
New Advances in Brain & Critical Care(NABCC)
ISSN: 2771-7887 | DOI: 10.33140/NABCC
Impact Factor: 1.01



Research Article - (2025) Volume 6, Issue 2
Prevalence Rate of Epilepsy among the Patients Attending the General Dhamar Hospital During the Period from 2020-2023
2Assistant Professor of Internal medicine, Faculty of Medicine, Thamar University, Yemen
3M.Sc. of Clinical Pharmacy, Yemen
Received Date: Jan 29, 2025 / Accepted Date: Aug 18, 2025 / Published Date: Sep 03, 2025
Copyright: ©2025 Khalid Saleh, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Saleh, K., Al-Thahbi, M., Al-Zaazaai, A. (2025). Prevalence Rate of Epilepsy among the Patients Attending the General Dhamar Hospital During the Period from 2020-2023. New Adv Brain & Critical Care, 6(2), 01-07.
Abstract
Background: Epilepsy is a prevalent neurological disorder, but data on its characteristics and regional variations are scarce in many parts of the world. This study focuses on Dhamar Governorate, Yemen, a region lacking sufficient information about epilepsy. Understanding the prevalence, age-of-onset patterns, gender distribution, and treatment practices for epilepsy in this area is crucial for improving public health efforts.
Objectives: This study aimed to investigate the prevalence, age-of-onset patterns, gender distribution, and treatment practices for epilepsy in this region.
Methods: This retrospective cross-sectional study analyzed medical records of patients attending General Dhamar Hospital from 2020- 2023. Data on age, gender, residence, epilepsy duration, type, and treatment were collected and analyzed using Statistical Package for Social Sciences (SPSS). Ethical approval was obtained from Thamar University Medical Ethics Committee (TUMEC). Informed consent was waived due to the retrospective nature of the study, but data confidentiality was assured.
Results: The study revealed an age-specific prevalence pattern, with the highest concentration of cases (46.1%) in the 20-40- year age group. Males exhibited a higher prevalence (56%) compared to females (44%). Regarding onset, a two-peak pattern emerged, with childhood (44.9%) and adolescence (24.8%) carrying the highest burdens. Geographically, the prevalence varied significantly, with Dhamar City, Ans, Al-Hada, and Maghirib Ans showing the highest rates. Carbamazepine was the most commonly used medication (74.8%), followed by sodium valproate (19.6%).
Conclusion: Epilepsy is a significant public health concern in Dhamar Governorate, with substantial geographical variations observed. The study highlights potential influences of age, gender, and geographical factors on epilepsy prevalence and treatment patterns. Further investigation is warranted to explore the underlying causes of these disparities and optimize treatment strategies in the region.
Introduction
Epilepsy is a chronic condition affecting the nervous system, where the brain shows an ongoing predisposition to generate seizures. seizure occurring at least 24 hours apart, after a single seizure with a high probability of recurrence, or through recognition of an epilepsy syndrome. It occurs in any age of life and affects all aspect of patent life that goes behind the medical aspect as social, behavioural, economic not only for patients but also for their families [1,2]. 70 million people in the word are affected by epilepsy, (> 80%) of them live in middle and low countries [3,4]. The diagnosis of seizures depends mainly on detailed history taking from patient and available witnesses who observed the events. During the events of epilepsy, the presence of Electroencephalography (EEG) With defined (i.e., abnormal, repetitive, rhythmic activity with a discrete onset and termination) serves as conformation of diagnosis [5]. Even so, the lack of such electrographic findings cannot roll out the diagnosis. Management of epilepsy is almost always multiple intervention, such as treatment of underlying etiology, avoidance of precipitating factors, prevent of recurrent seizures through prophylactic therapy with antiepileptic medications or surgery, and addressing psychological and social issues [6].
