
International Journal of Forensic Research(IJFR)
ISSN: 2767-2972 | DOI: 10.33140/IJFR
Impact Factor: 1.9

Research Article - (2025) Volume 6, Issue 1
Repeat Cholecystectomy. A Mummified Gallbladder was the Clue to Diagnose Duplicate Gallbladder: A Case Report and Review of Literature
2MBChB, faculty of medicine, Aswan university, Egypt
3Medical Research Platform, Egypt
4Faculty of Medicine, Delta University for Science and Technology, Dakahlia, Egypt
5Professor of general surgery, Department of General Surgery, faculty of medicine, Aswan university, Department of Maxillofacial Surgery, Faculty of Dentistry, Sphinx University, Egypt
Received Date: Mar 03, 2025 / Accepted Date: Apr 08, 2025 / Published Date: May 02, 2025
Copyright: ©©2025 Mohie El-Din Mostafa Madany, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Madany, M. E. D. M., Zakaria. A., Abdelaal. H. A., Ahmed. H., Bakr. A. M., et al. (2025). Repeat Cholecystectomy. A Mummified Gallbladder was the Clue to Diagnose Duplicate Gallbladder: A Case Report and Review of Literature. In J Fore Res, 6(1), 01-11.
Abstract
Background: Gallbladder duplication is a rare congenital anomaly and a rare cause of post cholecystectomy syndrome.
Methods: We reported a case of missed duplicate gallbladder and performed a review of literature on repeat cholecystectomy Additionally, a systematic review and meta-analysis was performed on the same topic. A database search was performed in PubMed followed by screening according to selection criteria which includes case reports that mentioned repeat cholecystectomy. We excluded all reviews, letters or abstract only articles. JBI critical appraisal tool was used to assess the quality of the included studies.
Results: A 34-year-old, male patient with a history of open cholecystectomy 2 years and 7 months ago, presented with recurrent episodes of severe right hypochondrial colicky pain radiating to the right shoulder. After appropriate history taking, physical examination, revision of the patient’s profile recorded in our database and lastly the mummified gall bladder kept with the patient’s mother, we decided to perform an abdominal ultrasound followed by MRCP to finally conclude intraoperatively that this is a case of duplicate gall bladder.
The systematic review included 20 articles after screening of 238 articles according to our selection criteria. The risk of bias was assessed in the included studies of which 18 studies got good score while only two got fair.
Conclusion: We conclude that we should include duplicate gall bladder as one of the causes of the post cholecystectomy syndrome. Moreover, it highlights that duplicate GB can be missed preoperatively, and operatively even with a senior experienced consultant.
Keywords
Case Report, Cholecystitis, Repeat Cholecystectomy, Duplicate Gallbladder
Introduction
Gallbladder (GB) duplication is a congenital anomaly that is considered rare being present in about one in 4000 births. The first report of duplication of the gallbladder is credited to Blasius in 1675. GB Duplication has many forms including the true duplication form being two completely separated gallbladders or Y-shaped in which the two gallbladders are united with a single cystic duct prior to joining the common hepatic duct. Gallbladder duplication is suggested to be the result of exuberant budding of the developing biliary tree during the division of the caudal bud of the hepatic diverticulum [1]. Additionally, it may be associated with duplication of cystic duct. Thus, the anatomy should be precisely visualized during surgery to avoid injuries to other structures [2,3].
Gallstone is the commonest complication associated with duplicate gallbladder. Although it usually affects one lobe, both can be involved with equal risk for the disease. Hence, resection of both gallbladders is the rule [3,4].
Ultrasonography (US) is a very popular imaging modality for the assessment of gallbladder diseases. Its primary benefit comes from evaluating the gallbladder wall and contents. However, it cannot assess the anatomy of the biliary tree, while magnetic resonance cholangiopancreatography (MRCP) can. Therefore, it is considered the investigation of choice to visualize the biliary anatomy even when complicated by certain diseases [1,5-7].
The identification of duplicate gallbladder before attempting to perform cholecystectomy is crucial to prevent or at least decrease the rate of complications. Moreover, the gallbladder duplication is diagnosed preoperatively in only fewer than half of the cases, which can be attributed to the presence of many variations. For instance, some of them were found to be more difficult to be detected when the duplicate organ is positioned remotely or deeper in the viscera, e.g. above the right or rarely the left hepatic artery [4]. Thus, appropriate diagnosis is essential to avoid recurrence of the symptoms, and repetition of the procedure, with a risk of special surgical complications mainly due to distorted biliary anatomy [1,5,8,9].
