
International Journal of Women's Health Care(IJWHC)
ISSN: 2573-9506 | DOI: 10.33140/IJWHC
Impact Factor: 1.011


Review Article - (2017) Volume 2, Issue 2
Remember the Ladies: Gender Equity for Corporate Compliance Programs Using Nanotechnology
Received Date: Sep 27, 2017 / Accepted Date: Oct 27, 2017 / Published Date: Nov 05, 2017
Copyright: ©Ilise L Feitshans. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
First Lady Abigail Adams was the wife of the second United States (U.S.) President and the mother of another U.S. President; she successfully ran a farm while her husband was away writing the Declaration of Independence.
Introduction
Rethinking An Old Problem: The Dilemma of Women’s Occupational Health
First Lady Abigail Adams was the wife of the second United States (U.S.) President and the mother of another U.S. President; she successfully ran a farm while her husband was away writing the Declaration of Independence.
Her famous letters to her husband urged him to “Remember the Ladies” when declaring independent suffrage for humans who lacked the divine right of kings, and also described the hard work of managing a family business while raising and educating several children while combatting illness. Abigail Adams wrote a letter to her husband, John Adams, 95 days before Mr. Adams signed the Declaration of Independence “in the new code of laws which I suppose it will be necessary for you to make, I desire you would remember the ladies and be more generous and favourable to them than your ancestors”. Gender equity in the workplace is therefore an old problem, and a problem that has garnered significant attention in recent decades.
Unfortunately, current international and U.S. workplace policies still reflect many of the dilemmas that were confronted by Mrs. Adams at the birth of the U.S. in 1776 [1].
According to the World Health Organization (WHO), women are less likely than men to receive employer-provided health and safety training, or to be re-trained during modernization activities and corporate restructuring. Women are also less likely than their male counterparts to benefit from workplace prevention and intervention measures, since they are not well-represented in management. Women often lack the authority to make an impact on their working conditions. WHO also notes that “when women do experience a work-related health problem; they are less likely than men to be diagnosed, recognized, compensated or be offered rehabilitation” [2]. Consequently, there are many unanswered questions about how to implement safety and health protections fairly for all people. The big question is: How can safety professionals proactively implement gender equity within the context of occupational health and safety compliance programs so that legal mandates are obeyed, so that once gender equity has been achieved, it is a win/win for all?
This article examines several unresolved issues. Despite success stories and great strides in gender equity around the world, many industrial hygiene and occupational health concerns have yet to be resolved regarding the role of women in the workplace. Issues of concern in occupational health and safety include: whether there is or ought to be a separate agenda for women’s health protections at work, elements of reproductive health at work that may impact men and women differently, and the resulting health disparities that may arise from inadequate protections within the scope of gender equity. There are also gaps in occupational epidemiology when considering the effect of gender. “Lack of consideration of sex and gender differences” in work exposures and hazards. A lack of analysis or measurement of domestic work hazards, part-time or flexible work arrangements, long working hours, and the lack of studies on gender segregation in work environments has also contributed to the paucity of information about gender inequalities in occupational health [3]. Questions surrounding how to implement effective occupational safety and health compliance programs offering fair protection for women workers ultimately impact the policies that should protect all humans at work.
In addition to providing yet another incentive for effective programming in the workplace, attention to these issues will have major societal benefits for reducing infant mortality and protecting the health of men who are dependent upon the wages of the women in their family. The work of implementing the goals of gender equity as protected under law has only just begun and readers are encouraged to work towards these goals to make their implementation a reality.
A. The Industrial Hygiene Context for Gender Equity
International law and the law of every nation require that employers bear responsibility for workplace health hazards, regardless whether they impact only men or only women. Just like discrimination laws, occupational health and safety laws are universally available in every country and in many treaties.
Sound compliance programs are the grease of the machinery of commerce, not the fat to be trimmed in times of economic austerity. Even employers in the public sector use compliance programs as a tool for obeying the law and providing evidence of compliance. The philosophy that work-related illnesses are an avoidable aspect of industrialization is a fundamental tenet of all occupational safety and health laws, around the world and under most national laws. For example, ILO Convention C155 was adopted in 1981 to require all employers to “formulate, implement and periodically review a coherent national policy on occupational safety, occupational health and the working environment” [4]. The UN Globally Harmonized System for the Classification and Labelling of Chemicals (GHS) includes 200 countries participating with private sector partners and United Nations Agencies in the worldwide chemical management system. These international and national laws are here to stay.
women’s health is a traditionally unresolved problem even in the paid workplace, under international laws society’s empirically established inability to deal with health disparities between men and women has harmed women historically and threatens to undermine the viability of Posterity
This reality is reflected in national and international laws preventing discrimination against people with disabilities, because those laws touch every part of daily life within and without the workplace, including education, accommodations for transport and housing and voting. The notion that accommodations can be required for people with disabilities without regard to the cause of their incapacity means that the international legal system is capable of being flexible to meet special needs, and therefore that similar accommodative systems could be created for women especially but not only during pregnancy and biological female related illness.
Thus the inexplicable sink hole in international legislation about work, health and survival of civil society: these key components of global health policy have not been synthesized into one workable women’s health strategy. To do so, however, requires synthesizing three broad categories of research that rarely interact. There is a little or no literature bringing together these three fields, and therefore this article represents a pathbreaking first step towards understanding and perhaps resolving major workplace health impacts that harm women, and therefore their children, families and greater society.

Slides by Dr Ilise L Feithsans JD and ScM and DIR used by permission 2017
There is plenty of work on occupational health programming even if it rarely examines women’s health, or looks at women’s health as a corner of an add-on about workplace health and then only if there are young women present does it examine reproductive health in the workplace, even though even an 80 year old woman can have ovarian cancer that had workplace causes. As the three circles defining broad realms of professional activity in this graphic demonstrate: there is a gap, a major hole in the finely woven policy analysis of work health and legal realms to protect human survival. This article is a very first attempt to examine the variables that will fill this hole with effective programs and meaningful legislation that will protect women, their health and in turn all of civil society.
sound occupational health programs that implement best strategies are the grease for the machinery of powerful economic engines.
Added to the underdeveloped realm of occupational health programming to address the health impacts on women, is the new technology that emerges in every workplace. Nanotechnology is the newest tool and a very exciting “revolution” in human understanding of the physical properties of matter.

“Health hazards of women workers have been traditionally under-estimated because occupational safety and health standards and exposure limits to hazardous substances a. based on male populations and laboratory test.”
Problems With the Traditional Model
EMBEDDED PREJUDICE IN RESEARCH
TRADITIONALLY Research has ignored women When reserch has included women it has used stereotypical working assumptions that do not reflect contemporary women’s changing exposures, stressors and special response to new technologies
It is important to note that “equity” is not “equality.” This subtle change of terms compared to early UN documents reflects recognition of the contribution of the disability community to the jurisprudence of human rights under international law. Specifically, disability is a confounder that militates against making everybody “equal.” For example, one cannot be fair to a person who is missing a leg by requiring everyone equally to walk up a flight of stairs in order to obtain free medical care. Conversely, making people equal by making everyone ill from workplace exposures would be a perverse endeavour. Thus, the law has evolved to seek fairness in outcome, even when “all things being equal, they aren’t,” by creating policies that attempt to have fair results. As noted in the same WHO report, which is not a legal document, but presents best practices for all employers: “Equity is just, impartial and fair. Gender equity refers to equal access, opportunity, control and benefits for women (compared to) men” [2].