According to the latest WHO data (2020), epilepsy-related deaths in Yemen reached 539, accounting for 0.35% of total deaths [7]. The incidence and prevalence of epilepsy vary widely across the world. Studies suggest that prevalence rates in developing countries can be several times higher than those in developed countries [8-11]. Reliable prevalence estimates are crucial for assessing the burden of epilepsy and developing targeted public health interventions. For example, a meta-analysis in India revealed higher incidence rates (60.0 per 100,000 person-years) compared to developed countries, where the age-adjusted incidence ranges from 24–53 per 100,000 person-years [12]. The prevalence and incidence of childhood epilepsy also vary significantly by geographical and socioeconomic factors, emphasizing the need for region- specific strategies to address this burden [13,14]. Confirming the relatively low incidence rates reported in some Asian countries requires rigorous, population-based prospective studies [15]. Despite its devastating impact, epilepsy continues to receive insufficient attention from the public health community. Assessing seizure control and identifying associated factors are essential to improve treatment strategies and enhance patients’ quality of life. Therefore, this study aims to determine the prevalence and associated factors of uncontrolled seizures among people with epilepsy receiving anti-epileptic drug therapy in Comprehensive Specialized Hospitals in Dhamar, Yemen.
Materials & Methods
Study Design and Setting
This retrospective cross-sectional study was conducted at General Dhamar Hospital, located in Dhamar Governorate, Yemen. General Dhamar Hospital is a major referral center serving the city of Dhamar and the surrounding rural areas. The hospital offers a comprehensive range of medical services, including neurology, internal medicine, and emergency care, and accepts patients from across the governorate.
Study Population
The study population consisted of all patients diagnosed with epilepsy who visited General Dhamar Hospital from January 1, 2020, to December 31, 2023. Patients were eligible if their medical records included complete demographic and clinical information relevant to the study variables. Those with incomplete medical records, uncertain diagnoses, or missing essential data were excluded from the analysis.
Data Collection
Data were obtained retrospectively from hospital medical records. Extracted variables included patient age, sex, First-Seizure Onset, place of residence (urban/rural), and treatment regimen. All data were anonymized before analysis to maintain confidentiality.
Statistical Analysis
Data entry and statistical analyses were performed using IBM SPSS Statistics, Version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the study variables. Categorical variables were expressed as frequencies and percentages, while continuous variables were summarized as means ± standard deviations (SD) or medians with interquartile ranges (IQR), depending on data distribution.
Ethical Considerations
The study protocol was reviewed and approved by the Thamar University Medical Ethics -Committee. As this was a retrospective study based on anonymized medical records, the requirement for informed consent was waived; however, patient confidentiality was maintained throughout the study. All procedures adhered to the principles outlined in the Declaration of Helsinki.
Results
General Characteristics of Patient
The total number of epilepsy cases in this study was 661. Table 1 and Figure 1 show the gender-and-age-specific and prevalence of active epilepsy. The peak prevalence of epilepsy was in the 20- 40 age category followed by people less than 20 and 41-60 age groups (46.1%. 33.9%. 15.6% respectively) Overall, there was slightly difference in the prevalence of epilepsy between genders where 56% was male and 44% female.
|
Item |
n |
% |
|
Age |
||
|
Less Than 20 |
224 |
33.9 |
|
20-40 |
305 |
46.1 |
|
41-60 |
103 |
15.6 |
|
More Than 60 |
29 |
4.4 |
|
Sex |
||
|
Male |
370 |
56.0 |
|
Female |
291 |
44.0 |
Table 1: Prevalence of Epilepsy by Age and Gender

Figure 1: Age-Specific Prevalence of Epilepsy by Gender (n=661)
Regarding to Epilepsy Onset
Our findings demonstrate a distinct age-related pattern in first- seizure onset. The highest risk (45.2%) is concentrated within the first decade of life. This is followed by a decrease, with a secondary peak observed in the second decade (24.8%). Subsequently, the incidence of first-time seizures steadily declines throughout adulthood (13.5% in third decade, 8.9% in fourth decade, and 5% to 0.3% from fifth to eighth decades).
