
World Journal of Radiology and Imaging(WJRI)
ISSN: 2835-2440 | DOI: 10.33140/WJRI


Case Report - (2024) Volume 3, Issue 1
Rare Case Report: Radiologic Findings of Stress Fracture and Avascular Necrosis of the Type 2 Accessory Navicular Bone
2Azerbaijan State Advanced Training Institute for Doctors named after A.Aliyev, Baku, Azerbaijan
Received Date: May 24, 2024 / Accepted Date: Jun 13, 2024 / Published Date: Jun 24, 2024
Copyright: ©Â©2024 Sultan Malakhat, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Bayramov R., Sultan M., Aghamaliyeva A., Gasymova N. (2024). Rare Case Report: Radiologic Findings of Stress Fracture and Avascular Necrosis of the Type 2 Accessory Navicular Bone. World J Radiolo Img, 3(1), 01-04.
Abstract
The accessory navicular bone (ANB) is one of several accessory ossicles of the foot and is considered as a normal anatomic and radiographic variant (1). It occurs due to failure of fusion of a secondary ossification centre within the navicular bone. Fewer than %1 of ANBs are symptomatic, and most of symptomatic ANBs are type II ANBs. Stress fracture of the type II ANB is a rare cause of symptomatic accessory navicular syndrome. We report a case of stress fracture and avascular necrosis of the type II ANB on radiographs and magnetic resonance images in a 23- year- old male.
Keywords
Avascular Necrosis, Stress Fracture, Accessory Navicular bone, MRI, X-Ray, Pain
Abbreviations ANB
accessory navicular boneMRI- magnetic Resonance Imaging
Introduction
The ANB is the second most common ossicle of the foot, with an incidence ranging 4-21% (2). It is more common in females and it may be bilateral 50-90% of the cases (3). The tibialis posterior tendon often inserts with a broad attachment into the ossicle. Medial side foot pain is the most common presenting feature of the ANB. The pain is aggrevated by physical activity. In our case we confirmed a rare cause of symptomatic type 2 ANB- a stress fracture and avascular necrosis of this ANB with characteristic radiographic and magnetic resonance imaging (MRI) findings.
Case presentation:
A 23-year-old male presented to our hospital with compaint of pain in the medial aspect of the foot for 9 month, which was increased with the physical activity. No significant injury was reported at the time. X-ray and MRI was performed. In our case there is stress fracture in the ANB and bone marrow edema due to repetitive microinjury.


Bilateral AP Ankle Radiography (a) and AP Ankle Radiography (b) Shows that there is Stress Fracture (red arrow) in the Type II ANB.