Many risks faced by women in the workplace can appear deceptively simple or even unremarkable. For example, the cumulative impacts of stress arms and fingers among sewing machine operators, exposure to chemicals in cleaning or hairdressing jobs, and exposure to pesticides in agricultural work may impact reproductive health as well as overall well-being. WHO found that job and task segregation by gender results in different hazards in their respective workplaces, with attendant different impacts on health status. It is well known that heavy tools and work equipment are usually designed for men and may be unsuitable for an average woman or a small man. When using the term “gender equity,” however, international law recognizes the reality that there are biological, cultural, and perhaps legal differences between men and women. Rather than deploying the legal fiction that everything is “equal.” Instead, the goal of gender equity is to render differences between genders so unimportant that the results of our policies are inherently fair.
Health in the workplace is an excellent starting point for ensuring fairness regardless of gender, by filling the void created by the inexplicable sink hole in international legislation about work, health and survival of civil society: these key components of global health policy have not been synthesized into one workable women’s health strategy. The WHO Constitution provides a clear definition of “health” that has been recognized as international law for over 70 years. Ratified by the U.S. and nearly 200 other nations, the definition of “health” has been incorporated into many national constitutions: “Health is a state of complete physical, mental and social well-being and not merely the absence of disease and infirmity” [5]. There is no shortage of Global Mandates for Women’s Safety and Health Protections!
women’s health is a traditionally unresolved problem even in the paid workplace, under international laws society’s empirically established inability to deal with health disparities between men and women has harmed women historically and threatens to undermine the viability of Posterity.
B. GENDER EQUITY UNDER LAW

Global mandates for women’s occupational health protections define the industrial hygiene context for gender equity and require programs promoting gender equity and workplace health. This sounds complicated and maybe it is, but it is vital to survival of all society and the health of human posterity. Without question, this field has been ignored consistently throughout research history of the 20th century, if not longer. Yet that does not alter its importance. Problems fester and therefore the time has come to examine the effect of chemicals on women’s health in the workplace, and examine the importance of women’s health at work, regardless of the workplace venue, in relation to the greater public health and work environment.
“Is equity the same as equality?” was a long-standing question in international meetings throughout the 1990s. This question impacts the legal definition of “gender equity.” This term is often confused with similar terms like “gender equality,” “occupational inequality,” and “gender inequality,” but “gender equity” has a specific meaning under international law. The term “gender” has evolved to replace terms such as the language in U.S. law for differences “based on sex” because people may find themselves in gendered roles despite the sex of their birth that are the cause of inequality or discrimination by people around them. Health and safety hazards experienced by women can include pesticide exposure, heavy work resulting in stillbirths and premature births, musculoskeletal disorders, occupational cancer, respiratory diseases, illnesses caused by chemical agents, and work overload. The ILO notes that “health hazards of women workers have been traditionally under-estimated because occupational safety and health standards and exposure limits to hazardous substances are based on male populations and laboratory tests.” Women’s multiple roles in society and the effects of gender on health need to be further researched to understand the relationship between work and women’s health.
Achieving goals of gender equity in the workplace under international law requires that women workers at every level of society have the same opportunity to work in a place of employment that will not adversely impact their health [2]. Operationalizing this goal may require constructing programs that meet women’s unique needs, rethinking job hazard analyses of traditionally “female” jobs and tasks, and then embedding those needs into compliance programs that monitor workplaces, to ensure good health for all.
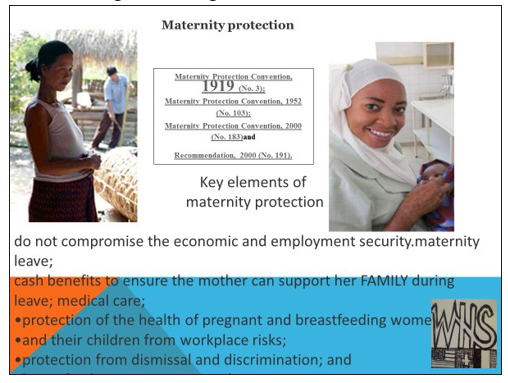
As revealed by the 20-year review of the United Nations (UN) Beijing Platform Document regarding the role of women, previously discussed in two publications from the American Society of Safety Engineers (ASSE), international and U.S. regulations associated with gender equity have been in place for several decades, but implementation is slow and in some regards society has regressed [6]. International initiatives such as the International Labour Organization (ILO) “Safe Maternity” programs, including the ILO Maternity Protection Convention, have set standards for pregnancy protections in the workplace, as a “shared responsibility of government and society” [7]. For example, the requirements of the ILO Maternity Protection Convention are now followed in the U.S. at Macy’s Inc. in their stored throughout the U.S. [8]. Additionally, the employment targets of the UN Entity for Gender Equality and the Empowerment of Women (UN Women) provide insight to a changed political climate favoring laws to enforce equitable employment for women that embraces safe and healthful working conditions with freedom from workplace discrimination [8]. The UN Convention on the Elimination of All Forms of Discrimination against Women (CEDAW) is widely considered an “international bill of rights for
women” since 1979. CEDAW established the following rights at work for women, which are still goals that employers struggle to achieve. Rights at work for women include:
• safe and healthful working conditions;
• rest, leisure, and reasonable limitation of working hours and periodic holidays with pay;
• Social security, including, but not limited to “special protections” such as paid leave and adequate benefits for women before and after childbirth [8].
The international framework for gender equity established by many treaty bodies of the UN, and the presence of anti-discrimination laws promoting gender equity exist in every nation reflects a universal commitment to gender equity under law at the local and national level. Even when the details of terms may conflict within a system, it remains true that the basic notions for promoting gender equity are found worldwide. For example, half a century ago, the Equal Employment Opportunity Commission (EEOC) was created by the U.S. Congress to enforce the civil rights of women and process discrimination claims associated with race, national origin, religious, and sex discrimination.
EU LAWS ABOUT GENDER & OSH
EU Council Directive 89/391 states: “Particularly sensitive risk groups must be protected against the dangers which specifically affect them.”
EU Council Directives 89/654 and 92/85 encourage improvements in OSH for pregnant workers and those who breastfeed, including restrictions on night work, provision of rest areas, and protection against tobacco smoke.
Finnish 058 80 738/2002 requires employers to account for reproductive health risks and to consider workers’ age, gender and other personal capacities.
Thus, laws mandating equitable treatment of women in the workplace are in place, plentiful and they are not going away. The plethora of laws mandating gender equity are justified because, according to WHO : Women in the workplace continue to be mainly responsible for domestic, unpaid work in their household or community, including cooking, cleaning, and caring for children and aged parents or disabled family

members. Informal sector workers are more likely to be women compared to men, with unstable wages and no benefits such as pension or insurance Unfortunately, informal and flexible work arrangements can be associated with reduced job security, reduced or non-existent benefits, inadequate training, unhealthy work conditions, underrepresentation and insufficient protections from governments and unions, and barriers to health care services because those employees do not qualify for health insurance or worker’s compensation. The impact of this inequity in underlying terms of employment may be seen in womens health disparities compared to men of their age or working cohort.
C183 - SAFE MATERNITY
Article 4
1. On production of a medical certificate or other appropriate certification, as determined by national law and practice, stating the presumed date of childbirth, a woman to whom this Convention applies shall be entitled to a period of maternity leave of not less than 14 weeks.
2. The length of the period of leave [...] including six weeks’ compulsory leave after childbirth, unless otherwise agreed at the national level by the government and the representative organizations of employers and workers. The prenatal portion of maternity leave shall be extended by any period elapsing between the presumed date of childbirth and the actual date of childbirth, without reduction in any compulsory portion of postnatal leave.
In the 20th session of the Human Rights Council of the UN General Assembly, the Special Rapporteur provided a report that describes the right of every person to enjoy the highest attainable standards of physical and mental health, including at work. The report states that occupational health must be considered an “integral component” of the right to health for every human. Consistent with Articles 7 and 12 of the International Covenant on Cultural Economic and Social Rights. When explaining the conceptual framework of the right to occupational health, the report identified the following basic elements of occupational health:
• Member States of the UN must improve all aspects of industrial hygiene, including the prevention, treatment, and control of occupational diseases.