Methods
Case Report
We report a case of cholecystitis after open cholecystectomy in a private center, according to SCARE criteria [10].
Systematic Review
We performed a systematic review and meta-analysis according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. (Supplementary table 1). The literature review was performed in PubMed and SCOPUS in October 2022 using the following search term (((repeat cholecystectomy) OR (second cholecystectomy)) AND ((double gallbladder) OR (duplicate gallbladder) OR (gallbladder duplication) OR (multiple gallbladders))). Then, title and abstract screening followed by full-text screening was performed by two independent reviewers according to our selection criteria. We included all case reports that reported repeat cholecystectomy without any restrictions to language, age, or gender. Any reviews, letters, or abstract only articles were excluded. Afterwards, the data of the included articles were extracted using a standardized excel sheet by two independent reviewers. All conflicts were solved through discussion and the senior author was consulted to reach a consensus. The extracted data was analyzed qualitatively and summarized in tables. Risk of bias was performed using JBI (Joanna Briggs Institute) critical appraisal tool for case reports [11]. The quality of the studies was divided into good, fair, or poor according to the score. In detail, the quality was considered good if it scored (6-8). On the other hand, a poor quality was considered if the study got (0-2).
Results
Case Report
Patient Information
A 34-year-old male patient presented to our private center with recurrent episodes of severe right hypochondrium pain, radiating to the right shoulder, lasting for 20 to 40 minutes. Additionally, the patient complained from epigastric pain which suggested cholecystitis [12].
The patient was not diabetic or hypertensive and didn’t suffer from any chromic or acute comorbidities. He had a history of mini-laparotomy cholecystectomy, which was done by the same consultant; Dr. Madany MEDM 2 years and 7 months ago. Also, the patient reported administration of symptomatic treatment such as proton pump inhibitor for epigastric pain.
On examination the patient was vitally stable, and the scare of the previous operation was observed through inspection. On palpation, there was mild tenderness in the right hypochondrium and epigastric region. The laboratory results including CBC, Bilirubin, AST, and ALT were within the normal range. An US report, which was performed before visiting our center, revealed the presence of non-calcular cholecystitis. Reviewing his records revealed that the previous cholecystectomy passed without any complications. Moreover, his mother had brought the specimen of the removed GB in the same piece of gauze she received! (Figure 1). On gross examination, it was complete GB, measured 4x2 cm2, with clearly ligated cystic duct with Vicryl suture. Abdominal US was repeated and revealed GB-like structure containing small stones in the GB fossa, followed by MRCP to confirm the diagnosis. Our proposed differential diagnoses were 1) Dilated cystic duct containing stones, 2) GB remnant, 3) Duplication of GB, and 4) Choledochal cyst.
Medical treatment was started immediately, and the patient was followed up monthly. There was no detected improvement in the symptoms for 20 months till the patient agreed to laparoscopic intervention. Intra-operative diagnosis of duplicate GB was established, and laparoscopic cholecystectomy of the 2nd gall bladder was performed after extensive meticulous adhesiolysis especially in the presence of a caterpillar hump of the right hepatic artery (Figure 3).
Surgical Technique
Under general anesthesia a classic laparoscopic cholecystectomy was performed. We inserted a 5 mm port in the upper margin of the umbilicus for the 5 mm 30° scope. During exploration, there was a minimal adhesion to the right of the falciform ligament. The sub-xiphoid and the subcostal midclavicular line 5 mm ports were inserted.
Thereafter, we found an accessory Riedel’s lobe in the liver situated to the left of the gallbladder fossa, where extensive adhesions of the previous surgery were found. Thus, a meticulous adhesiolysis was performed until we surprisingly found a missed gallbladder. Finally, we inserted a fourth 5 mm port in the lateral subcostal port.
We caught the fundus of the gallbladder and used it for retraction. Then, we continued meticulous adhesiolysis using monopolar diathermy and hydro dissection until we reached the Calot triangle, where a caterpillar hump of the right hepatic artery was found (Figure 3). Using 2/0 vicryl, we performed two sutures to ligate the cystic duct, then we divided the cystic duct.
