
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Research Article - (2020) Volume 5, Issue 4
Reproductive Health Commodity Security Analysis and Planning System (RAPSYS): A Synergistic Study Model
Received Date: Sep 03, 2020 / Accepted Date: Oct 20, 2020 / Published Date: Oct 27, 2020
Copyright: ©Bongs Lainjo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Maternal and infant morbidity and mortality remain a global challenge and based on latest reports, mitigation efforts have not been encouraging. Unsustainable fertility rates continue to rise unabated in low and middle-income countries (LMICs). Reasons for these dismal performances include limited access to quality services, qualified staff, poor logistics management and lack of commodities. Reproductive Health Commodity Security Analysis and Planning System (RAPSYS) model is focused on mitigating these challenges. The participatory model is based on implemented results. It is defined by key themes. The systems use expert experience to develop effective strategies: qualitative assessment, Delphi ranking, action plan, commodity projection and monitoring framework. Evidence indicates that the conventional approach in program design and implementation continues to show different levels of understanding of the expected outcomes. This model has helped vulnerable countries in streamlining their interventions, making them more result-based, efficient, effective, sustainable and accountable. There is convincing evidence that the complications involved in designing development interventions have become more convoluted, unstructured, and poorly coordinated. This outlook has resulted in many cases producing inadequate and dismal outcomes. The relevant tasks are daunting. This framework – implemented in Asia - is part of an initiative to help refine current processes and procedures
Keywords
Reproductive-Health-Commodity-Security, Low-and-middle-income-countries, Synergistic-Framework, Maternal-In-fant-Morbidity, Family-Planning, Logistics-Management
Introduction
Contraception is a global issue affecting mostly women. In many countries, most women are cut off from education due to unplanned pregnancies before even completing a basic certificate. This results from a lack of education on contraceptives and a scarce supply. In this situation, Reproductive Health Commodity Security (RHCS) ensures contraceptives are available to all who need them. According to UNFPA (2010), ‘reproductive health commodity security means that all individuals can obtain and use affordable, quality reproductive health supplies of their choice whenever they need them’ (UNFPA 2010) [1].
RHCS ensures no customer is left out due to their locality, livelihood or social economic status. It requires that the right portion be supplied at the right time, place, condition, and price. It also ensures proper education is given to vulnerable parties before supplies are purchase and dispensed. Hence, each person in need chooses what suits their needs and comfort level and knows how to properly use the contraceptives to get maximum results.
Organizations like UNFPA, WHO and national and international funding agencies teaming up to support RHCS is a great encouragement and achievement. These institutions collectively contribute in promoting effectiveness to every person in need. They participate in ensuring that there is always a supply for those in need provided by qualified and motivated staff.
The national government also plays a major role in RHCS. Without its support, commodity security would not be where it is today, its shortcomings notwithstanding. For example, during the period of 1964 to 1973, where the landmark US Supreme Court case Griswold vs. Connecticut ended restrictions on the sale of contraceptives, the federal governments boosted the funding for family planning significantly. These changes advocated for the use of contraceptives and made an impact that is still felt today. As a result, more women were able to learn about the importance of family planning, leading to a more stable and informed generation of women.
From a human rights perspective, every country should embrace and support the use of contraceptives. Building facilities, creating awareness and providing the models at an affordable price to all is a sine qua non for the ultimate desired outcome, which is the ability for countries to achieve an increase in income. The population will be well sustained and more women will be able to achieve their educational goals. The mitigation of high infant and child mortality leads to an improved quality of life for both the mother and child. As families get planned parents and their children are able to improve their livelihood. In the long run very few people will be living below poverty line.
The importance of an effective monitoring and evaluation system operating in tandem with RHCS dynamics needs to be highlighted. Continuous collection, analysis, and reporting cannot be adequately emphasized.
In an article that appeared in one Centres for Disease Control report, over one-in-ten - nearly 37 per cent of all pregnancies in the USA are unintended [2]. In a report produced by UNFPA (2014), 225 million women around the world do not have access to contraceptives [3]. The commonality between both reports is the limited access to contraceptive by vulnerable communities and groups. There is every reason to believe that such a high level of discrepancy directly has a negative effect on both mothers and children. Such shortfalls also directly affect their quality of life in catastrophic ways. While MDGs did accomplish some of its targets, these indicators become significantly skewed when countries like India and China are included in the equation. Low and middle-income countries (LMICs) remain vulnerable and the urgent need to address these issues by making access to healthcare and commodities includes a human rights dimension. Africa, for example, (especially in sub-Sahara) has some of the most dismal health statistics including inadequate infrastructure, inconsistent access to and availability of commodities, limited trained staff and inadequate conditions of service among others. Additional key challenges that vary from country to country include: the high levels of anaemia and malnutrition among women (especially pregnant women); the continuing high unmet need of FP; low use of male participation in RH and FP; discontinuation of contraceptives; inadequate postnatal care. These are in addition to limited availability of services for the management of other RH care needs, including STI management, infertility management, Voluntary Counselling and Testing, reproductive organ cancers; and meeting the sexual and reproductive health needs of different vulnerable communities, especially unmarried adolescents.