• Preventive measures include minimization of health hazards inherent in the work environment using available technology and epidemiology.
• Women have a right to health and safety at work, including “safeguarding of the function of reproduction,” and should be provided special protection during pregnancy if the work they are doing has been proven to be harmful to them.
• Workers must be protected against sickness, disease, and injury resulting from employment as a fundamental human right.
• “Health” should be defined in the context of work as not just the absence of disease or injury, but also include the physical and mental elements affecting health.
• Industrial hygiene should include all efforts to protect worker health through “control of the work environment, including the recognition and evaluation of those factors that may cause illness, lack of well-being or discomfort among workers or the community” [9].
Proposed Rethinking of the Traditional Model to Reflect a Maternalistic View of Occupational Safety and Health, Thereby Protecting Reproductive Health for All A maternalistic view addresses the need for information about risks long before conception, taking a close and candid look at the risks and assets in the life of each potential parent, and then relating that information back to the workplace.
In the UN report on “Progress of the World’s Women 2015-2016,” Figure 2.3, “An Eye on the Gap,” illustrates the difference between participation in the labor force between men and women of prime working age, defined by the UN/ILO as between 25 to 54 years. The UN report presents the vision of women’s rights as compared to the reality, which is shown below in Exhibit 1. The vision for women’s rights to work and at work include: equal access to paid work; decent work, with social protection; fair and adequate earnings; and equal sharing of unpaid care work.
The report notes the gender gap is “striking and persistent” in all regions [10].
This means more than simply implementing kinder and gentler paternalistic mores regarding pregnant workers.
“Unfortunatelythat more fundamental issues of gender equity when crafting occupational health programs are left by the wayside, treated as an afterthought if though about at all” the law of reproductive health has become so bogged down in the quagmire of rhetoric surrounding reproductive “choice;”
There is a confluence of international laws promoting gender equity, and laws requiring hazard communication under the GHS or national legal systems, combined with laws prohibiting work in unsafe conditions, and laws prohibiting discrimination. It is in an employer’s best interest to take the initiative to provide and document such required protections, without waiting for workers to ask for help. It is critical to note that, according to WHO, the “major burden of disease in females is related to their reproductive function and reproductive potential, and the way in which society treats or mistreats women because of their gender.” WHO further cautions that “workplace exposures can affect reproductive health in various ways: sexual functioning, menstrual health, fertility (for women and men), pregnancy, breastfeeding, certain cancers (e.g. prostate, breast, cervix), menopause and children’s development.” WHO also suggests that these exposures may have a different impact for women and for men [11]. Thus, the same exposures may not provide equal results, and therefore a gender equity model may necessitate different approaches and different standards for women and men. In the U.S., the National Institute for Occupational Safety and Health (NIOSH) provides some basic points for employers and safety professionals to understand the basics of reproductive hazards in the work environment [12].
• Women’s fertility and menstrual function can be affected by some workplace hazards.
• Both men and women can carry chemicals home on the skin, hair, clothes, and shoes. Some of these chemicals can harm the health of children, pregnant or breastfeeding women, and other people in their households.
• When a pregnant or breastfeeding worker is exposed to hazards, her baby might be exposed too.
• Some chemical exposures might be riskier for an unborn but there is precious little research regarding which exposures might harm an unborn baby.
• Many chemicals in the workplace remain untested regarding reproductive problems.
• Laws for workplace safety and health may be inadequate to protect men’s and women’s reproductive health despite known reproductive health hazards in the workplace.
The American College of Obstetricians and Gynecologists has published a brief entitled “Exposure to Toxic Environmental Agents” that explains some reproductive health effects from known chemicals that are present in many workplaces. Some examples of environmental contaminants that have reproductive health effects are listed in Appendix 1 of this paper [13]. Recent changes to OSHA’s Hazard Communication regulations, including the alignment with the UN’s GHS system, mean it has become simpler to educate workers about the chemical hazards they may face in the workplace. In the 2012 Hazard Communication standard, all of the following health concerns are noted under the “Health Hazard” pictogram carcinogenicity, mutagen city, reproductive toxicity, respiratory sensitizer, and target organ toxicity. One of the few aspects of workplace health where a difference in the impact upon health of men compared to women has long been recognized is response to stress. Yet, male paradigms for stress at the workplace have dominated occupational epidemiology for years, and few studies take into account the important role of household and family stressors that impact women’s health at work; sometimes the stressful demands of work and family members are inseparable.
Reproductive health: a women’s issue or a question of gender equity?
One of the greatest stressors in life surrounds the question of whether to parent a child. Yet, workplace safety and health programs have traditionally been ambivalent about this subject, or have misunderstood why supporting this worker decision is important, despite it being an intensely stressful issue. While it is true that reproductive choices are often beyond the scope of employment, it is also true that stress and uncertainty surrounding these personal choices may have an impact on the workplace with a concomitant effect on worker health. Many of the traditional workplace contexts for dealing with workers’ choices to become a parent are changing; some workplaces proudly proclaim that they are “baby-friendly” or “family friendly,” offering infant breast-feeding programs and space for toddlers. Whether these changes are due to the improving economy, implementation of new technology, or the success of international gender equity programs, it appears that employers are rethinking the previous tradition of ignoring family concerns in the workplace.
Research is needed and attention should be paid to key reproductive choice issues that have previously been ignored: not simply the question of whether pregnant workers or a fetus should be allowed in the workplace, but also whether workers should be encouraged to delay procreation by insurance coverage for any or all of the following: sperm preservation, egg “freezing” (as currently available through employers such as Google), a variety of contraceptive procedures, and abortion. The UN CEDAW noted that a woman’s right to reproductive and sexual health is key to women’s health; a presentation by Dr. Carmel Shalev, an expert member of CEDAW, noted that these rights are persistently violated in areas such as maternal mortality, inadequate allocation of resources for family planning, coercive population programs, and workplace discrimination of pregnant women [14].
• Evaluate and address potential differential impacts of work organizational factors on health and well-being of both women and men workers.
• Encourage a zero-tolerance policy towards all forms of violence and discrimination that encourages the reporting of violent incidents.
• Without restricting women’s access to jobs, address women’s concerns about working alone, working late, and provide access to safe parking facilities.
• Educate workers on the issue of violence and explain avenues available for help or support.
• Perform periodic training for managers and supervisors on work-family balance, workplace violence, and health and safety issues from a gender perspective.
• When possible, have formal flextime arrangements, self-scheduling, schedule exchanges, telework or virtual work, compressed workweeks, predictable working hours, paid or unpaid leave for family emergencies or prolonged illness of a family member, and parental leave after the birth or adoption of a child.
• Institute workplace policies on workplace daycare, if possible.
• Provide a clean, private room for breastfeeding or breast milk pumping; this eases women’s return to work following maternity leave.
• Establish accessible/affordable communication pathways that so that workers are able to attend to family responsibilities during work hours, especially emergencies.
• Institute a work culture that is supportive of family responsibilities/ relationships.
• Part Three How Do We Do THIS? Bringing Gender Equity to Effective Compliance Programs
The international legal community and civil society have repeatedly stated in reports and instruments that have been ratified by the UN Member States ILO relating to occupational health and safety, including the Convention on Occupational Safety and Health, No. 155 (1981); the Working Environment (Air Pollution, Noise and Vibration) Convention, No. 148 (1977); the Occupational Health Services Convention, No. 161 (1985); and the Protection of Workers’ Health Recommendations, No. 97 (1953). Most importantly, the report states that workers must be involved in the decision-making processes relating to occupational health law.
Compliance program models are applicable globally across many types of operations. In-house occupational safety and health compliance programs serve two major functions: (1) providing clear evidence of an enterprise’s commitment to obeying the law, while (2) identifying hazards in time to reduce costs and potential liability [15]. Key components include but are not limited to employer due diligence, audit reports, embedding compliance programs within the employer’s “infrastructure,” and in-house communication concerns for employers.