The previous gallbladder had a clear print on the liver bed, we carefully continued the dissection of the gallbladder from its surrounding adhesions with concerns to the caterpillar hump. We found the second gallbladder situated to the left of the previous gallbladder and above the caterpillar hump.
We removed the second gallbladder and explored the hilum of the liver where we found a tubular structure which was assumed to be the cystic duct of the previously excised gallbladder. Therefore, we can describe that both cystic ducts were situated distal to the caterpillar hump of the right hepatic artery. Finally, we retrieved the gallbladder through the 5 mm lateral subcostal port.
After the laparoscopic cholecystectomy, the patient had a smooth post-operative period without any complications.
Histopathology
Histopathologic examination of both gallbladders; the mummified and the recent one confirmed the diagnosis of duplicate gallbladder.
Gross Picture
1. The 1st gall bladder: A mummified gall bladder measured 4x2 cm, with dark outer surface and intraluminal stone mud.
2. The recently removed cholecystectomy specimen: Gall bladder measured 3x2 cm, with smooth outer surface, greenish velvety mucosa and average wall thickness 0.3 cm. Lumen was distended with bile.
Microscopic Picture
1. Sections examined from the 1st gall bladder revealed dense fibrosis and hyalinosis of the wall without definite mucosal lining and with remnants of stone.
2. Sections examined from the recent gall bladder:
a. Revealed partially ulcerated mucosa.
b. The wall was infiltrated by lymph-plasma cells and showed fibrosis.
There was no evidence of malignancy in the received specimens.
Histopathologic Diagnosis
The histopathologic report concluded a gall bladder duplication (congenital anomaly), with chronic cholecystitis in both of them, with no malignancy.
Systematic Review
The database search revealed 238 articles of which only 20 articles were eligible according to our selection criteria. (Figure 1)
The demographic and characteristics of included studies were summarized in Table 1. The age ranged from 20 to 75 years. There were 12 female and 9 male cases, and a case was undefined.
Laparoscopic cholecystectomy was performed to remove the first gall bladder in 15 cases of whom only one converted to open surgery. While 6 patients undergone open cholecystectomy and only one case performed Laparoscopic Endoscopic Cooperative Surgery (LEC). On the other hand, the number of patients undergone open cholecystectomy for the 2nd operation was 11, while 9 patients undergone laparoscopic cholecystectomy. The remaining two patients had either LEC or unreported. The time between the 1st and the 2nd operation ranged from 5 days to 40 years. The rate of shifting from open in the 1st operation to laparoscopic in the 2nd operation was 2 of 22 cases, and the rate of shifting form laparoscopic to open was 7 of 22 cases.
Although, the type of 1st operation was laparoscopic cholecystectomy in 15 cases, we suggest that the type of operation isn’t the cause of the repeat cholecystectomy, as the 1st case reported in the literature was Deans & Brough, 1994, which was after the beginning laparoscopic era, so the surgeons started to rely on laparoscopic more than open in cholecystectomy [13]. Moreover, the availability of some investigations like MRCP and ERCP facilitate the diagnosis of missed GB in addition to the development of new generations of ultrasonographic devices with a better resolutions and efficacy. Also, laparoscopic assessment encourages surgeons to evaluate these patients more than open surgery.
The radiological investigations available for the diagnosis of missed gallbladder after cholecystectomy were US, X-ray, CT, MRI, ERCP, MRCP, intraoperative cholangiogram, HIDA scan, barium follow through and CT cholangiogram. The most used investigation was US in 21 cases, MRCP in 8 cases, ERCP in 7 cases and CT in 7 cases. The proposed differential diagnoses (DD) for these cases were as follow: 1) a remnant infundibulum from subtotal cholecystectomy, 2) a pseudocyst of the common bile duct, 3) a choledochal cyst, 4) a recurrent internal hernia with postoperative changes on imaging, 5) a duplicate gall-bladder, 6) acute pancreatitis, 7) bile duct diverticulum, 8) free fluid or abscess formation, 9) gallbladder diverticulum, 10) focal adenomyomatosis, 11) Phrygian cap, 12) walled off collection as a result of granulomatous reaction to dropped gallstones, 13) bilobed or duplex gallbladder with one half having been removed at previous surgery, 14) incomplete cholecystectomy or a collection in the gallbladder bed, and 15) remnant GB. The risk of bias was assessed in the included articles which yielded a good score in 18 studies, fair score in two studies and no article got bad score. The detailed assessment is shown in supplementary table 1.