These ubiquitous challenges are, for the most part, driven by two key factors-policy and culture. In the former case, RHCS is perceived as an attempt by donors and funding agencies to control national populations. And the effects of this mind-set have been so dominating that even in cases where policies do exist, very limited efforts are made by different governments to effectively implement them. For example, a significant amount of contraceptive commodity budgets is supported by funding agencies. They are forced to establish some degree of ‘policing’ in order to achieve meaningful results. To that effect, it is logical to conclude that the level of ownership by the nationals is not only inadequate but also dismal. In a cultural context, there are beliefs in some countries that having more children is not only an indication of ‘wealth’ but also a way to maintain generational continuity in a significant way. And every attempt to justify the rationale of having too many children is counter-balanced by the potential health risks faced by both the mother and baby.
According to available research findings, in order for any contraceptive security plan to work, there needs to be a market to enable utilization [4]. It is women in the market who will utilize the commodity of contraception being developed. Secondly, demand is also necessary [5]. This is because demand helps a company understand their target market and design a product specifically suited for them [6]. Access is also crucial since once the product is developed, it needs to be easily accessible to the members within the target market [7]. At this point, the marketing and distribution strategies used are critical [8]. This is also where supply comes into play since the company needs to supply enough of the product within the market and also ensure that it is not too much or too little [9].
Background
From a global perspective, the challenges presented earlier affect geopolitical communities in diverse and complicated ways. The implication is that in a given scenario, the potential and effective strategies in strengthening RHCS can vary from country to country. And this diversity and sophistication can even exist in the same region. One-size-fit all is an inappropriate approach that needs to be discouraged. While recognising these diversities, there is a need to also be conversant with existing commonalities. For example, ‘enabling environment’ will serve as a useful determinant in achieving sustainable RHCS but it differs amongst countries.
In order to convey some meaningful and compelling perspective, I have included some population-based graphs as an illustration of historical dynamics of FP-related indicators. These are countries from which participants were selected for a regional workshop whose study is presented in this paper.
Figures 1, 2, and 3 are demographic indicators of countries that participated in the regional RHCS training session conducted in Colombo, Sri Lanka.

Figure 1: Maternal Mortality Ratio. Source: UNFPA State of World Population (2004)

Figure 2: Contraceptive Prevalence Rate (Modern Methods). Source: UNFPA State of World Population (2004) & UNICEF State of World Children Report (2004)

Figure 3: Demographic Indicator: Total Fertility Rate. Source:
UNFPA State of the World Population Report (2004)
Rapsys: Highlights
The Reproductive Health Commodity Security Analysis and Planning System (RAPSYS) is a model designed to address some of the challenges identified in the previous paragraphs. It is a framework that if used effectively would contribute significantly in mitigating many of these weaknesses. Based on training sessions that have been conducted in Asia, the effectiveness of the model depends on the availability and motivation of experienced experts willing to work as a team in developing an action plan that is comprehensive, practical, cost effective and manageable. Because of the diverse nature of the team of experts, efforts are made to group them thematically in order to achieve high levels of concordance and mitigate discordances.
The model is conceptually defined (see figure 5) as a combination of unique and crosscutting determinants. The crosscutting components in this process involve coordination, supervision, funding, advocacy, as well as capacity building. All these factors provide for easy assessment of the performance of the product in meeting the needs of the clients as well as increases number of users (Contraception, 2015 250). These factors are all influenced by an enabling environment - from the physical health of the user to the market and the society in general [10]. The systems use expert experience to develop effective strategies including: qualitative assessment, Delphi ranking, action plan, commodity projection and monitoring framework [11].
The main objective of the model is to strengthen RHCS programming capacity. The methodology used would involve a panel of experts, a plenary, group work and a draft committee. In this paper, RHCS is defined as a contraceptive security that can continuously give commodities of high quality to a target and vulnerable group at the right place and when needed. These factors include an enabling environment, supply, procurement, use, access and demand, which are the bases of conceptual framework. The other highlights of the framework include its practical design, simplicity, participatory option, synergism it is synergetic, inclusiveness, and adaptability.
A more specific and comprehensive definition used in the paper includes the ability to continuously (enabling environment) provide (supply, procure) high quality commodities to the vulnerable group and target populations (use) at the right time and place (access) when needed (demand). RAPSYS characteristics include being practical, simple, participatory, synergistic, inclusive, multisector, adaptable and programmatic. The RAPSYS process (see Figure 4 and Figure 8) starts with determinant assessment (gaps) constituting of the input, followed by the development of strategies and activities constituting the process, and finalized with the development of Action Plan including an M & E system constituting the output.