For example, in the U.S., the OSH Act of 1970 provides the following “general duty clause” in Section 5: that employers must provide “a place of employment which are free from recognized hazards that are causing or are likely to cause death or serious physical harm” [16]. This term includes a wide variety of potential harm. The U.S. OSH Act of 1970 and general duty clause emphasizes each employer’s responsibility to recognize, correct and reduce potential hazards. The law does not state a preference based on gender, it is “gender neutral.”
Bringing Health to Work is Required by Law
A compliance program must: (1) expand the scope of audits beyond policies, to include procedures; (2) take affirmative steps to “find out what’s going on”; (3) empower compliance personnel; (4) discipline with vigor; and (5) clearly document activities in the compliance program; without documentation, the program never happened. The difference between “genuine” or “meaningful” compliance and “sham” compliance programs, however, is found in their implementation. Enhancing in-house occupational health compliance infrastructure involves describing the “how to” of in-house compliance programs to each member of the staff, from the top of the organization to the lowest echelons.
Effective management systems use approaches honed by regulators to prevent, detect, report and correct failures in occupational safety and health. For example, OSHA’s Voluntary Protection Programs (VPP) require identifying occupational health problems to prevent future harm, by requiring job hazard analysis, management commitment and employee involvement [17].
Compliance staff must have a command of occupational health laws, health insurance regulations, and laws prohibiting discrimination based on age or disability, and perhaps even federal entitlements to social security for workers near retirement as part of routine compliance practices. Staff must have the good sense to apply sound information about immediate dangers, despite the undercurrent of pervasive risks, in order to steer clear of danger. Compliance staff must also have the power and professional integrity in order to use sound occupational health information, even in the face of a storm of controversy regarding the potential economic loss or other costs associated with withdrawing or changing plans.
Compliance programs therefore provide the constant, although ever-changing means, for an employer to demonstrate due diligence complying with law, by offering the in-house blueprint to conduct simultaneous oversight in several areas of law: preventing discrimination based on age, gender, race, ethnicity, religion, or disability combined with health insurance requirements and laws preventing environmental harm. Technology and the impact of globalization have dramatically altered the nature and organization of work in the United States and throughout the world [18]. This requires a new approach taking into account a wide variety of special individual needs, custom tailored workplace protections rather than offering a “one size fits all” approach.
Due Diligence Is Your Best Friend
An Introduction
To be effective, a compliance program must be able to prove itself. This requires that the program be documented in order to prove that the employer has complied with the law. Each in-house compliance program must decide for itself the area of emphasis that will best foster compliance, specific to the workplaces and the demands of the tasks at hand. This requires examining the relative advantages and weaknesses of different components of effective occupational health programs.
Due diligence requires developing committee structures and, then the regular use of a smooth-flowing, on-going infrastructure for improved communications for training and for reporting compliance problems. The in-house compliance program for safety and health cannot be treated as if it were a trade secret. A clear organizational structure allocates in-house compliance tasks and makes in-house staff accountable for the achievement of compliance program goals and objectives. These goals and objectives should be stated by the employer’s actions and in its written policies.
Implementation of the compliance approaches in these programs can assist organizations to anticipate areas where compliance failures may arise employing hotlines, committees and other compliance tools to prevent systemic failures. One key tool is the internal audit, and there are several examples of the major components of audit systems offered in legislation. According to the Texas Environmental Health and Safety Audit Privilege Act : “Environmental or health and safety audit means a systematic voluntary evaluation, review, or assessment of compliance with environmental or health and safety laws or any permit issued under those laws.”
What to Include in Audit Reports
Audit reports typically include:
1. a report prepared by an auditor, monitor, or similar person, which may include:
a. a description of the scope of the audit;
b. the information gained in the audit and findings, conclusions, and recommendations; and
c. exhibits and appendices;
2. memoranda and documents analyzing all or a portion of the materials discussing implementation issues; and
3. An implementation plan or tracking system to correct past noncompliance, improve current compliance, or prevent future noncompliance [15].
Due Diligence is Your Best Friend
Due diligence is the fundamental concept for crafting and implementing effective in-house management systems for occupational health compliance that avoids liability. In many legal systems, the strongest systems are cyclical as noted in the cyclical graphic below by Dr. Mark Hoover, et al., the American Industrial Hygiene Association (AIHA) and NIOSH [19].
The most reliable risk management decision making framework is cyclical. As adapted by AIHA and NIOSH (American Industrial Hygiene Association, 2015), the framework should include training, documentation, and continuous improvement between each element. NIOSH and AIHA use the term “ARECC” as shorthand for the five elements of risk management, “Anticipate, Recognize, Evaluate, Control, and Confirm” repeated at reasonable intervals.
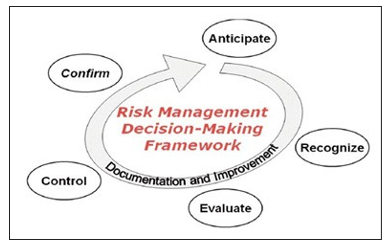
Industrial Hygiene Risk Management Decision-Making Framework
Hoover, M., Armstrong, T., Blodgett, T., Fleeger, A., Logan, P., MacArthur, B., & Middendorf, P. (2011, October). Confirming Our Industrial Hygiene Decision-Making Framework. The Synergist, 10-11.
The notion of a cyclical system makes reporting normal as well as required, with built-in follow up as well as long term accountability. With the help of corporate anthropologists and outside consultants, staff can be briefed about key issues, when designing the overall in-house approach to occupational safety and health right to know training, tailored to corporate culture of a specific enterprise and thereby creating a specialized system with effective results. Key steps towards touching each of the baes in this cycle include:
1. setting procedures that are capable of reducing illegal acts;
2. assigning high level personnel to compliance;
3. preventing the delegation of authority to people who are likely to engage in illegal activity;
4. effectively communicating standards and procedures to all employees;
5. implementing reasonable compliance measures such as monitoring, auditing and reporting systems;
6. using discipline to enforce standards;
7. taking appropriate steps to detect and correct offenses, including changing the program as necessary; and
8. Understanding that repeated compliance activity requires diligent monitoring to prevent harm.
Design Components of Due Diligence: Embedding Compliance
Compliance programs offer concrete proof of due diligence, and thus allow an employer to enjoy a legal presumption of compliance in litigation or regulatory enforcement actions where the limits are unknown. To do so, however, requires candid ongoing detailed scrutiny of internal problems within the worksite, as well as documentation of every reasonable effort for troubleshooting and creating the most reasonable solutions to those problems.
Effective in-house OSHA compliance programs require the best possible lines of communication in order to be successful. In order to work, lines of communication must be established long in advance of any emergency. Such efforts can also facilitate compliance with new changes or modifications in the federal law because of their inherent flexibility. The so-called “paper trail” is dependent entirely upon proving this concept of “due diligence”.
Embedding compliance values into the corporate culture and its infrastructure may be viewed as an essential step towards constructing and implementing a system of mandatory procedures integrated into operations, designed to ensure that proper compliance with the law is actually achieved to the maximum extent practical. When it works perfectly, an embedded value will also function as a safety “valve” that prevents the flow of inappropriate concepts from gaining currency throughout the system. Embedding compliance therefore extends beyond operating divisions, and embraces everyone affected by the system, from the chair-of-the-board to the custodial staff, ensuring that all employees are subject to policies and procedures that are applicable to their particular functions.Significantly, if the correct values have been embedded into the infrastructure, illegal or irresponsible activities will be prevented by the system itself. This applies not only to manufacturers, chemical plants, steel mills – or any businesses that have a greater degree of physical risk for workers – it also applies to all other businesses that have an established workplace with key staff.