|
Item |
n |
% |
|
Frist decade |
299 |
45.2 |
|
2nd decade |
164 |
24.8 |
|
3rd decade |
89 |
13.5 |
|
4th decade |
59 |
8.9 |
|
5th decade |
33 |
5.0 |
|
6th decade |
8 |
1.2 |
|
7th decade |
7 |
1.1 |
|
8th decade |
2 |
.3 |
Table 2: Distribution of Patient with Regard to First-Seizure Onset
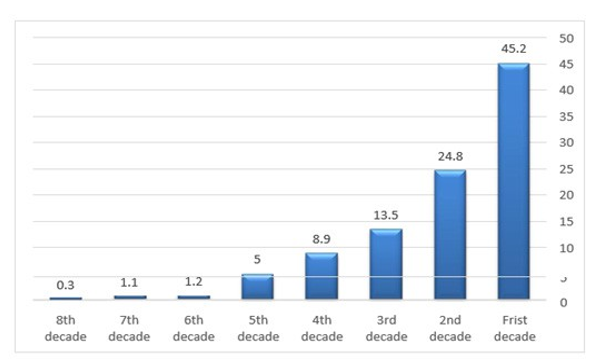
Figure 2: Distribution of Patient with Regard to First-Seizure Onset (n=661)
Prevalence of Epilepsy Across Various Regions
Study revealed a marked variation in the prevalence of epilepsy across regions. A statistically significant variation was observed, with Dhamar City, Ans, Al Hada and Maghirib Ans demonstrating the highest prevalence rates (ranging from 44.6% to 7.3%). Conversely, epilepsy prevalence in Jahran, Mayfa'at Ans, Utmah and Yarim exhibited moderate levels (4.8% - 2.4%), while the lowest prevalence was observed in areas belonging to Al Manar, Wusab Al Ali, Dawran Aness, Wusab As Safil, Ibb, Ar Radmah, An Nadirah, As Saddah, Jabal Ash Sharq (2.0% - 0.2%) see Table 3.
|
Item |
n |
% |
|
Dhamar City |
295 |
44.6 |
|
Ans |
109 |
16.5 |
|
Al Hada |
65 |
9.8 |
|
Maghirib Ans |
48 |
7.3 |
|
Jahran |
32 |
4.8 |
|
Mayfa'at Ans |
26 |
3.9 |
|
Utmah |
18 |
2.7 |
|
Yarim |
16 |
2.4 |
|
Al Manar |
13 |
2.0 |
|
Wusab Al Ali |
12 |
1.8 |
|
Dawran Aness |
8 |
1.2 |
|
Wusab As Safil |
7 |
1.1 |
|
Ibb |
6 |
0.9 |
|
Ar Radmah |
2 |
0.3 |
|
An Nadirah |
2 |
0.3 |
|
As Saddah |
1 |
0.2 |
|
Jabal Ash Sharq |
1 |
0.2 |
Table 3: Prevalence of Epilepsy by Regions
Regarding to Epilepsy Treatment
As shown in [Table 4], In our investigation into epilepsy treatment, carbamazepine stood out as the most frequently employed medication, accounting for a significant 74.8% of cases. Sodium valproate followed at a distant second with 19.6%, highlighting a clear preference for carbamazepine within the studied population Notably, phenobarbital and phenytoin sodium usage trailed considerably behind at 3.2% and 2.4% respectively, suggesting a potential shift towards carbamazepine as the primary therapy.
