosing their wounds.
Noga Zerubavel and Margaret O’Dougherty Wright have proposed that the relative absence of dialogue in the field regarding wound¬ed healers encourages secrecy and shame among the wounded, thereby preventing access to support and guidance and discourag¬ing timely intervention when needed [4]. We explore the complex¬ities of navigating disclosure of wounds, given the atmosphere of silence and stigma. We suggest that the mental health field move toward an approach of greater openness and support regarding the wounded healer and provide recommendations for cultivating the safety necessary to promote resilience and posttraumatic growth.
Recovery Trajectories
The uncertain stability of the wounded healer’s recovery. Recov¬ery is not necessarily linear or, when achieved, permanent, con¬tributing to the complexity of assessing a wounded healer’s recov¬ery status. While psychologists can assess the wounded healer’s history of functioning, there is, inevitably, uncertainty about the wounded healer’s future trajectory. They proposed four different types of future trajectories that might characterize therapists who have struggled with a significant wound:
1. a trajectory anticipating recovery over time.
2. a trajectory characterized by posttraumatic growth.
3. a relapse trajectory, anticipating fluctuations and setbacks; and
4. a chronic dysfunction trajectory anticipating continuous symp¬tom-related struggles
(see Figure1).
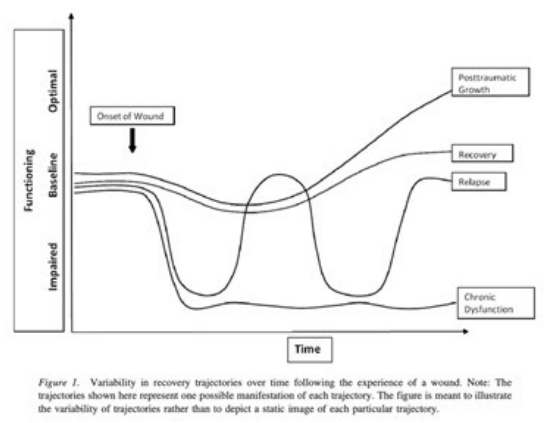
It should be noted that these four trajectories are presented to il¬lustrate the variability that is possible in recovery trajectories and are only some of the many trajectories of recovery that might oc¬cur. Because recovery processes are dynamic and include various trajectories, there is inherent uncertainty regarding an individual’s future psychological functioning.
Articulating this ambiguity helps to clarify the wariness and sus- picion that wounded healers often encounter professionally. The uncertainty regarding wounded healers’ future functioning pro-vides a framework for understanding the challenges faced by su-pervisors/consultants in responding to them. They suggested that professional wariness toward wounded healers is based on concern for relapse and regarding chronic dysfunction. The key issue for wounded healers, and for other professionals, is whether or not the manifestations of the wound interfere with or enhance their ability to provide effective and appropriate therapy. All the above applies to the field of psychological and psychosomatic therapies.
My experience however moves the model into the physical med-icine realm applying these techniques to treating even hard core neurological diseases such as Parkinsonism, MS and other neu¬ro-degenerative disease. More on that to follow [5-12].
References
- Jung, C.G. (1963) Memories, Dreams, Reflections. Edited by Jaffe, A., Ed. Translated by Winton, C. and Winton, R., Random House, 121-123.
- See The Body in Pain: The Making and Unmaking of the World by Elaine Scarry
- Frank A. (1995). The wounded storyteller: body, illness, and ethics. Chicago and London: University of Chicago Press.
- Greenhalgh, T. (2002). Intuition and evidence--uneasy bedfellows?. British Journal of General Practice, 52(478), 395-400.
- Zerubavel, N., & Wright, M. O. D. (2012). The dilemma of the wounded healer. Psychotherapy, 49(4), 482.
- Victor, S. E., Devendorf, A. R., Lewis, S. P., Rottenberg, J., & Muehlenkamp, J. J. et al. (2022). Only human: Mental-health difficulties among clinical, counseling, and school psychology faculty and trainees. Perspectives on Psychological Science, 17(6), 1576-1590.
- See, Groesbeck. (1975). The Wounded Healer. Journal of the Advanced Practitioner in Oncology, 8(5), 453-455.
- Nolte, S. P., & Dreyer, Y. (2010). The Paradox of being a Wounded healer: Henri JM Nouwen’s contribution to Pastoral Theology. HTS Teologiese Studies/Theological Studies, 66(2).
- Groesbeck, C. J. (1975). The archetypal image of the wounded healer. Journal of analytical psychology, 20(2), 122-145.
- Halifax, J. (1982). Shaman: The Wounded Healer. London: Thames and Hudson.
- Sander, Donald. F., & Steven, H. W. (1997). The Sacred Heritage: The Influence of Shamanism on Analytical Psychology. London: Routledge.
- Zerubavel, N., & Wright, M. O. D. (2012). The dilemma of the wounded healer. Psychotherapy, 49(4), 482-491.