The concept of embedding values into the employer’s infrastructure is not novel. Starting in 2016, the UN has released 17 Sustainable Development Goals (SDGs) to address a host of social reforms by 2030 that were adopted by world leaders in 2015; these SDGs strive to end gender inequality, improve health and well-being, and provide decent work for improved economic growth [20]. Such strategies are not mere add-ons that one inserts carefully to retrofit existing standards. The value added by these goals improves the economic well-being of workers, their employers, and their health and their families immeasurably.
WHAT NEXT?
So the two first crucial parts of solving the riddle of women’s health protections at work already exist. We have law mandating occupational helath rograms and law mandating gender equity. What does this mean for nanotechnology in the workplace? All the world has proclaimed hat nanotechnology is a “revolution” for science. The rules change at the nanoscale; silver becomes anti-bacterials and gold become combustible Will empirically documented gender-based health disparities between men and women be reproduced, OR improved, following the widespread use of nanotechnology? The World Health Organization has documented health disparities that exist between men and women (2009) and concluded that women’s health lags behind their male cohorts at five key stages of the life cycle: 1. birth to 5 years, 2. adolescence (including implications of adolescent pregnancy) 3. Reproductive years 4. Post-reproductive years (menopause and greater risk for cancer among sex-based target organs) and 5. Advanced aging (65-80 years). It remains unknown but an intriguing legislative policy question, to what extent nanotechnology in the workplace will either exacerbate or remove those disparities. Womens health disparities will become more difficult to grasp after nanotechnology takes hold because the extent of nanoparticle expsoure in cosmetics, food, daily exposure to consumer products (such as automobile tires, paintings and coatings and refrigerators used in food transport). This potential cumulative effect will be more complex than any synergistic effect that epidemiology has attemepted to measure before. Lessons learned from the late twentieth century initiatives that funded “Big Science” teach us that governments can use regulatory programs to supervise and promote risky new technologies, without creating a new race of genetically -engineered monsters or blowing up the whole world.
Wise people will therefore try to foresee inevitable but presently unknown nanotechnology risks. Then they will try to address these anticipated risks with best practices, codes of conduct and scientific principles to prevent harm under international law. Key public health policy questions to explore regarding nanotechnology, nanomedicine and the possible disparate impact upon women’s’ health include but are not limited to:
1. Impact on access to high quality care
2. Rethinking the distribution of public health care and delivery of health services
3. Rethinking the role of public health compared to private insurance
4. Rethinking the role of key illnesses and injuries in the global disease burden
5. Rethinking notions of informed consent as presymptomatic testing diagnosis and treatment using nanomedicine becomes a reality
6. Changing paradigms for patient choices and ‘informed consent” in light of “personalized medicine”, which applies nanotechnology techniques to pre-existing genetic and protenomic information about the individual patient
7. Discussion of the role of rehabilitation as a source of return to gainful work among aging populations who might not have considered working without the benefits of nanomedicine, a “revolving door” approach to long term disability care and chronic illness treatment
8. Clarification of the role of different exposure sources; workplace, home and ambient environment
If indeed the change is a revolution then we can use this opportunity to discard the harmful paradigms that ignored womens health outcomes by ignoring womens rights. This means that new research with a new maternalistic view of health should examine each of the 4 bricks of the hierarchy of controls, and fill in the blanks with protections and data that meets womens health needs.
III. The Moscow Declaration on Reproductive Health at Work: The Call For Maternal-Based Research into Environmental and Occupational Impacts on Health
In light of this impressive but dormant body of international human rights law, the Committee of Experts on Reproductive Health at Work the conference “Medical and Ecological Problems of Workers’ Reproductive Health” was held December 9-10, 1998, in Moscow, Russia. In a satellite meeting on December 11, 1998, the Committee of Experts on Reproductive Health at Work (COERHW) unanimously adopted “Declaration Position Statement and Proposed Plan of Action for Period up to 2000 and in 21st Century on Workers’ Reproductive Health Protection” which was unanimously adopted with instructions that it be sent before February 1, 1999, to WHO Director_General Dr. G.H Brundt land, According to the data presented at the conference, alarming changes in vital statistics regarding increased miscarriage, infertility, death from infectious diseases, pregnancy anemia, and complications from pregnancy threaten to undermine the health of every pregnant worker and challenge the viability of humanity for all posterity. At the same time, in areas of ecological catastrophe, reported data indicate that the death rate has increased even as the birth rate declines. Thus, in many different nations for different reasons, reproductive health among all people has declined in recent years, with a demonstrated disproportionate adverse impact on the health of working women. Some of these dramatic increases in pregnancy-related illness cannot be understood in relation to the injury and illness experience of male workers, nor can they be explained by simply claiming that increased illness that is found among women workers is a result of working womens significant double burden. Participating researchers offered methods of assessing the structure and degree of work-related disorders; noted that the issues raised by research examined at the conference transcends international borders in a manner that threatens to undermine international human rights to health; and offered an approach to integral evaluation of health risk categories based on simultaneous understanding of the physical and chemical work load in work environments within the greater ecological context of the territory in which the worker resides, so that the best possible risk assessment can be made and every available resource for risk management can be employed. In addition to the COERHW’s unanimous consensus regarding the Declaration, there was a strong sentiment among the Members that simply articulating a Plan of Action would be inadequate to address the long-term implications of the urgent problems surrounding reproductive health and hazardous exposures at work. Although the Members agreed to limit their formal activity to a Declaration, thereby taking an incrimentalist approach, there was widespread agreement that the Declaration was merely the first step in a long process, given the scientific data discussed above. Some of the issues that were discussed within the Committee but were not specifically addressed in the Declaration may become the subject of future deliberations, when the Committee reconvenes to report on the progress towards its goals and to discuss any proposed draft international convention.
Due to time constraints and the preliminary nature of the Declaration itself, many subjects were raised and tabled for future deliberations, including: mechanisms for risk communication to workers; the scope of the right to know information about reproductive health hazards in the workplace; minimum and maximum standards of protection; how to address the special needs of pregnant workers and workers with young children. Left unsettled, also were the questions about the Right to refuse hazardous work for all workers and whether there are reproductive health hazards that are so problematic and dangerous that exclusion would be advised or required for workers contemplating childbearing, for pregnant women or other sub-populations such as young children in those industries where dangerous substances may have a long half-life that could render them functionally impaired. Questions regarding smoking and alcohol use were also put aside, because of the difficulties when teasing apart personal liability, risk, and synergy with workplace toxins. These issues may be addressed during future meetings.
Despite widespread scientific consensus that a fetus is uniquely at risk from dangers in the workplace, there is no scientific or legal consensus about how to address this eternal conundrum, universally part of the human condition. A recent thread of discourse on the occupational medicine listserve once again raises the perennial question that has, for a century, been unanswered in occupational health: Is there a legal basis for employing special risk assessments or additional preventive strategies to protect fetal health when pregnant women are exposed to workplace hazards that may contribute to adverse pregnancy outcome(s)? This policy question holds special importance for the future productivity of the American workforce and the society at large.
The University of Medicine and Dentistry of New Jersey-School of Public Health (UMDNJ-SPH) with in 2002 sponsored a field-work project which was a feasibility study of corporate reproductive health policies among 14 employers, each with over 1,000 employees. The study included worksites in the chemical, pharmaceutical, insurance, health care, automobile and technical industries in New Jersey. The survey consisted of questions regarding current reproductive health policies, practices and hazardous exposure prevention, including legal issues pertaining to employer obligations and workers’ rights. The results suggest that although 14/14 (100% of responding employers in the survey) unanimously stated they are in compliance with law, very few of these same employers offered in practice the features of compliance required under these laws. For example, most (9/14) of the companies stated that specific reproductive health policies (RHP) are in place at their sites, yet the vast majority (12/14) reported that specific or individual protective policies for different work stations do not exist at their sites. Furthermore, most (8/14) companies stated that female and male workers do not receive special training about worksite exposures to reproductive health hazards.