|
Items |
N |
% |
|
CARBAMEZAPINE |
587 |
74.8 |
|
SODIUM VALPROATE |
154 |
19.6 |
|
PHENOBARBITAL |
25 |
3.2 |
|
PHENYTION SODIUM |
19 |
2.4 |
Table 4: Distribution of Patient with Regard to Epilepsy Treatment
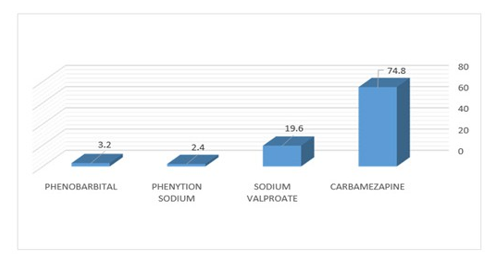
Figure 3: Distribution of Patient with Regard to Epilepsy Treatment
Discussion
This study sheds light on the prevalence and treatment patterns of epilepsy in Dhamar Governorate, a region where such data has been scarce. Age-specific prevalence pattern in this study was slightly similar to that of Finland, where the prevalence of epilepsy increased until the age of 40-50 years, then it declined as the people become older [16]. In Arab countries the prevalence of epilepsy is bimodal in distribution with a first peak in children and another smaller peak in the elderly, which is align with international studies [17]. In comparison to estimates from other parts of the world, a study in rural Zambia Revealed children aged 5-15 years and people over 65 years had the highest rates of prevalence and in Congo the younger individuals were in the peak suggesting potential variations in risk factors or healthcare access across these regions [18,19]. In China. A higher prevalence of epilepsy was among young male and rural [20]. Surprisingly, a systematic review and meta-analysis of international studies conducted that the prevalence of epilepsy is not affected by age group, sex, or study quality [21]. Age-specific prevalence pattern mismatch might be explained by the differences in risk factors of epilepsy in different geographical areas [17].
The study also highlights a slight gender disparity, with a higher prevalence among males (56%) compared to females (44%). This aligns with the findings of seven previous studies in arab region about gender prevalence. Which showed a slightly higher prevalence in males than in females [17]. Male excess might be due to Head trauma as it is one of the etiological factors of epilepsy and is well-known more frequent among male [22- 24]. Possibly that epilepsy in women was under-reported in this study due to various social and cultural factors, one of them is misconceptions about epilepsy in this region, as people consider it a psychiatric illness caused by the devil, and epileptic women will not get married, which in turn led females to hide the diagnosis [25,26]. However, research from Guatemala suggests a possible higher prevalence among females, prompting further investigation into potential gender-based disparities in epilepsy presentation or healthcare access across different countries [27]. Regarding to onset of epilepsy. Our study highlights a two-peak pattern in first-time seizure risk. Childhood (first decade of life) carries the highest burden (45.2%), potentially due to factors like ongoing brain development, genetic predisposition, or childhood illnesses. While the risk lessens after this initial peak. In previous published studies the incidence and prevalence of first-time seizure were difficult to assess due to uncertainty to account for precisely for the first seizure. Some seizure types without impairment of consciousness such absences, myoclonus, or focal seizures are usually not perceived as epileptic events. Other challenging factor is the Differential diagnosis. For example, in the epilepsy clinic pf pediatric, first unprovoked seizures were missed in 30% and other events were classified as epileptic in 25% [28,29].
A secondary peak persists also in adolescence by (24.8%). This aligns with as research published in Pakistan in which the onset of first-time seizures is seen among those before age of 18 years (74.3%) [30]. Thereafter, the risk steadily declines throughout adulthood. This age-related trend suggests potential vulnerability windows for first-time seizures, warranting further investigation into the specific causes during these developmental stages. The striking geographical heterogeneity in epilepsy prevalence was also identified in our study. Regions including Dhamar City, Ans, Al-Hada, and Maghirib Ans exhibited the highest prevalence rates, ranging from 44.6% to 7.3%. These findings highlight epilepsy as a significant public health concern in these specific regions. Conversely, epilepsy prevalence in Mayfa'at Ans, Jahran, Utmah, and Yarim demonstrated a moderate range (3.9%-2.4%). Notably, the lowest prevalence was observed in areas belonging to Dawran Aness District, Wusab As Safil District, Ibb Governorate, Ar Radmah, A Nadirah, and As Saddah regions. This observed disparity warrants further investigation, particularly within the high-prevalence regions. Potential contributing factors may include differential environmental exposures, such as toxins or infectious agents, across Yemeni geographical areas. Additionally, variations in the genetic makeup of Yemeni populations might influence susceptibility. Furthermore, healthcare access and reporting practices cannot be discounted. Limited access to neurological specialists or cultural stigma surrounding epilepsy could lead to underdiagnosis in some regions. Regarding Treatment Patterns the decision to start anti-epileptic drug should be individualized, but must be taking into account after 2 unprovoked attacks of seizures or after 1 unprovoked attack during sleep and/or evidence of epileptiform activity on an electroencephalogram and/or in the presence of a structural lesion on the brain magnetic resonance imaging (MRI). The selection of appropriate drug depends on the epilepsy type, epilepsy syndrome and the adverse effects of the drug [31].