Figure 4: RAPSYS Processes
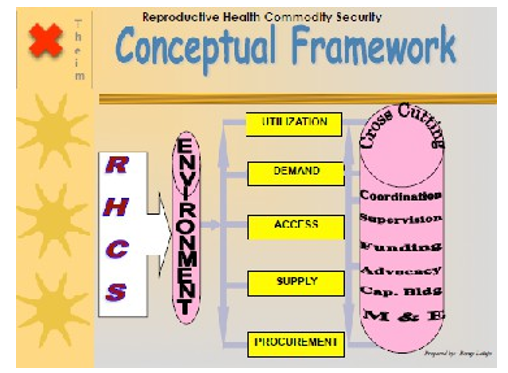
Figure 5: RAPSYS Conceptual Framework
The RAPSYS conceptual framework (see Figure 5) consists of the environment affecting the utilization, demand, access, supply and procurement, which then affects the cross cutting, coordination, supervision, funding advocacy, capacity building and M & E. The RAPSYS determinant matrix consists of access to public outlets, private outlets, social marketing outlets, bars, hotels, clubs, gas stations, toilets, bus/train station, and dispensers. The second determinant is the utilization, which consists of CPR, disease prevention, strengthened dual protection, promotion of female condoms. The third determinant is demand, which is composed vulnerable groups, current users, potential users (unmet needs), drop outs-family planning methods and unemployed and out of school youth. The fourth determinant is supply and is composed of distribution, transportation, storage/warehousing, LMIS, quality of care (QOC) and commodities. The fifth determinant is procurement composed of projection, costing/budgeting process, tendering process, ordering, shipment schedules, and quality assurance.
The first cross cutting determinant is environment consisting of political will, appropriate laws, and appropriate policies. The second crosscutting determinant is advocacy consisting of political leaders, religious leaders, community leaders, civil society, vulnerable groups and hard to reach communities and groups. The third crosscutting determinant is coordination consisting of government leadership, defining stakeholder roles (private, civil society, social marketing, public sector), dissemination forums, coordinating mechanisms, stakeholder meetings, and availability of coordinating committee. The fourth crosscutting determinant is funding consisting of stakeholders/partners, funding gaps, short, medium and long term funding strategy, exit strategy, sustainability strategy (phase in approach), and grants vs. loans.
The fifth cross cutting determinant is capacity building consisting of institutionalized (process vs. events), medium & long term plans, skills transfer, south-south collaboration, and target groups. The sixth cross cutting determinant is M and E consisting of institutionalized and systematic, clear and feasible objectives (CAFO), established achievable bench marks and timeframes, functional instruments, process approach with built in feedback mechanisms, and accountability/transparency. The seven cross cutting determinant is supervision consisting of supportive, availability of follow up plans, availability of feedback mechanisms, integrated instead of vertical, availability of guidelines and regular and consistent visits.
Table 1 classifies all the determinants and links them to their respective components.
Table 1: RAPSYS Determinant and Component Matrix
|
Determinant |
Component |
|
Access |
bus/train station
|
|
Utilization |
|
|
Demand |
|
|
Supply |
|
|
Procurement |
|
|
Crosscutting Determinants |
|
|
Environment |
|
|
Advocacy |
|
|
Coordination |
Marketing, Public sector)
|
|
Funding |
strategy
|
|
Capacity Building |
|
|
M and E |
timeframes
|
|
Supervision |
|
Rapsys: Thematic Description
Access Refers to the ease with which clients of RH services can access contraceptives and RH services when they need them. Such plac-es may be public outlets such as RH and Family Planning clinics or Non-Governmental Organizations (NGOs) community-based distribution programs. They may be private outlets such as phar-macies, department stores, groceries or kiosks selling cigarettes, juice, popular beverages, snacks and knickknacks. They may be places frequented for entertainment purposes, such as bars, hotels, or night clubs, or other places where items such as condoms may be available in dispensers such as bus depots, train stations, petrol stations, public toilets.
Access also means to point out the routes and degrees of ease or difficulty that people desiring and in need of RH services can fol-low to get information (advice, counselling) and services. It en-compasses a range of issues from regulatory practices governing the prescription and or sale of medical devices, hormonal forms of contraception and drugs that are used to treat RTIs/STIs, to convenience issues such as the places where contraceptives and antibiotic drugs are available, in both public and private sectors, and when people can purchase or obtain them and at what cost to the consumer depending on what he/she is able to afford. Access also extends to beliefs among providers as to what forms of con-traception are best for whom and, to some extent, the degree and severity of such infections that can be tolerated without resorting to medical attention, to belief systems among societies and family members regarding whether and if contraceptives should be used at all, and whether or not various severities of RTIs and STIs are, in fact, conditions that require medical attention.
Utilization
Means to measure the use of reproductive health services and com-modities. The use of contraception in family planning program is often measured through doing a Contraceptive Prevalence Survey (CPS) from which a Contraceptive Prevalence Rate among mar-ried couples is compiled. Other measurements are aimed to un-derstand utilization of male and female condoms in the prevention of sexually transmitted disease and HIV. Dual protection is a term applied to the use of condoms for both prevention of unwanted pregnancies and the prevention of sexually transmitted disease. RH Program approaches now often feature both the prevention of unwanted pregnancies and the prevention of disease transmission. Utilization also means a ratio that compares the supply of and de-mand for a particular good or service, or combination or goods and services whether the provision of the latter is dependent on the availability of the former.