Figure 1: Prisma Flow Diagram Showing the Search Results and Screening Process of Included Articles

Figure 2: The Specimen of the Removed GB in the Same Piece of Gauze she Received 2 Years and 7 Months Ago in A Mummified State!
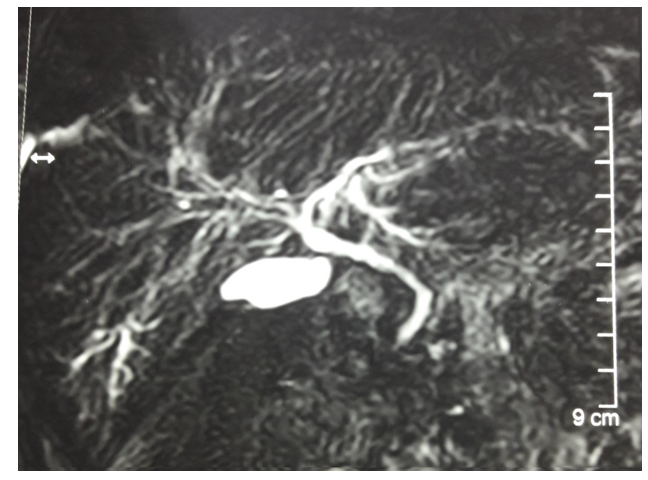
Figure 3: MRCP Showing the Biliary Tree and Structure Like Gall Bladder

Figure 4: Laparoscopic Image Showing 1) Caterpillar Artery and 2) Cystic Duct
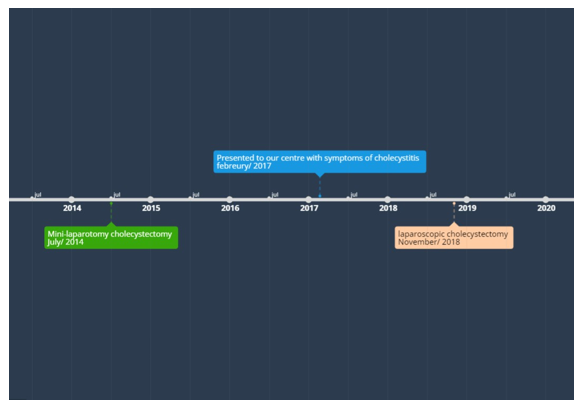
Figure 5: Timeline of the Case Events
Discussion
Gallbladder duplication is one of the rarest congenital anomalies of the hepatobiliary system accounting for 1:4000 births. However, this ratio reports only symptomatic cases and cases discovered incidentally during surgery, imaging modalities and autopsy. Hence, the true incidence of this anomaly is not precisely known. In addition, the usual initial preoperative imaging modalities used in cases of cholelithiasis, and cholecystitis often miss the detection leading to increased risk of intraoperative iatrogenic complications. Incidental detection of double gall bladder during surgery requires intraoperative cholangiography with meticulous delineation of biliary tree [8,14-17].
According to Desolneux et al., the incidence of gall bladder disorders is the same in both single and duplicated gall bladder.
Meanwhile, Pillay study reported that the inadequate bile drainage, which is usually present in this anomaly, increases the risk of cholelithiasis [18,19].
Asymptomatic gallbladder duplication does not require surgical intervention. However, when surgery is decided, removal of both is crucial once become symptomatic [20].
In our case, when patient presented to us 4 years ago, the diagnosis of duplicate gallbladder was missed preoperatively with ultrasound and intraoperatively during open surgery which could be justified by that this duplicate gall bladder was type II and it was remote and deeply situated in viscera above the right hepatic artery. Also, the mini-laparotomy approach may be a factor. The second time the patient presented to our clinic with similar complaint of biliary colic and after appropriate history taking, physical examination, revision of patient’s profile recorded in our database and lastly the mummified gall bladder kept with the patient’s mother, we decided to perform an abdominal ultrasound followed by MRCP to finally conclude intraoperatively that this is a case of duplicate gallbladder [1,5,8].
The operative data in the reported cases was limited, so we can’t identify a risk factor for missing a gall bladder e.g., the use of an angled lens (30 degrees) or Zero-degree lens.