This suggests that there is a major disconnect between the theory and practice of in-house compliance regarding OEM approaches to reproductive health hazards in the workplace. The report2 concluded that few large employers actually provide the training and/or equipment that is necessary to inform workers and prevent reproductive health hazards at work, despite nominal statements of compliance. . The tangible results of this project, incorporated into a Model In-House Corporate Compliance Policy for reproductive Health at Work will enable employers to foster the on-going employment of trained and skilled workers who wish to found their family to enjoy enhanced work productivity during their reproductive years. In sum, there is an obvious but ill-defined gap between the requirements for employment of pregnant workers under law, the needs of peri-conceptual workers both male and female, and the reality of daily workplace practices as reflected in either actual work or implementation of in house corporate compliance policies.
Conclusion
The sheer economic force of nanotechnology in commerce will take the changed rules of science and rewrite the rules of global business. The window of opportunity therefore exists to also rewrite the rules governing civil society’s approach to women’s occupational health. Whenusing the term “gender equity” rather than “gender equality,” we suggest an international recognition of the fact that there are biological, cultural, and perhaps legal differences between men and women that cannot make everything inherently equal. However, in the workplace and the greater society that is served by our work, we want that difference to become unimportant, so that the results of regulations and policies are fair. This means making sure that every worker, regardless of gender, has the safety and health protections necessary to enjoy the right to a safe and healthful working environment.
Achieving goals of gender equity while providing a safe and healthful working environment is not only required, but an important feature of due diligence in every employer’s compliance program and the long-term impact of reproductive toxins from workplaces on the health of our posterity.

The future of personalized/individualized medicine, including using genetic engineering and nanotechnology for precision medicine, may change the focal points of these questions of gender equity. We hope that as social barriers in the workplace are removed, women will be treated fairly in places of paid employment throughout the international workplace. In this context, safety engineers and occupational health professionals are on the front lines in a winning battle to do the right thing. We can help to achieve gender equity in the workplace by providing sufficiently protective health and safety standards for all workers.
Researchers should encourage recordkeeping that can be stratified by sex as well as accident/illness data hours of work Nature and duration of exposures.
Former Guest Researcher at NCRWE Copenhagen
Legal Advisor for the Greek National Platform on Nanomedicine
Swiss 0041 79 836 3965 USA 917 239 9960
forecastingnanolaw@gmail.comhttps://www.facebook.com/
messages/t/100012810330919
Author, Council of Europe Handbook for Parliamentarians on the Ratification of the Convention Preventing Medicrime (English and french versions available on the web coe.int) MS-JD Writer in residence on international Law
Award Recipient MS-JD SUPERWOMEN- JD conference 2016 Expert on Nanotechnology for the Parliamentary Assembly of the Council of Europe Author of several books and hundreds of published articles about health, technology, nanotechnology, education, disability, assistive technology for people with disabilities.
NEW BOOK!! GLOBAL HEALTH IMPACTS OF NANO TECHNOLOGY LAW
• Appendix 1: Chemicals with Reproductive Health Effects
• Examples of chemicals with known reproductive health effects [13].
• Pesticides – can be ingested, inhaled, and absorbed by the skin; lead to impaired cognitive development, neurodevelopment, and fetal growth, as well as increased childhood cancer
• Solvents – examples include benzene, toluene, xylene, styrene, perchloroethylene, trichloroethylene; exposure is primarily through inhalation; lead to fetal loss and miscarriage
• Toluene – exposure is primarily through inhalation; leads to decreased fetal and birth weight and congenital malformations
• Phthalates – can be ingested, inhaled, and absorbed by the skin; leads to shortened gestational age and impaired neurodevelopment in girls • Lead – can be ingested or inhaled; leads to intellectual impairment and increased likelihood of allergies
• Mercury – exposure is primarily through ingestion of contaminated seafood; leads to reduced cognitive performance and impaired neurodevelopment
• Polychlorinated Biphenyls – exposure is primarily through ingestion from various animal products; lead to development of attention deficit and hyperactivity disorder-associated behavior, increased body mass index, and reduced IQ
• Air Pollutants – examples include carbon monoxide, lead, ground-level ozone, particulate matter, nitrogen dioxide, and sulfur dioxide; exposure is primarily through inhalation; lead to low birth weight and birth defects
• Cigarette Smoke – exposure is primarily through inhalation; leads to miscarriage, low birth weight, and preterm delivery
• Perchlorate – exposure is primarily through ingestion of contaminated products; leads to altered thyroid function
• Perfluorochemicals– can be ingested, inhaled, and absorbed by the skin; lead to reduced birth weight
• Polybrominated Diphenyl Ethers – can be ingested or inhaled and bio-accumulate in the environment; lead to impaired neurodevelopment, premature delivery, low birth weight, and stillbirth
• Bisphenol A – can be ingested, inhaled, and absorbed by the skin; leads to recurrent miscarriage and aggression/ hyperactivity in female children
• Formaldehyde – can be ingested, inhaled, and absorbed by the skin; leads to spontaneous abortion and low birth weight
• Antineoplastic Drugs – can be ingested, inhaled and absorbed by health care workers; lead to spontaneous abortion and low birth weight
• Anesthetic Gases – exposure is primarily through inhalation; lead to congenital anomalies and spontaneous abortion
• Ethylene Oxide – exposure is primarily through inhalation; leads to spontaneous abortion and pregnancy loss as well as preterm and post-term birth
Appendix 2: DECLARATION_POSITION STATEMENT AND PROPOSED PLAN OF ACTION FOR PERIOD UP TO 2000 AND IN 21st CENTURY: ON WORKERS’ REPRODUCTIVE HEALTH PROTECTION
(Adopted by the International Conferenc_Medical and Ecological Problems of Workers Reproductive Health, 9_10 December 1998, Moscow, and refined by the Informal International Consulting Meeting of Experts on Reproductive Health Protection, 11th December 1998, Moscow, Russian Federation) To insure optimum reproductive health protection worldwide, the Members of the International conference and Informal meeting of experts believe that there is an urgent need for elaboration of international consensus statements as well as the Plan of Action.
BACKGROUND INFORMATION
As satellite venture to the Conference on 11 December 1998 the Informal International Consulting Meeting of Experts on Reproductive Health Protection was held organized by the Initiative group (Dr. O.Sivochalova, Dr. E.Denisov, Prof. I. Figa_Talamanca, Dr. T.Vergieva, and Prof. I. Feitshans as Member and Legal Advisor). In the Consulting Meeting 21 specialists have participated from Belarus, Kazakhstan, Poland, Russia, Tadzhikistan, USA as Attending experts and 4 specialists from Bulgaria, Canada, Italy and Ukraine as Ex Officio experts (contributing by fax and e_mail correspondence). Chairpersons of the Meeting were Prof N. Izmerov, Director of the RAMS Institute of occupational health and Dr. O.Sivochalova, Head of the Centre of Medical and Ecological Problems of Workers, Reproductive Health of this Institute .Declaration_Position Statement and Proposed Plan of Action for Period up to 2000 and in 21st Century on Workers’ Reproductive Health Protection have been unanimously adopted by the Committee of Experts.
INTRODUCTION
As recently called for by His Excellence, Mr. Kofi Annan, Secretary_ General of the United Nations, the International Organizations, such as the ILO and the WHO and the national governments throughout the world should give occupational health and safety higher priority of their agendas. This would be necessary to respond effectively to the health and safety needs of working people and thereby promoting the overall socioeconomic development and well_being of countries and people. Dr. Gro Harlem Brundtland, Director_General Elect of the World Health Organization in her speech to the Fifty_first World Health Assembly emphasized: 2WHO can and must change. It must become more effective, more accountable, more transparent and more receptive to a changing world.