Demand
Implies the level of interest that people express and the degree of effort they are willing to expend to acquire reproductive health advice, counselling and services and products such as contracep-tives and antibiotics for treating RTIs/STIs. In RAPSYS, this re-fers to the design, development or availability of communication messages, campaigns and strategies to create or increase demand. Demand creation is often targeted to specific vulnerable groups, such as sex workers or adolescents, whose access to and knowl- edge of RH is constrained by ignorance, social stigma and lack of empowerment. Demand is measured in terms of met and unmet indicators. Current Users of means of modern contraception is an example while unmet demand is measured through surveys that ask married women who are not using contraception whether they would rather be practicing some form of contraception. Demand is also viewed as ‘potential’ in that there may be social a group, such as unemployed men or out-of-school unmarried youth, who would like to or should be using RH services and family planning but are not. The popularity of RH services and different forms of con-traception is sometimes measured through tracking of dropouts, or women who cease using contraception for reasons other than wanting to become pregnant.
Supply
Means a process of the systematic distribution of goods and ser-vices, the former often through a chain of warehouses or store-rooms, to the latter which could be points of sale or service pro-vision (hospitals, clinics) in both the public and private sectors. The process of supplying involves transportation (frequency, cost, capacity), storing or warehousing of goods at intermediate and end points, managing and monitoring the process (LMIS) and under-standing that the process of supply adds value to commodities. The appropriate handling, storing and transporting of commodities has much to do with their condition when they are made available to intended end users. This is known as the Quality of Care ele-ment in the supply process. Capacity building efforts are most of-ten aimed at increased efficiency and skilled ability to effectively accomplish this function.
Procurement
Means the systematic acquisition of goods and services in cadence with demand and in cognizance of the supply ‘pipeline’ or the quantity of goods already purchased, entered into an inventory and either stored or in transit to points of sale and service provision. Procurement is a process requiring a high degree of knowledge and integrity as it involves a range of specialized skills. These in-clude (1) an ability to project or accurately forecast future needs; (2) an ability to accurately cost and budget for these needs on an annual basis; (3) a sound (fool proof) system for following ten-dering protocols related to the advertising for and evaluation of bids related to commodity requirements; (4) technical capacity to prepare/write legally binding and financially guaranteed contracts with suppliers and/or manufacturers who are awarded purchase or-ders, (5) technical capacity built on a sound LMIS to plan shipping schedules so that inventories do not grow dangerously excessive or that stock outs do not occur at the service delivery facilities and points of sale; (6) resources to closely monitor shipping sched-ules and movement of vessels and aircraft so that when goods pur-chased arrive at the port they are swiftly and safely disembarked, stored temporarily securely, promptly cleared through
custom formalities, and safely moved to central warehouse facili-ties and inventoried without delay; (7) and of inspecting manufac-tured items before shipping to ascertain that they meet standards stipulated in the purchase order and arranging and carrying out the inspection of all procured items upon arrival at destination to ensure that no damage was sustained during transit. The Quality Assurance process starts when decision to procure is made.
Environment
Often means the political will manifested by government and civil society to reduce excess or unwanted fertility, morbidity and mor-tality among a population perceived as being at risk. It implies a series of political, legal and financial commitments from those in positions of authority, which are very often influenced by groups who advocate for changes to archaic laws, policies and practices that are seen to dampen enthusiasm for or deny to those in need fulfilment of their reproductive rights and improved reproductive health status. In terms of RAPSYS, it includes the creation and en-actment of favourable laws and policies that facilitate implemen-tation of all determinants required to enable RHCS programming.
Advocacy
process of persuading an audience whether it be influential de-cision-makers, in the form of individuals, community and public opinion leaders, and/or public figures such as politicians, clergy, civic leaders or members of vulnerable populations, of the benefits of a changed status quo particularly when accumulated evidence demonstrates conclusively that the status quo is disadvantageous to one’s health and well-being and the health and well-being of the community and its constituents. In the context of RAPSYS, it means advocacy for the creation and enactment of favourable laws and policies that facilitate implementation of all determinants required to enable RHCS programming.
Coordination
Means a process of sharing information on strategies, plans and activities, results and outcomes and budgets and expenditures among stakeholders and partners usually in the context of a so-cial or civic endeavour such as in development. Stakeholders and partners are inclusive of donors, government agencies with vested interest, associations of business and commerce, non-governmen-tal organizations (NGOs) and the ‘intended beneficiaries’ who are often represented as special interest groupings such as women, young people, adolescents and men. The purpose of coordination is to ensure that conflicts of interest are avoided in the pursuit of common goals, that duplication of effort is minimized, and that resources are used to the best possible advantage to achieve the common goal and purposes of the endeavour or endeavours.