According to our knowledge, this is the 1st article to report duplicate GB removal by the same surgeon, the 1st was mini laparotomy, and the 2nd was lap. Chole in addition to the presence of the old and the new GB at time of pathological examination. Also, the presence of an isolated mummified GB that belongs to a living person for 4 years and 3 months, is reported in literature for the first time.
Conclusion
This study suggests including duplicate gallbladder as one of the causes of post cholecystectomy syndrome. Moreover, it highlights that duplicate GB can be missed preoperatively, and operatively even with a senior experienced consultant. Preoperative ultrasound can often miss the diagnosis of gallbladder duplication. Additionally, the lack of performing a careful and meticulous dissection of biliary system will likely lead to missing the diagnosis. MRCP is the investigation of choice for proper identification of the anatomy of the biliary system.
|
Author ID |
Age & gender |
Clinical picture of the repeated chole- cystitis |
Interval between the 2 operations |
Radiology |
Suggested differ- ential diagnosis |
site of 2nd gall bladder |
|
(Deans & Brough, 1994) [13] |
65 yrs. â?? patient |
Recurrent abdominal pain |
Lap. Chole. And they didn't report if re-operated or not |
US and ERCP |
NR |
NR |
|
23 yrs. â?? patient |
Recurrent abdominal pain |
Lap. Chole. then Roux- en-Y hepatico-jejunostomy (Bluhmgart type) performed after 3 months |
US and ERCP |
NR |
NR |
|
|
(Cohen et al., 1995) [21] |
42 yrs. â?? patient |
Acute onset of epigastric pain and vomiting |
Lap. Chole. then Open Chole. after 7 months |
X-ray, US and ERCP |
NR |
NR |
|
(De Leeuw et al., 1995) [16] |
46 yrs. â?? patient |
NR |
Lap. Chole. then Cholecys- tectomy (didn't report the op. type) after 6 months |
US, CT and ERCP |
NR |
NR |
|
45 yrs. â?? patient |
Continuous RUQ pain. |
Lap. Chole. then open after 6 months |
ERCP |
NR |
NR |
|
|
(Heinerman et al., 1995) [22] |
36 yrs. â?? patient |
RUQ pain for one day Clinical examination revealed tenderness in the RUQ. |
Lap. Chole. then Open Chole. after 5 days |
US and ERCP |
NR |
NR |
|
(Silvis, 1996) [23] |
56 yrs. â?? patient |
Pain in epigastric region radiation to shoulder, without fever for a year |
Lap. Chole. then Open Chole. after 12 months |
US, ERCP and CT |
NR |
NR |
|
(Gigot et al., 1997) [3] |
29 yrs. â?? patient |
RUQ pain for 5 months |
Selective Lap. accessory Chole then Lap. Chole. after 5 months |
US and Oral chole- cystography |
NR |
the accessory gall- bladder was located inferiorly to the main one |
|
(Shapiro & Rennie, 1999) [24] |
42 yrs. â?? patient |
Bilious vomiting, and characteristic non-ra- diating pain. On examination dif- fuse Tenderness with guarding in the RUQ. A +ve Murphy’s sign. |
Open Chole. then Open Chole. after 2 years X-ray, US, and intraoperative chol- angiogram |
X-ray, US, and intraoperative cholangiogram |
|
The second gall- bladder was located deep in the liver bed. |
|
(Leenhouts et al., 2004) [25] |
48 yrs. â?? patient |
Colic attacks in the URQ with nausea and vomiting for one year On physical exam- ination, there was pressure pain in the RUQ. |
Open Chole. then Re-explo- ration with Open Chole. after 1 year |
US and MRCP |
NR |
NR |
|
69 yrs. â?? patient |
Pain in shoulders |
Open Chole. then Open Chole. after 40 years |
US and MRCP |
NR |
NR |
|
|
(Strupas & Simutis, 2004) [26] |
30 yrs. patient |
Colicky pain in the LUQ, nausea and bloating for 3 years |
Lap. Endoscopic Co-opera- tive Surgery (LEC) then LEC after 3 years |
US, CT, ERCP and MRI |
NR |
NR |
|
(Singh et al., 2006) [27] |
63 yrs. â?? patient |
Progressive jaundice for one months |
Lap. Chole. then Open Chole. after 1 year |
US and CT |
NR |
the gallbladder with a cystic duct that drained towards the rt. hepatic duct |
|
(Borghi et al., 2008) [15] |
72 yrs. â?? patient |
History of Abdominal pain and vomiting for 5 hours |