Recognizing the urgent need for improved primary care, protection of mothers, working parents and their children for the benefit of the family and the urgency attached to the problem of understanding the interaction between workplace exposures, environmental factors and preventing worker exposures that jeopardize familial health and human reproductive health, the Committee of Experts hereby calls upon the Director_General of WHO to use her good offices to foster further understanding, research and international co_operation in the following areas to prevent and reduce known or expected hazards to reproductive health AND RECOGNIZING THAT many conventions that suggest there is an international need and obligation to address these issues, but no single comprehensive internaitonal instrument about reproductive health in the workplace addresses these issues directly nor does any such instrument adequately ensure access to information and risk communication for all people who confront reproductive health hazards at work;
The following proposals are based on updated principles and practices and should be considered as background for better reproductive health protection for every worker.
GENERAL STATEMENTS
According to the UN definition, “Reproductive health is a state of complete physical, mental and social well_being and not merely the absence of disease or infirmity, in all matters relating to the reproductive system and its functions and processes... reproductive health care is defined as the constellation of methods, techniques and services that contribute to reproductive health and well_being by preventing and solving reproductive health problems”.
The Committee of Experts,
HAVING REGARD TO THE Aims and Principles of United Nations Charter, Universal Declaration of Human Rights, International Convention on the Elimination of All Forms of Discrimination Against Women, International Convention on Child Rights, UN Conference on Environment andDevelopment, on Population and Development, on Women, WHO Constitution, Alma Ata Declaration (1978) and AHealth for All 2000”, WHO Global Strategy for Occupational Health for All (1996), WHO revised policy document Health for All in the 21st Century (to be issued later), ILO Conventions and Recommendations on women workers, specifically but not limited to: C.103 Convention Concerning Maternity Protection (1952), C.165 Convention Concerning Employment Protection and Protection Against Unemployment; C. 156 AConvention Concerning Equal Opportunities and Equal Treatment for Men and Women: Workers With Family Responsibilities”, and C. 155 Convention Concerning Occupational Safety and Health, Related regional and national directives and recommendations namely Council Directive 92/85/ on safety and health of pregnant workers and RECOGNIZING First that preserving any and every wage_earner’s health and ability to enjoy reproductive health is essential to family life; to preserving the family; and protecting the next generation for posterity and RECALLING the WHO view that health is tied to the prevention of impairments and the ability to participate in all life activities, and that the WHO should endorse a Plan of Action in this Declaration to address this urgent problem the Committee of Experts hereby FINDS AND DECLARES: At present experts in many countries express serious anxiety about unsatisfactory health status of population especially of reproductive health as well as of children’s health due to influence of hazardous occupational and environmental factors (physical, chemical, biological agents, physic loads and nervous stresses9[xii]). In some countries on the background of social and economical problems a critical situation in population reproduction have formed which threatens their sustainable development, especially for countries with transitional economies. Many pregnant workers have been denied access to primary care in occupational health services or in the health care delivery systems of the different nations and this grave situation causes further deterioration of maternal and child health and the well_being of all society.
The International Conference on Population and Development (Cairo, 1994) and the Fourth World Conference on Women (Beijing, 1995) have together focused on the need for all countries to examine policies and practices related to broader health concerns, bringing in both a human rights and a gender perspective. According to modern approach adopted ILO and WHO reproductive health of both genders (men and women) should be protected and promoted as part of general health. Women in some periods of reproductive life (women of fertile age, pregnant, recently delivered and breast_ feeding) as well as children and adolescents should be considered as vulnerable groups i.e. high risk groups and need supplementary protection. In fundamental medical sciences by mutual efforts of professional community the concept of reproductive health is emerging as topic of the highest medical and social priority. The Meeting of Experts was an extension of other actions in the field namely Expert meeting AWomen at work@, 10_12 November 1997, Helsinki, Finland where it was suggested to develop an International legal document on the health protection of women at work, including pregnant women.
ISSUES
Priorities in research and for primary health care system and occupational safety and health service Notwithstanding the progress in maternal and child health and in reproductive pathologies, some problems persist, and are even in the increase. A high proportion of concept uses is lost prematurely, manifested as sub_fecundity and infertility, the rate of spontaneous abortion seems unchanged, congenital defects are a continuous problem, while childhood cancers are increasing. According to some, but not all studies, fertility and sperm quality are decreasing. Although research efforts have considerably increased in this area in recent years, there are still many open questions. Some examples are the following:
![]() Is there a differential susceptibility of the female versus the male organism to exposures of chemical and physical agents in the work environment,
Is there a differential susceptibility of the female versus the male organism to exposures of chemical and physical agents in the work environment,
![]() How justifiable are differential standards and limits of exposure for the two genders, are present day work exposure limits sufficiently low to protect the reproductive health of men and women,
How justifiable are differential standards and limits of exposure for the two genders, are present day work exposure limits sufficiently low to protect the reproductive health of men and women,
![]() Is there a true reduction in human fertility (and sperm quality), in the industrialized countries, and what may be the risk factors involved,
Is there a true reduction in human fertility (and sperm quality), in the industrialized countries, and what may be the risk factors involved,
![]() How do factors previously neglected such as stress, shift work, work with new technologies, affect reproductive health,
How do factors previously neglected such as stress, shift work, work with new technologies, affect reproductive health,
![]() Are the known reproductive risks under control, and how can this be accomplished?
Are the known reproductive risks under control, and how can this be accomplished?
![]() Particular attention must be paid to the health of working women, a subject that has been neglected in both developed and developing countries. To fill this gap, it is important that the following steps be undertaken by governments and international organizations:
Particular attention must be paid to the health of working women, a subject that has been neglected in both developed and developing countries. To fill this gap, it is important that the following steps be undertaken by governments and international organizations:
![]() Studies in the production sectors which employ predominantly female workers. These include both paid and unpaid (invisible) work in agriculture, in domestic labor, in garment, textile and food industry, in the health care sector.
Studies in the production sectors which employ predominantly female workers. These include both paid and unpaid (invisible) work in agriculture, in domestic labor, in garment, textile and food industry, in the health care sector.
![]() Identify reproductive risks for both men and women in these settings, and prevent exposures of those more vulnerable.
Identify reproductive risks for both men and women in these settings, and prevent exposures of those more vulnerable.
![]() Take account in studies of the double load of women workers, and of family and other stresses.
Take account in studies of the double load of women workers, and of family and other stresses.
![]() Most reproductive hazards are dangerous to both males and females. Research should examine both. Selective overprotection of women may compromise employment opportunities of women, condemning them to poverty.
Most reproductive hazards are dangerous to both males and females. Research should examine both. Selective overprotection of women may compromise employment opportunities of women, condemning them to poverty.
![]() Document the many forms of exploitation and illicit labor in developing countries, especially among adolescent girls and child laborers. These phenomena, although macroscopic are not sufficiently documented, and are often tolerated by local authorities.
Document the many forms of exploitation and illicit labor in developing countries, especially among adolescent girls and child laborers. These phenomena, although macroscopic are not sufficiently documented, and are often tolerated by local authorities.
![]() Document the deprivation and reproductive risks of migrant workers, who seek employment and survival in western countries. For them too, documentation and intervention programs are deplorably scarce.
Document the deprivation and reproductive risks of migrant workers, who seek employment and survival in western countries. For them too, documentation and intervention programs are deplorably scarce.
Considerations for the need of specific approach in studying reproductive health at work
A number of chemicals are with a short half_life in the organism and a certain endpoint (as for example a birth defect) might arise only after exposure in the respective sensitive period of gestation, the necessity of studying a range of endpoints including sensitive ones and subtle changes as minor birth defects and postnatal functional deficits. Investigation directed to reveal dose_effect and dose_ response relationship for proven and/or suspected reproductive and developmental hazards.