Funding
Means the resources, most commonly monetized in terms of hard and local currencies but also considered in terms of ‘in kind’ con-tributions, that stakeholders contribute, in terms of collective ef-fort, towards the achievement of strategic goals. Efforts are usually conceived as a series of deliberately planned and executed activi-ties, often structured as projects, timed in terms of short, medium and long perspectives or periods to achieve outputs that together will leverage the separate efforts to achieve the larger purpose and contribute significantly to realizing the strategic goal.
Capacity Building
A process of transferring knows how from highly skilled prac-titioners to those who are placed in charge of executing specific functions in order to achieve specific outputs on a routine and re- petitive basis. In terms of RAPSYS, capacity is seen as having been built sufficiently when designated employees of an institution or organization, working as a team, can continuously and routine-ly forecast, finance, procure and distribute all reproductive health services and products to the points of sale or service provision in such a way that the utilization ratio, that is the relationship be-tween supply and demand, is close to 1:1.
Monitoring and Evaluation
Monitoring is systematic and institutionalized process of observ-ing work in progress and noting when specified and scheduled in-dicators of progress, sometimes called milestones, are achieved or delayed and whether the overall progress is moving towards achieving an objective. In order to properly monitor, there must be clear and feasible outcomes or objectives (CAFO) and established, achievable benchmarks and timeframes. There must be an identi-fied and functional measurement system in place for good moni-toring to occur. There must be a process approach with a built-in feedback mechanism. And there must be accountability functions and transparency guarantees. Monitoring is, in fact, a deliberate effort to compile evidence that, when considered as a whole, pre-dicts the likelihood of a structured effort, such as a project, will be completed on time with the desired outcomes. It produces both a graphic and narrative ‘running’ commentary and offers managers and supervisors insight into delays and obstacles that impede effort as well as noting innovations that overcome unplanned or unex-pected events and unforeseen problems. In terms of RAPSYS, it may convey setting up milestones to monitor a procurement action, or series of procurement actions, and/or it may involve monitoring the supply system to determine whether the effort to maintain the left hand side of the supply/demand ratio at 1 or higher but not to exceed 2 is working.
Evaluation is an exercise to assess whether and to what degree the financial and material inputs and human effort achieved the stated outcome or objective in a systematic and institutionalized manner. It is one that requests an impartial observer, in effect a judge, to ascertain whether the outcome of an activity as described, say, in a log frame, was achieved as per schedule and within the budget, with commentary on the expenditure of resources and ef-fort, including skilled and unskilled labour and managerial effort. In terms of RAPSYS it means determining whether the, or any combination of the, 12 determinants was effective in raising the contraceptive prevalence rate and lowering the incidence of repro-ductive health morbidity.
Supervision
The process of exercising authority over the human and technical effort engaged in a planned and structured activity. The preferred method of exercise of authority is supportive. In this, the person in position of authority observes the work effort and points out when, where and how the worker, or the work force, can increase his/her/ its efficiency and productivity without increasing the risk to his/ her/its health, in both physical and mental terms. He/she would do this through direct observation as well as through established feed-back mechanisms so that communication between management and the workforce is integrated and two-way. He/she would ensure that guidelines related to worker safety, working conditions, and occupational hazards are in place, updated and reviewed with the work force on a periodic basis. He would also point out to manage-ment conditions detrimental to the health and safety of the work force and proffer concrete suggestions as to how to improve these.
In terms of RAPSYS, a supervisor might observe workers in a warehouse lifting and stacking cartons, noting the temperature and humidity of the warehouse, observing whether the worker is lifting by bending his knees, is seeking assistance from a fellow worker in the case of heavy cartons being stacked manually, is organizing the stacks properly by positioning the labels so as to be visible, is practicing First Expiry First Out (FEFO) in the arrangement of products, is using hydraulic lifting devices to stack at higher lev-els, and is wearing protective clothing, headgear and masks de-pending on the atmosphere in the warehouse. The supervisor will note the productivity of workers in terms of their physical health and safety, taking into account proper rest periods, intake of food and water, and the climate within which they are working, and then plan future work effort according to these measurements. He would make recommendations to management on how to improve the working environment overall so as to obtain the best human effort from the work crew and plan the monthly work output based on these expectations.
Figures 6 and 7 are pilot case studies that were conducted in Ban-gladesh and Sri Lanka: Two countries that participated in the Re-gional Workshop.

Figure 6: Panel Assessment – Bangladesh RHCS Level of Achievement
Panel Assessment: RHCS Level of Achievement-Bangladesh

Figure 7: Panel assessment – Sri Lanka RHCS Level of Achieve-mentScore: 1= insignificant, 2 = moderate, 3 = adequate, 4 = substan-tial, 5 = significant

Figure 8: RAPSYS Algorithm
Participants are divided into three or four groups (maximum of ten per group). Each group will identify a rapporteur and modera-tor and will be assigned 5-12 RHCS determinants for assessment. The rapporteurs will be responsible for compiling the group work according to the provided reporting format. The moderator will serve as a guide and limit discussions to the relevant issues and required outputs. Tables 2, 3, 4, and 5 were used in developing the final product. An illustrative and summarized workshop outcome of one of the participating countries is presented in Appendix A.