Lap. Chole. then Lap. Chole. after 8 days |
X-ray, CT, US and ERCP |
1- acute pancreatitis |
It with its own cys- tic duct and cystic artery was con- firmed posterolater- ally in the pedicle |
|
(Lefemine & Lazim, 2009) [28] |
55 yrs. â?? patient |
The patient complaint from recurrent attacks of persistent, sharp pain in the RUQ, peri-umbilical and epigastric region, very rarely radiated to the back. The pain was exacerbated by movement. |
Lap. Chole. then Lap. Chole. after 1 year |
US, barium follow through, HIDA, MRCP and CT cholangiogram |
incomplete cho- lecystectomy or a collection in the gallbladder bed |
it was wrapped in omentum and laying on the transverse colon |
|
(Reinisch et al., 2009) [29] |
73 yrs. â?? patient |
Colic-like RUQ pain, jaundice, and elevated cholestasis parameters |
Open Chole. then Lap. Chole. after 17 years |
US and ERCP |
NR |
NR |
|
(Fitchett et al., 2011) [30] |
75 yrs. â?? patient |
RUQ pain for 5 months |
Lap. Chole. then Exploration & Lap Chole after 6 months |
US, MRCP and HIDA (A hepatobi- liary iminodiacetic acid scan) |
|
NR |
|
(Mulholland et al., 2012) [31] |
20 yrs. â?? patient |
Severe episodic epi- gastric pain, related to food |
Lap. Chole. then Lap. Chole. after 4 years |
US and MRCP |
NR |
The gallbladder was identified and noted to be largely intra- hepatic and difficult to dissect from the liver bed. |
|
(Rangarajan et al., 2017) [32] |
46 yrs. â?? patient |
RUQ pain and dys- pepsia |
Open Chole. then Lap. Chole. after 2 y |
|
remnant bladder -gall bladder dupli- cation |
NR |
|
(Kowalchuk et al., 2018) [33] |
49 yrs. â?? patient |
NR |
Lap. Chole. converted to open then Open Chole. after 48 days |
US, CT, MRCP and intraoperative cholangiogram |
NR |
A gallbladder with a long tortuous cystic duct was identified posterior to the co- lon and duodenum, inferomedial to the inferior tip of the right lobe of the liv- er, and anterolateral to the right kidney MRI with MRCP demonstrated that it located within the retroperitoneal space posterior to the colon. It was lateral to the duodenum at its lower portion and posterior to the duodenum super- omedially near the CBD |
|
(Pera et al., 2019) [34] |
45 yrs. â?? patient |
History of Rt upper quadrant pain ↑meals with associated nausea and occasional abdominal distention for 30 days on examination there were tenderness to palpation in the right upper and lower quadrants |
Lap. Chole. then Lap. Chole. after 3 years. |
CT and MRCP |
changes on imaging 5- a duplicate gall- bladder |
The gallbladder was situated directly above the right hepatic artery, from which arose the cystic artery sup- plying the duplicate gallbladder. |
|
(Fetti et al., 2020) [35] |
47 yrs. â?? patient |
History of recurrent URQ abdominal pain, nausea, vomiting, and bloating started 24 hours ago after a fatty meal. Physical examination revealed abdominal surgical scars, tender- ness without guarding or Murphy’s sign |
Lap. Chole. then Lap. Chole. after 9 years |
US and MRCP |
1-choledochal cyst 2- bile duct diver- ticulum |
A short cystic duct between the saccular structure and the main bile duct and a cystic artery were found |
|
(Hailu et al., 2021) [36] |
39 yrs. â?? patient |
RUQ colicky pain for 2 weeks |
Open Chole. then Open Chole. after 6 months |
X-ray and US |
NR |
NR |
|
(Wang, 2022) [37] |
63 yrs. â?? patient |
Intermittent both RT& LT upper abdominal pain, 30 to 60 minutes after meals, and significant flatulence and bloat- ing and intermittent loose stools for 16 years |
Lap. Chole. then Lap. Chole. after 16 years |
US, MRCP and intraoperative cholangiogram |
4-Phrygian cap, |
Though the visual- ized gallbladder was small with a deep intrahepatic lie |
Table 1: Baseline Characteristics of Similar Case Reports
References
- Boyden, E. A. (1926). The accessory gall? Bladder? An embryological and comparative study of aberrant biliary vesicles occurring in man and the domestic mammals. American Journal of Anatomy, 38(2), 177-231.