This study explores the most commonly used medications for managing epilepsy at Dhamar General Hospital. Carbamazepine reigns supreme at 74.8%, indicating its potential effectiveness as a first-line treatment for this patient population. This medication has a well-established track record for managing various seizure types, and its dominance suggests affordability, tolerability, and efficacy in the local context. In contrast, a review about epilepsy medication conduct that, the first-line therapy for focal epilepsy are oxcarbazepine and lamotrigine, while levetiracetam can be also considered if there is no history of psychiatric disorder [31]. The same review revealed that ASDs with cytochrome P450 enzyme-inducing properties (eg, carbamazepine, phenytoin) may worsen the condition of patient complaining of coronary and cerebrovascular disease indirectly by causing hyperlipidaemia and accelerating the metabolism of concomitant drugs used for their treatment. They may also cause osteopenia and osteoporosis [31]. Sodium valproate follows closely behind at nearly 20%, offering another treatment option for patients. Interestingly, the usage of phenobarbital (3.2%) and phenytoin sodium (2.4%) is significantly lower. This suggests these medications might be reserved for specific cases, such as patients who are intolerant of carbamazepine or valproate, or for particular seizure types that respond better to these medications. This pattern aligns with findings in Turkey, where similar treatment hierarchies have been observed [32]. However, this contrasts with a study in Cameroon, where phenobarbital was the most commonly used drug [33]. The updates on Antiseizure Medications 2025 revealed that the newer antiseizure medications have undergone comparative trials conducting that the efficacy and tolerability at least equal to or better than older antiseizure medications as first-line therapy for focal epilepsy.
These medications include lamotrigine, oxcarbazepine, levetiracetam, topiramate, zonisamide, and lacosamide. This variation highlights potential differences in healthcare practices, medication availability, or treatment guidelines across these regions. Further research may explore the reasons behind the observed medication choices. Are there cost considerations that favor carbamazepine? Are there limitations in the availability of other medications? Additionally, investigating treatment outcomes for patients on these various medications would provide a more comprehensive understanding of how epilepsy is managed and its effectiveness in Dhamar Governorate. By delving deeper into these aspects, researchers can gain valuable insights into optimizing epilepsy treatment strategies in this region. Further research could explore the reasons behind the observed medication choices. Are there cost considerations that favor carbamazepine? Are there limitations in the availability of other medications? Additionally, investigating treatment outcomes for patients on these various medications would provide a more comprehensive understanding of how epilepsy is managed and its effectiveness in Dhamar Governorate. By delving deeper into these aspects, researchers can gain valuable insights into optimizing epilepsy treatment strategies in this region.
Conclusion and Recommendation
Conclusion
This study provides valuable insights into the prevalence, treatment patterns of epilepsy in Dhamar Governorate, Yemen. The findings reveal an age-specific prevalence pattern with peaks in childhood and young adulthood, similar to observations in Finland, and Arab countries. A slight male predominance aligns with trends in developing countries. The study also highlights a concerning geographical heterogeneity in epilepsy prevalence, with some regions exhibiting significantly higher rates than others. Regarding treatment patterns, carbamazepine is the dominant medication used at Dhamar General Hospital, potentially due to affordability, tolerability, and efficacy. This pattern aligns with observations in Turkey, but contrasts with studies in Cameroon.
Recommendations
Further research is recommended to explore the following:
• Investigate the reasons behind the observed geographical variations in epilepsy prevalence. Potential contributing factors may include environmental exposures, genetic makeup, or healthcare access disparities.