Establishing The Achievement Level
Methodology
The ‘quantitative assessment’ of the different determinants is based on the following simple calculation: For each Determinant Establish: Feasible Achievements (Gold Standard) MINUS Actual Achieve-ments EQUALS Potential Gap
Note: The bigger the potential gap, the lower the ‘achievement score’.
Group Work Guide
Table 2: RAPSYS: Qualitative Assessment Matrix (Qam)
|
Basic Determinant (1) |
Achievement Level Low=1 to High=5 (2) |
Gaps (3) |
Strategies (4) |
Remarks/ Observa-tions (5) |
|
1. Demand |
|
|
|
|
|
2. Supply |
|
|
|
|
|
3. Procurement |
|
|
|
|
|
4. Utilization |
|
|
|
|
|
5. Access |
|
|
|
|
|
Crosscutting Determinants |
||||
|
6. Enabling Environ-ment |
|
|
|
|
|
7.Coordination & |
|
|
|
|
|
Dissemination |
|
|
|
|
|
8. Supervision |
|
|
|
|
|
9. Funding |
|
|
|
|
|
10. Advocacy |
|
|
|
|
|
11. Capacity Building |
|
|
|
|
|
12. M and E |
|
|
|
|
Column Description
Column 1: List of all RHCS Determinants
Column 2: Scores, established by each group based on level of achievement (1= inadequate, 3 = adequate, 5 = significant level of achievement)
Column 3: List of potential Gaps
Column 4: Strategies to address gaps identified in column 3
Column 5: Additional remarks or comments:
Table 3: RAPSYS: RHCS Ranking Matrix
|
Basic Determinant (1) |
Rank (2) |
Remarks/Observations (3) |
|
Demand |
|
|
|
Supply |
|
|
|
Procurement |
|
|
|
Utilization |
|
|
|
Access |
|
|
|
Crosscutting Determinants |
||
|
Enabling Environment |
|
|
|
Coordination & Dissemination |
|
|
|
Supervision |
|
|
|
Funding |
|
|
|
Advocacy/BCC/IEC |
|
|
|
Capacity Building |
|
|
|
M and E |
|
|
|
Other (specify) |
|
|
Column Description
Column 1: List of all RHCS components
Column 2: Ranking based on level of importance of each deter-minant – 1 is most important - (note: more than 1 component can have the same rank)
Column 3: Additional information that may have significantly influenced the ranking
Table 4: RAPSYS: RHCS Action Plan (RAP)
|
Determinant (1) |
Identified Gaps (2) |
Strategy (3) |
Activities (4) |
Approximate Timing (5) |
Responsible Party (6) |
Approximate Cost (7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Column Description
Column 1: List of all RHCS Determinants
Column 2: Appropriate Gaps identified by each group for each determinant
Column 3: Required relevant strategy to address gaps identified in (2)
Column 4: Activities required to accomplish the strategy identi-fied in (3)
Column 5: Stakeholders responsible for implementing activities in (4)
Column 6: Approximate completion time of implementation
Column 7: Approximate cost of implementation
Table 5: RAPSYS: Monitoring and Evaluation Framework
|
Results(1) |
Strategy (2) |
Activities (3) |
Indicator (4) |
Baseline (Year) (5) |
Q1 (6) |
Q2 (7) |
Q3 (8) |
Q4 (9) |
Data Source (10) |
|
|
|
|
|
|
TA |
TA |
TA |
TA |
|
|
|
|
|
|
|
|
|
|
|
|
Column Description
Column 1: Gaps recorded with key words like improved, strength-ened, increased availability, increased accessibility etc.
Column 2: Strategy from action plan
Column 3: Activities from action plan
Column 4: Simple, feasible and measurable indicators
Column 5: First Year benchmark
Column 6 to 9: (T) Targets and (A) achievements for every quarter of a given year
Column 10: Source of data
Rapsys: Findings - Lessons Learned
For a workshop like this with participants from different countries, cultures and backgrounds, there is no doubt that the planning and implementation phases can be overwhelming. In order to mitigate some of these challenges, we developed in partnership with partic-ipating governments a set of criteria that was applied uniformly in each and every country. The list below highlights some of the post workshop analyses.
• Panel selection very critical
• Role and level of coordinator important
• Panel composition should be relevant to determinants
• Level of responsibility of panel members critical
• Minimum of two days required for meeting
• Initial group of panellist represents RHCS ad hoc committee
• Selection process of group moderator and rapporteurs critical
• Rapporteurs are responsible for first draft report
• Minimum of one month required for planning (logistics, mo-bilization)
• Media participation important
• Limit total number of participants to 25
• Leadership role of national government very important factor
• Panel members come from National & sub-national levels
• Participatory nature of meeting is a strong motivating factor.