- Kothari, P. R., Kumar, T., Jiwane, A., Paul, S., Kutumbale, R., & Kulkarni, B. (2005). Unusual features of gall bladder duplication cyst with review of the literature. Pediatric surgery international, 21, 552-554.
- Gigot, J. F., Van Beers, B., Goncette, L., Etienne, J., Collard, A., Jadoul, P., ... & Kestens, P. J. (1997). Laparoscopic treatment of gallbladder duplication: a plea for removal of both gallbladders. Surgical endoscopy, 11, 479-482.
- Horattas, M. C. (1998). Gallbladder duplication and laparoscopic management. Journal of Laparoendoscopic & Advanced Surgical Techniques, 8(4), 231-235.
- Goh, Y. M., Goh, Y. L., Ewan, L. C., Turner, P. D., Lapsia, S., & Subar, D. A. (2015). A case report of duplex gallbladder and review of the literature. International journal of surgery case reports, 14, 179-181.
- Mazziotti, S., Minutoli, F., Blandino, A., Vinci, S., Salamone, I., & Gaeta, M. (2001). Gallbladder duplication: MR cholangiography demonstration. Abdominal imaging, 26, 287-289.
- Vasanthraj, P. K., Ramachandran, R., Athiyappan, K., Chandrasekharan, A., & Narayanan, C. D. (2014). Imaging in double gall bladder with acute cholecystitis—a rare entity. Surgical Science, 5(7), 273-279.
- Hishinuma, M., Isogai, Y., Matsuura, Y., Kodaira, M., Oi, S., Ichikawa, N., ... & Kuriki, K. (2004). Double gallbladder. Journal of gastroenterology and hepatology, 19(2), 233-235.
- Udelsman, R., & Sugarbaker, P. H. (1985). Congenital duplication of the gallbladder associated with an anomalous right hepatic artery. The American journal of surgery, 149(6), 812-815.
- Agha, R. A., Borrelli, M. R., Farwana, R., Koshy, K., Fowler,J., Orgill, D. P., ... & Kasi, V. (2018). The SCARE 2018statement: updating consensus Surgical CAse REport (SCARE) guidelines. International Journal of Surgery, 60, 132-136.
- Porritt, K., Gomersall, J., & Lockwood, C. (2014). JBI's systematic reviews: study selection and critical appraisal. AJN The American Journal of Nursing, 114(6), 47-52.
- Knab, L. M., Boller, A. M., & Mahvi, D. M. (2014).
- Deans, G. T., & Brough, W. A. (1994). ‘Persistent gall- bladder’after laparoscopic cholecystectomy. Minimally Invasive Therapy, 3(4), 215-216.
- Urbain, D., Jeanmart, J., Janne, P., Lemone, M., Platteborse, R., De Reuck, M., & Deltenre, M. (1989). Double gallbladder with transientcholestasis:preoperativedemonstrationbyendoscopic retrograde cholangiopancreatography. Gastrointestinal endoscopy, 35(4), 346-348.
- Borghi, F., Giraudo, G., Geretto, P., & Ghezzo, L. (2008). Perforation of missed double gallbladder after primary laparoscopic cholecystectomy: endoscopic and laparoscopic management. Journal of Laparoendoscopic & Advanced Surgical Techniques, 18(3), 429-431.
- De Leeuw, T. G., Verbeek, P. C. M., Rauws, E. A. J., & Gouma,D. J. (1995). Adouble or bilobar gallbladder as a cause of severe complications after (laparoscopic) cholecystectomy. Surgical endoscopy, 9, 998-1000.
- Cummiskey, R. D., & Champagne, L. P. (1997). Duplicate gallbladder during laparoscopic cholecystectomy. Surgical Laparoscopy Endoscopy & Percutaneous Techniques, 7(3), 268-270.
- Desolneux, G., Mucci, S., Lebigot, J., Arnaud, J. P., & Hamy,J. G. R. (2009). Duplication of the gallbladder. A case report. Gastroenterology research and practice, 2009(1), 483473.