Examination of additional and eventually new endpoints for reproductive toxicity. Studies on contribution of combined exposures. Exploration of potential reproductive hazards of new technologies, for newly introduced occupational chemicals and other agents as well as in branches of industry which have not been considered yet. Development of study protocols and statistical approach to deal with the problem of small numbers of employees in specific occupational settings and being exposed to specific hazards.
Implementation of models for monitoring reproductive health of workers and subsequent use of these data for epidemiological studies. Further refinement of the protocols with inclusion of individual exposure data relevant for the respective endpoint period in case control studies nested in a follow_up cohort. Encouraging occupational health services in reporting eventual clusters of mis_events in reproductive health and with the help of other specialists organizing at spot of follow_up studies.
Proposed Action to fill the gaps in existing international and state laws Regarding the role of workplace exposures in shaping reproductive health outcomes:
The Committee of Experts Notes that there are many conventions that suggest there is an international need and obligation to address these issues, but No single comprehensive international instrument about reproductive health in the workplace addresses these issues directly nor does any such instrument adequately ensure access to information and risk communication for all people who confront reproductive health hazards at workAn initial survey of international laws demonstrates that many of the treaties and conventions and international human rights instruments that provide jurisdiction for the protection of reproductive health are important but inadequate; they form only a patchwork of indirect efforts to protect people from reproductive health hazards in their workplace. Further international legal research is needed inthis area, comparing and harmonizing local, national and internaitonal laws and codes of practices from corporations regarding reproductive health hazards from occupational exposures.
In addition to further legal research harmonizing international and state laws and analyzing the jurisprudence of pregnancy and of related health laws and laws governing the delivery of primary care at local, national regional and international levels,
The Committee of Experts strongly urges the development of an international instrument
(Such as an ILO Convention, WHO Recommendation, ISO Standard, treaty or other multilateral document) that will directly address these problems, Combined with a strong legislative awareness effort that will educate legislators, members of the international governmental community, regulators, scientists and the general public regarding the urgency and the visible means of preventing foreseeable reproductive health hazards in the workplace and preventing their adverse consequences.
PROPOSED PLAN OF ACTION
Request for Urgent Priority to this matter from the Director General of the WHO and of the ILO and related International Organizations.
Implementation of international consensus statements on reproductive health protection (UN Task Force on Reproductive Health, WHO, ICOH, ILO, Council of Europe=s CDEG etc). Development of agreed terminology on reproductive hazards and reproductive health risks as well as standard definitions for describing and monitoring legislation, policies, services provision and use and reproductive health outcomes (UN Task Force on Reproductive Health, WHO, ICOH, ILO, Council of Europe=s CDEG, WHO Collaborating centers on Occupational Health) for the purposes of the implementation of an enabling International Instrument.
Elaboration of the Guide (or Code of practice) ARisk assessment and risk management for pregnant female workers and health monitoring@ (WHO, ILO, ICOH,).
International Co-ordination of efforts and exchange of experience gained between National centers on reproductive health protection of WHO Collaborating centers on Occupational Health (coordinating meeting with participation of WHO and ILO) and methodological support of the WHO Safe Motherhood Campaign up to 2000 (WHO Collaborating centers on Occupational Health) regarding risk assessment, management and communication, research regarding the interaction of occupational exposures and environmental factors, and related matters of reproductive health of workers.
Preparation of an International Instrument (e.g. ILO Convention supplemented by WHO/ILO_Joint Committee activity or the specialized branches of WHO; or criteria such other documentation as appropriate) on safe motherhood, reproductive health protection for mothers, fathers, and the next generation whose reproductive health may be impaired by the harms we study today, but who will not experience the effects of those harms until they also reach reproductive age; and health promotion of female workers (ad_hoc group).
Recommendation
Therefore the Committee of Experts on Reproductive Health in the Workplace Meeting in Moscow December 11, 1998 hereby Declares and recommends that definitions of occupational health, reproductive health and environmental health impacting on the vitality of the family and the next generation include but are not limited to the effects of dangerous or potentially dangerous exposures to adults in any workplace and shall be considered as a fundamental component of assessing each individual’s health status and well_being.
Therefore this Committee further Recommends that there shall be an international meeting to follow_up this meeting on regular basis, under the auspices of WHO and related international governmental organizations, and that the results of such meetings shall be the production and adoption of an International Instrument for the protection of reproductive health of people at work [21,22].
References
- Adams A (1776) Letter from Abigail Adams to John Adams, Retrieved from Adams Family Papers: An Electronic Archive.
- World Health Organization(2011) Building Health and Equitable Workplaces for Women and Men: A Resource for Employers and Worker Representatives. Geneva: WHO Press.
- Artacoz L, Borrell C, Cortes I, Escriba-Aguir V, Cascant L, (2007) Occupational epidemiology and work related inequalities in health: a gender perspective for two complementary approaches to work and health research. Journal of Epidemiology and Community Health pp. ii39-ii45.
- International Labour Organization. (1983) Convention concerning Occupational Safety and Health and the Working Environment. Retrieved from C155 - Occupational Safety and Health Convention, 1981 (No. 155).
- World Health Organization (2006) Constitution of the World Health Organization, 45th Edition. Retrieved from WHO Governance.
- Feitshans IL (2015) Beijing to Geneva to New York City: the Long Road Towards Protecting Health for All by Increasing STEM Opportunities for Women. The Monitor, a Technical Publication of ASSE’s Industrial Hygiene Practice Specialtypp. 18-24.
- International Labour Organization (2002) C183 - Maternity Protection Convention, 2000 (No. 183). Retrieved from Convention concerning the revision of the Maternity Protection Convention (Revised) 1952
- Macy’s, Inc. (2015) Infant Feeding policy. May’s InSITE Employee Webpage.
- United Nations General Assembly (2012) Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, Anand Grover. New York: United Nations.
- UN Women (2015) Progress of the World’s Women 2015-2016: Transforming Economies, Realizing Rights. Retrieved from UN Women.
- World Health Organization(2011) Building Health and Equitable Workplaces for Women and Men: A Resource for Employers and Worker Representatives. Geneva: WHO Press.
- Centers for Disease Control and Prevention. (2015) Reproductive Health and the Workplace. Retrieved from National Institute for Occupational Safety and Health.
- American College of Obstetricians and Gynecologists. (2013) Exposure to Toxic Environmental Agents. Retrieved from Committee on Health Care for Under Served.
- Shalev C. (1998) Rights to Sexual and Reproductive Health -the ICPD and the Convention on the Elimination of All Forms of Discrimination Against Women. International Conference on Reproductive Health, Mumbai (India), Mumbai: UNDP/ UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction.
- FeitshansIL (1997)Bringing Health to Work.Emalyn Press.
- Occupational Safety and Health Act of 1970 (OSH Act) Section 5 (a) 1 29 USC 651 et seq as discussed in I.L Feitshans Designin an Effective OSHA Compliance Program (Westlaw. com and West/Thomson Reuters 2013)
- Feitshans I, Oliver C (1997) More Than Just a Pretty Program: OSHA Voluntary Protection Programs Improve Compliance by Facing Problems Head-On. 5 Corporate Conduct Quarterlypp. 79: 69-73.
- Feitshans IL (2004) NIOSH Director Launches New MilleniumFrom Mt. Sinai. OEM Rep.
- Hoover M, Armstrong T, Blodgett T, Fleeger A, Logan P, et al (2011) Confirming Our Industrial Hygiene Decision-Making Framework. The Synergist, 10-11.
- United Nations (2015) Transforming our world: the 2030 Agenda for Sustainable Development. Retrieved from UN General Assembly.
- Feitshans IL (2013) Designing An Effective OSHA Compliance Program Westlaw.com and Hard copy West Thomson Reuters 2013.
- Karamessini M, Rubery J (2014) Women and Austerity: The Economic Crisis and the Future for Gender Equality. New York: Routledge.