• Strong level of ownership among participants also a motivat-ing factor
• Peer review session very important
• Selection of national counterpart critical
• Profile of panellists critical
Conclusion
There is compelling evidence that the complications involved in designing development interventions have become more convolut-ed, unstructured, and poorly coordinated producing in many cases inadequate and dismal outcomes. The relevant tasks are daunting with resources becoming more and more limited. This framework is part of an initiative to help refine current processes and pro-cedures. The euphoria, motivation and dynamism displayed in-cluding feedback received from the participating governments are indications of commitment and political will to make this model a reality. For example, countries like the Maldives and Sri Lanka with some of the most impressive action plans had no difficulty implementing the framework [12]. Appendix A Rapsys: Summary of Maldives Workshop Outcome Background Maldives has made significant progress in improving access to maternal health and family planning within the last few decades. For example, the country has substantially expanded delivery and access of care and has also improved antenatal coverage, skilled birth attendance, infertility treatment, and adolescent sexual and reproductive health (ASRH) services. The development and use of various national standards and guidelines have also been wit-nessed. All this has contributed to significant reductions in mater-nal mortality, infant mortality, and fertility. Since 1984, various family planning services have been offered in the country, includ-ing CoCs, progesterone only pills, injectable, IUD, Norplant, male condoms, and male and female sterilization – all sponsored by UNFPA. The National Reproductive Health Strategy was devel-oped in 2004 as part of efforts to streamline government policies concerning reproductive health. Ongoing UNFPA Assistance Under the UNFPA Country Programme III, the Department of Public Health and the Ministry are currently involved in imple-menting the RH Quality of Care Project from 2003-2007, which focuses on RHCS issues, particularly family planning. The project involves the development of Logistics Guidelines, and a National RH Strategy and procurement of all free contraceptives and RH commodities. The project focuses on five atolls in addition to the capital. Through the project, UNFPA and the Public Health De-partment procure free contraceptives and other RH commodities including drugs, consumables and the relevant equipment. The project facilitates training in RHCS according to the developed guidelines. The five atoll areas are strengthened, as they are the basic areas of focus. The project also emphasizes on advocacy that is meant to complement the ongoing work in the QoC project. The Thematic Trust Fund will greatly assist in reaching other atolls. Challenges Remaining Highlights of some outstanding challenges range from high un-met needs to dropouts to STI and infertility management to limited method mix and more. These services are to some extent available at the central level. However, to make further progress towards achieving the ICPD and MDG goals, these areas need further con-solidation within the nation RH programme and mainstreaming throughout the country. RHCS Assessment The RHCS assessment of the situation in the country revealed sig-nificant gaps in a number of areas, namely: demand, access, capac-ity building, advocacy, supervision, and procurement utilisation. Achievements are summarized in Figure 1 below.

Figure 1: RHCS Assessment
Scores: 1 = inadequate, 2 = moderate, 3 = adequate, 4 = substantial, 5 = significant
Demand
The gaps related to demand that were identified include overall low demand for contraceptives, limited targeting of specific de-mand creation initiatives for vulnerable groups, and poor outreach to dropouts and potential users.
Access
The gaps associated with access include limited access through private outlets, such as hotels and other outlets, weak technical capacity for condom promotion and marketing campaigns.
Capacity Building
The gaps identified under capacity building include limited local/ national capacity for training, limitations in funding, and lack of a comprehensive staff development plan; high turn-over, skill and work mismatch in filling positions, limited means for establishing systematic mechanism for regular refreshers.
Advocacy
Under advocacy, the key gaps identified include limited informa-tion dissemination on RH issues for political and religious leaders, undeveloped mechanisms for ongoing advocacy and lobbying to political and religious leaders for support of RH/FP.
Supervision
Gaps under supervision included insufficient systematic supervi-sion, benchmarks and targets not always utilised, limited feedback mechanism, underdeveloped standards/guidelines for supervision, checklist needs to cover supervision and logistics issues in super-vision such as high transportation costs.
Utilisation
Gaps related to utilisation included a high unmet need for contra-ceptives and limited awareness regarding STI prevention and dual protection.
Procurement
The gaps identified under procurement included limited capabili-ties in quality assurance, costing and budgeting to be undertaken by government and quality assurance deficiencies.
RHCS Action Plan
The country has made achievements in securing, stabilizing, and making the RHCS program sustainable and the UNFPA has played a significant role in assisting the program. The RH project has also gained commodities from the national budget line created by the government. Under the current RH program, an exit strategy has also been established. The government will have to gradually uti-lise the national budget line in the procurement of contraceptives and reduce reliance on the UNFPA to secure RHCS, which will serve as the exit strategy. The national strategy and the coordi-nating committee will oversee the implementation of the major strategies and activities in the RH program including those in the proposal. Based on the RHCS Assessment, the country proposal focuses on two basic determinants and three crosscutting determi-nants. In order of priority these are:
1. Demand
2. Access
3. Capacity Building
4. Advocacy
5. Supervision
6. Procurement
7. Utilisation
Demand
The proposed RHCS action plan and strategies include strength-ening awareness of and demand for RH/FP services amongst ad-olescents, educating young people on RH/FP including HIV/STI, building capacity of service providers for quality RH/FP services and promotion of services.