Axial T1W (c) and Sagittal T1W (d) MRI Shows that Hypointense Stress fracture line (blue arrow) and Hypointense Avascular Necrosis in the Type II ANB (red arrow).
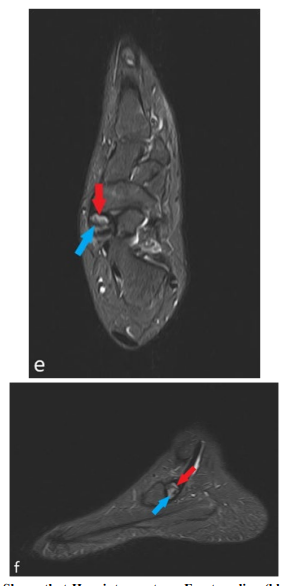
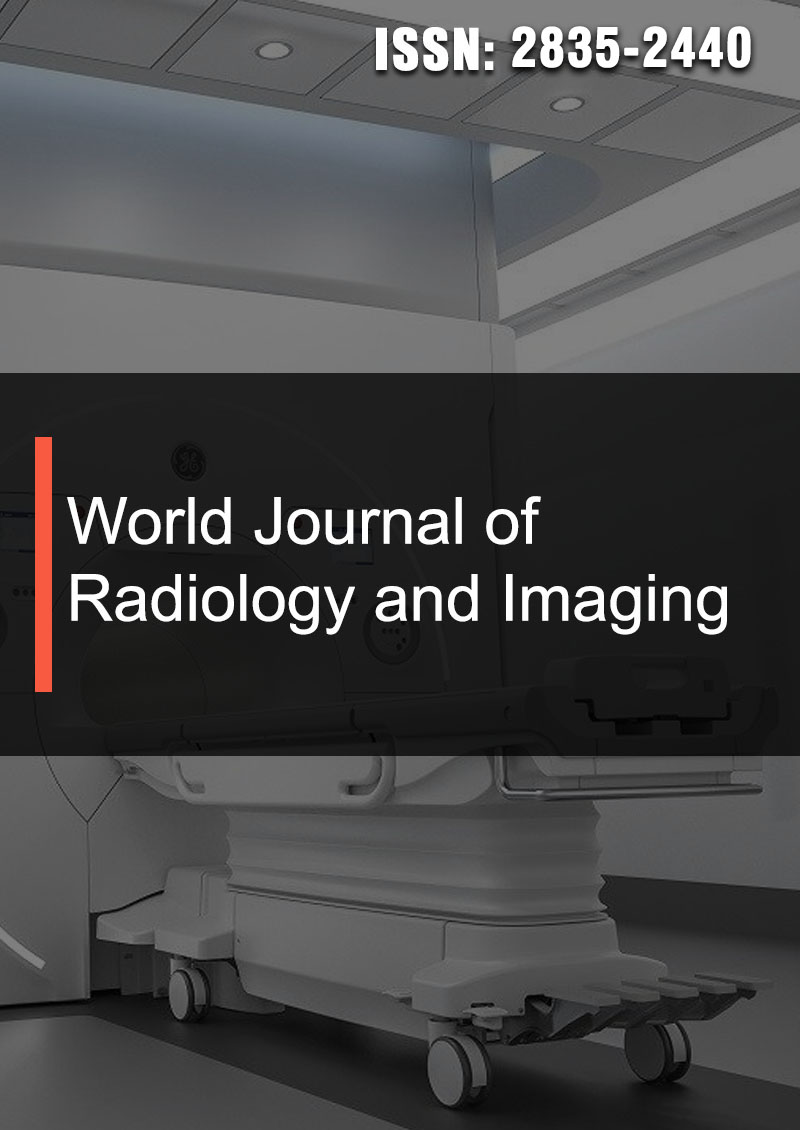
Axial STIR (e) and Sagittal STIR (f) Shows that Hypointense stress Fracture line (blue arrow) and Hyperintense Avascular Necrosis (red arrow)
Discussion
The foot and the ankle are sites of frequent variant anatomy, of which the most commonly seen relate to the accessory ossicles. The most common accessory ossicles in the foot and ankle are the os trigonum and accesory navicular bone. ANB is located adjacent to posteromedial tuberosity of navicular bone. ANBs are classified (Geist classification) into three types based on their morphology and location (4). Type I (os tibiale externum) is 2-3 mm sesamoid bone embedded distal portion of posterior tibial tendon. It accounts for 30 % of ANBs and there is no cartiliginous connection to the navicular tuberosity. This type is usually asymptomatic. Type II ANB (prehallux) is triangular or heart shaped and accounts for 50- 60 % of ANBs. This type is connected to navicular tuberosity by either fibrocartiliginous or hyaline cartilage. Eventually osseous fusion to the navicular tuberosity may take place. Type III ANB is an prominent navicular tuberosity and is considered as fused variant of type II ANB.
Majority of the cases are asymptomatic, but in symptomatic patients type II is the most common and causes medial foot pain (5). Most common clinical symptoms are visible bony prominence on the medial aspect of the foot, erythema and swelling increased by physical activity. The cause of the pain was thought to be repetitive tension and shear stress across the synchondrosis as a result of the pull of posterior tibial tendon (6). Repetitive shearing force can cause osteonecrosis and stress fracture of this ANB. Stress fracture is a rare cause of symtomatic type 2 ANB cases.
Plain radiograph of the foot showed medial navicular eminence of ANB. The ANB appears as a smooth, well corticated density. In the symptomatic type II ANB there is reactive sclerosis which may represent edema or avascular necrosis. MRI is useful in demonstrating both bone marrow and soft tissue edema. The marrow edema represent either osteonecrosis or bone remodelling due to shear forces (7). Tendinosis or thickening of posterior tibial tendon, or tear may also be seen.
Acute pain is usually tretated with oral non-steroidal anti- inflammatory drugs and ice application. For refractory cases surgical management, involving excision of the bone and repair of posterior tibial tendon may be considered.
Conclusion
Most ANBs are detected incidentally on radiographic examinations. In a patient with localized pain in medial foot withou trauma, ANB must be suspected. Presence of ANB should not be disregarded as an incidental radiological variant in a symptomatic patient.
Conflict of Interest: The authors state that there is no conflict interest.
Acknowledgements: The consent form was filled out by the patient.
References
- ES, G. (1914). Supermaumary bone of the foot-a roentgen study of the feet of one hundred normal individuals. Am J Orthop Surg, 12, 403-414.Aparisi Gómez, M. P., Aparisi, F., Bartoloni, A., Ferrando Fons, M. A., Battista, G., Guglielmi, G., & Bazzocchi, A. (2019). Anatomical variation in the ankle and foot: from incidental finding to inductor of pathology. Part I: ankle and hindfoot. Insights into Imaging, 10, 1-13.
- Mosel LD, Kat E, Voyvodic F. Imaging of the symptomatic type II [9] accessory navicular bone. Australas Radiol. 2004; 48(2):267- 71
- Miller TT, Staron RB, Feldman F, Parisien M, Glucksman WJ,Gandolfo LH.
- The symptomatic accessory tarsal navicular bone: assessment with MR imaging. Radiology. 1995; 195(3):849-5
- Vora BMK, Wong BSS. Common accessory ossicles of the foot: imaging features, pitfalls and associated pathology. SingaporeMed J 2018; 59(4):183-189
- SELLA, E. J., LAWSON, J. P., & OGDEN, J. A. (1986). The accessory navicular synchondrosis. Clinical Orthopaedics and Related Research (1976-2007), 209, 280-285
- Pothiawala, S. (2022). Os Navicular Syndrome: A Symptomatic Accessory Ossicle of the Foot. Case Reports in Clinical Practice.