- Pillay, Y. (2015). Gallbladder duplication. International journal of surgery case reports, 11, 18-20.
- Shiba, H., Misawa, T., Ito, R., Ohki, K., Igarashi, T., & Yanaga, K. (2014). Duplicated gallbladder. International Surgery, 99(1), 77-78.
- Cohen, S. A., Attiyeh, F. F., Kasmin, F. E., & Siegel, J. H. (1995). Persistence of the gallbladder following laparoscopic cholecystectomy: a case report. Endoscopy, 27(04), 334-336.
- Heinerman, M., Lexer, G., Sungler, P., Mayer, F., & Boeckl, O. (1995). Endoscopic retrograde cholangiographic demonstration of a double gallbladder following laparoscopic cholecystectomy. Surgical endoscopy, 9, 61-62.
- Silvis, R. V. W. A., Van Wieringen, A. J. M., & Van der Werken, C. H. R. (1996). Reoperation for a symptomatic double gallbladder. Surgical endoscopy, 10, 336-337.
- Shapiro, T., & Rennie, W. (1999). Duplicate gallbladder cholecystitis after open cholecystectomy. Annals of emergency medicine, 33(5), 584-587.
- Leenhouts, P. A., Zeebregts, C. J., Plaisier, P. W., &Gerritsen, J. J. (2004). Symptoms of cholelithiasis following cholecystectomy; possibly a second gallbladder. Nederlands tijdschrift voor geneeskunde, 148(4), 190-193.
- Strupas, K., & Simutis, G. (2004). Treatment of double gallbladder: A case report and review of the literature. CHIRURGISCHE GASTROENTEROLOGIE, 20(2), 157-160.
- Singh, B., Ramsaroop, L., Allopi, L., Moodley, J., & Satyapal, K. S. (2006). Duplicate gallbladder: an unusual case report. Surgical and Radiologic Anatomy, 28, 654-657.
- Lefemine, V., & Lazim, T. R. (2009). Neuroma of a doublegallbladder: a case report. Cases Journal, 2, 1-5.
- Reinisch, A., Brandt, L., & Fuchs, K. H. (2009). Doppelt angelegte Gallenblase–Laparoskopische Cholezystektomie 17 Jahre nach konventioneller Cholezystektomie. Zentralblatt für Chirurgie, 134(06), 576-579.
- Fitchett, J. M., l Davies, L., & Kumar, N. (2011). Gallstone pancreatitis after laparoscopic cholecystectomy. Case Reports, 2011, bcr0820114673.
- Mulholland, D., McEntee, G., McCormack, O., & Geoghegan,T. W. (2012). Double trouble-duplication of the gall bladder requiring repeat laparoscopic cholecystectomy.
- Rangarajan, K., Chinna, S., Nair, N., & Das, C. J. (2017).Peril of missing a double gall bladder: report of a patient who needed cholecystectomy two times over. Case Reports, 2017, bcr2016218248.
- Kowalchuk, R. O., Kowalchuk, R. M., Kaplan-List, K., Oates,T. K., & Smith, S. C. (2018). Symptomatic cholelithiasis in an ectopic retrocolic retroduodenal subhepatic duplicated gallbladder. Radiology Case Reports, 13(4), 904-908.
- Pera, S. J., Huh, N., & Orcutt, S. T. (2019). Duplicate gallbladder: a case report of a patient with cholecystitis after cholecystectomy. International Journal of Surgery Case Reports, 65, 156-160.
- Fetti, A. C., Necula, A., Puia, V. R., Zaharie, F., Puia, A., & Al Hajjar, N. (2020). Laparoscopic cholecystectomy for overlooked duplicated gallbladder. A case report and review of the literature. Annali Italiani di Chirurgia, 9, S2239253X20034350-S2239253X20034350.
- Hailu, S., Gebremariam, M., Girma, T., & Regasa, T. (2021). Re-operation for symptomatic cholelithiasis with a double gallbladder: A rare case report in a limited imaging setup. International Journal of Surgery Open, 36, 100416.
- Wang, T. N., Shriki, J. E., & Marquardt, D. L. (2022). Repeat laparoscopic cholecystectomy for duplicated gallbladder after 16-year interval. Federal Practitioner, 39(2), e1.