Access
To address the RHS gaps the main action plan involves strengthen- ing capacities for promotion of condom use using media and other means and building partnership with private sector to increase the availability of contraceptives.
Capacity Building
The planned strategies for addressing capacity building related gaps include strengthening capacity for training at the national lev-el, international training for the programme manager, logistics of-ficers and developing and implementing a staff development plan.
Advocacy
To reduce advocacy related gaps, planned actions include strength-ened dialogue between MoH and religious leaders and preparing and disseminating user-friendly information on RH/FP issues to political and religious leaders as well as building links and part-nerships with media for RH/FP advocacy.
Supervision
The plan to address supervision-related gaps includes developing national standards and guidelines, reforming management pro-cesses, and strengthening decentralisation.
Utilisation
The planned strategies for addressing utilisation RHCS gaps in-clude increasing awareness amongst young people on condom use for dual protection (FP and disease prevention), promoting FP information and services with special emphasis on IUD/male methods, and supporting local NGOs to participate in the RH/FP program.
Procurement
The RHCS action plan for addressing procurement gaps includes building national capacities and leadership for projections, cost and budget forecasting, liaising with MPND/MOH to develop long-term/medium-term forecasting and costing (activity) and strengthening national guidelines for contraceptive logistics.
Monitoring and Evaluation
The implementation of the strategies and the planned activities will be monitored by the RH coordinating committee, which was established under the RH strategy. Specifically, the monitoring of the activities will be performed by the Department of Public Health. The Department is already performing oversight roles in the Quality of Care project in the major areas of focus. Any other new initiated activity will thus be under the department for eval-uation of their progress. The findings will then be reported to the overall committee of the UNFPA on the QoC project. The regional hospitals will be designated the responsibility of day-to-day super-vision in strengthening its decentralization. A framework has been developed to monitor and evaluate the project. The framework is a qualitative assessment matrix containing the determinants, the level of achievements, and the possible gaps and strategies for the various measures. The core determinants are demand, access, capacity building, advocacy, supervision, utilization, and procure-ment
Total Budget Requirements
The budget is based on the costs of each determinant and totals US$ 156,050.
|
Basic Determinant |
Cost US$ |
|
Demand |
10500 |
|
Access |
50000 |
|
Capacity Building |
44000 |
|
Advocacy |
29350 |
|
Supervision |
13000 |
|
Utilisation |
2000 |
|
Procurement |
7200 |
References
- UNFPA (2010) The program to enhance reproductive health security 7.
- William D Mosher, Jo Jones, Joice C Abma (2012) Intended and Unintended Births in the Unites States: 1982-2010: Na-tional Health Statistics Report Number 55.
- UNFPA (2014) Guttmacher Institute, The Costs and Benefits of Investing in Reproductive Health 10.
- Belaid L, Dumont A, Chaillet N, De Brouwere V, Zertal A, et al. (2015) Protocol for a systematic review on the effect of demand generation interventions on uptake and use of modern contraceptives in LMIC. Systematic Reviews 4: 124.
- Rabbani F, Pradhan NA, Zaidi S, Azam SI, Yousuf F (2015) Service quality in contracted facilities. International Journal of Health Care Quality Assurance 28: 520-531.
- Stenberg K, Axelson H, Sheehan P, Anderson I, Gülmezoglu AM, et al. (2014) Advancing social and economic develop ment by investing in women’s and children’s health: a new Global Investment Framework. The Lancet 383: 1333-1354
- Cavallaro FL, Benova L, Macleod D, Faye A, Lynch CA (2017) Examining trends in family planning among harder to-reach women in Senegal 1992–2014. Scientific Reports 7.
- Rademacher KH, Vahdat HL, Dorflinger L, Owen DH, Stein er MJ (2014) Global introduction of a low-cost contraceptive implant. In Critical Issues in Reproductive Health. Springer Netherlands 285-306
- Grindlay K, Burns B, Grossman D (2013) Prescription re-quirements and over-the-counter access to oral contracep-tives: a global review. Contraception 88: 91-96.
- Nawaz Y, Maan AA, Mahmood B, Asif F (2013) Knowledge and Usage of Contraceptives, Influencing Male Reproductive Health Behavior. International Journal of Asian Social Sci-ence 3: 38-68.
- Alayande A, Mamman Daura F, Adedeji O, Muhammad AZ (2016) Midwives as drivers of reproductive health commodity security in Kaduna State, Nigeria. The European Journal of Contraception & Reproductive Health Care 21: 207-212.
- Belluck P (2016) Panel calls for depression screenings during and after pregnancy. The New York Times