• Conduct studies to assess treatment outcomes for patients on various medications (carbamazepine, sodium valproate, phenobarbital, phenytoin sodium) to gain a more comprehensive understanding of treatment effectiveness in Dhamar Governorate.
• Explore cost considerations and availability of different epilepsy medications to understand the factors influencing treatment choices
Declarations
Data Availability
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request.
Acknowledgements
We would like to express our sincere gratitude to General Dhamar Hospital for their generous support, cooperation, and valuable contributions that made this study possible. Their assistance and collaboration were essential to the successful completion of our work.
Authors Contribution
Prof. Khaled Saleh contributed to the conception and design of the study, supervised the research process, and provided critical revisions to the manuscript. Prof. Mohammed Al-Thahbi contributed to data analysis and interpretation, assisted in drafting the manuscript, and reviewed it for important intellectual content. Both authors read and approved the final manuscript.
References
- Camfield, P., & Camfield, C. (2015). Incidence, prevalence and aetiology of seizures and epilepsy in children. Epileptic disorders, 17(2), 117-123.
- Cowan, L. D. (2002). The epidemiology of the epilepsies in children. Mental retardation and developmental disabilities research reviews, 8(3), 171-181.
- Kakoozaâ?Mwesige, A., Ndyomugyenyi, D., Pariyo, G., Peterson, S. S., Waiswa, P. M., Galiwango, E., ... & Noh, J. (2017). Adverse perinatal events, treatment gap, and positive family history linked to the high burden of active convulsive epilepsy in Uganda: a populationâ?based study. Epilepsia Open, 2(2), 188-198.
- Guerreiro, C. A. (2016). Epilepsy: Is there hope?. IndianJournal of Medical Research, 144(5), 657-660.
- Vedanthan, P. K., Nelson, H. S., Agashe, S. N., Mahesh, P. A., & Katial, R. (Eds.). (2014). Textbook of Allergy for the Clinician. CRC press.
- Dan Longo, Anthony Fauci, Dennis Kasper, Stephen Hauser,J. Larry Jameson, Joseph Loscalzo, et al. Harrison’s principlesof internal medicine. Vol. 22. 2025.
- World Health Organization. (2022). Improving the lives of people with epilepsy: a technical brief. World Health Organization.
- Sridharan, R., & Murthy, B. N. (1999). Prevalence and patternof epilepsy in India. Epilepsia, 40(5), 631-636.
- Beghi, E. (2020). The epidemiology of epilepsy. Neuroepidemiology, 54(2), 185-191.
- World Health Organization. Epilepsy. World Health Organization . 2024 Feb 7.
- Feigin, V. L., Vos, T., Nair, B. S., Hay, S. I., Abate, Y. H., Abd Al Magied, A. H., ... & Gadanya, M. A. (2025). Global, regional, and national burden of epilepsy, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet Public Health, 10(3), e203-e227.
- Amudhan, S., Gururaj, G., & Satishchandra, P. (2015). Epilepsy in India I: Epidemiology and public health. Annals of Indian Academy of Neurology, 18(3), 263-277.
- Darabi, B., Shokri, M., & Rahmatian, A. (2023). Prevalence of Epilepsy among Iranian Children and Adolescents: A Systematic Review and Meta-Analysis. Journal of Pediatric Perspectives, 11(5), 17807-17817.
- Lahmini, W., Gyamfi, S. O., & Bourrous, M. (2023). Survey on the management of childhood epilepsy among general practitioners in the area of Marrakech. BMC pediatrics, 23(1), 159.
- Mac, T. L., Tran, D. S., Quet, F., Odermatt, P., Preux, P. M., & Tan, C. T. (2007). Epidemiology, aetiology, and clinical management of epilepsy in Asia: a systematic review. The Lancet Neurology, 6(6), 533-543.
- Keränen, T., Riekkinen, P. J., & Sillanpaa, M. (1989). Incidence and prevalence of epilepsy in adults in eastern Finland. Epilepsia, 30(4), 413-421.
- Idris, A., Alabdaljabar, M. S., Almiro, A., Alsuraimi, A., Dawalibi, A., Abduljawad, S., & AlKhateeb, M. (2021). Prevalence, incidence, and risk factors of epilepsy in arab countries: A systematic review. Seizure, 92, 40-50.
- Birbeck, G. L., & Kalichi, E. M. (2004). Epilepsy prevalence in rural Zambia: a doorâ?toâ?door survey. Tropical Medicine & International Health, 9(1), 92-95.
- Colebunders, R., Mandro, M., Mokili, J. L., Mucinya, G., Mambandu, G., Pfarr, K., ... & Laudisoit, A. (2016). Risk factors for epilepsy in Bas-Uélé Province, Democratic Republic of the Congo: A case–control study. International Journal of Infectious Diseases, 49, 1-8.
- Gu, L., Liang, B., Chen, Q., Long, J., Xie, J., Wu, G., ... &Su, L. (2013). Prevalence of epilepsy in the People's Republic of China: a systematic review. Epilepsy research, 105(1-2), 195-205.
- Fiest, K. M., Sauro, K. M., Wiebe, S., Patten, S. B., Kwon,C. S., Dykeman, J., ... & Jetté, N. (2017). Prevalence and incidence of epilepsy: a systematic review and meta-analysis of international studies. Neurology, 88(3), 296-303.
- Hauser, W. A., & Kurland, L. T. (1975). The epidemiology of epilepsy in Rochester, Minnesota, 1935 through 1967. Epilepsia, 16(1), 1-66.
- Bharucha, N. E., Bharucha, E. P., Bharucha, A. E., Bhise, A. V., & Schoenberg, B. S. (1988). Prevalence of epilepsy in the Parsi community of Bombay. Epilepsia, 29(2), 111-115.
- Annegers, J. F., Grabow, J. D., Groover, R. V., Laws Jr, E. R., Elveback, L. R., & Kurland, L. T. (1980). Seizures after head trauma: a population study. Neurology, 30(7), 683-683.
- Al Rajeh, S., Awada, A., Bademosi, O., & Ogunniyi, A. (2001). The prevalence of epilepsy and other seizure disorders in an Arab population: a community-based study. Seizure, 10(6), 410-414.
- Jallon P. Epilepsy in Developing Countries. Epilepsia. 1997 Oct 3;38(10):1143–51.
- Garcia-Noval, J., Moreno, E., Mata, F. D., De Alfaro,H. S., Fletes, C., Craig, P. S., & Allan, J. C. (2001). An epidemiological study of epilepsy and epileptic seizures in two rural Guatemalan communities. Annals of Tropical Medicine & Parasitology, 95(2), 167-175.
- Jiménez-Villegas, M. J., Lozano-García, L., & Carrizosa- Moog, J. (2021). Update on first unprovoked seizure in children and adults: a narrative review. Seizure, 90, 28-33.
- Hamiwka, L. D., Singh, N., Niosi, J., & Wirrell, E. C. (2007). Diagnostic inaccuracy in children referred with “first seizure”: role for a first seizure clinic. Epilepsia, 48(6), 1062-1066.
- Khatri, I. A., Iannaccone, S. T., Ilyas, M. S., Abdullah, M., & Saleem, S. (2003). Epidemiology of epilepsy in Pakistan: review of literature. JPMA. The Journal of the Pakistan Medical Association, 53(12), 594-597.
- Kanner, A. M., & Bicchi, M. M. (2022). Antiseizure medications for adults with epilepsy: a review. Jama, 327(13), 1269-1281.
- ÇaliÅ?ir, N., Bora, I., Irgil, E., & Boz, M. (2006). Prevalence of epilepsy in Bursa city center, an urban area of Turkey. Epilepsia, 47(10), 1691-1699.
- Angwafor, S. A., Bell, G. S., Ngarka, L., Otte, W., Tabah,E. N., Nfor, L. N., ... & Sander, J. W. (2021). Incidence and prevalence of epilepsy and associated factors in a health district in North-West Cameroon: a population survey. Epilepsy & Behavior, 121, 108048.