
Journal of Ophthalmology & Clinical Research(JOCR)
ISSN: 2573-9573 | DOI: 10.33140/JOCR
Impact Factor: 1.3


Research Article - (2025) Volume 9, Issue 1
Prevalence, Patterns, and Risk Factors of Retinopathy of Prematurity in a Tertiary Mult Speciality Hospital in Western Odisha
2Consultant, Department of Neonatology Vikash multi speciality Hospital Bargah, Odisha, India
Received Date: Dec 04, 2024 / Accepted Date: Jan 08, 2025 / Published Date: Jan 13, 2025
Copyright: ©©2025 Sushil Kumar Kar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Kar, S. K., Satapathy, A. K. (2025). Prevalence, Patterns, and Risk Factors of Retinopathy of Prematurity in a Tertiary Mult Speciality Hospital in Western Odisha. J Ophthalmol Clin Res, 9(1), 01-06.
Abstract
Retinopathy of Prematurity (ROP) is a significant concern in premature infants, with varying prevalence rates and associated risk factors. The stages of ROP range from stage 1 (demarcation line) to stage 5 (total retinal detachment). Aggressive posterior ROP is a severe variant characterized by rapid progression and high risk of blindness if not promptly treated. We assessed infants born between 27 weeks to 40 weeks of gestation having birth weights under 2500 g for ROP prevalence, patterns and risk factors. Total 600 eyes of 300 neonates were examined during the study period. Out of them 278 neonates underwent ROP screening based on inclusion criteria.
In present study, 27.7% of neonates screened had ROP were found positive for ROP. The mean gestational age (GA) of infants diagnosed with ROP had 31 weeks and 3 days. The incidence of ROP was maximum (59.74%) at 28+1 - 32 weeks. A significant association of ROP with gestational age (<34 weeks) and birth weight (<2000gm) was noted. Stage 1 and Stage 2 ROP was exhibited by 27.92% and 36.36% neonates respectively. Neonates participated in study did not show Stage 4 and Stage 5 ROP. Presence of anemia, Intraventricular hemorrhage, packed red blood cell transfusion, apnea, respiratory distress, and two or more risk factors were also major contributor of ROP.
Keywords
Retinopathy of Prematurity; Stages of Rop, Risk Factors, Anemia, Intraventricular Haemorrhage
Introduction
Retinopathy of Prematurity (ROP) is a significant concern in premature infants, with varying prevalence rates and associated risk factors [1]. ROP is a vaso-proliferative condition primarily affecting premature infants, leading to preventable blindness [2]. This condition involves the abnormal proliferation of blood vessels in the retina, which, if not addressed, can result in vision loss or blindness. The stages of ROP range from stage 1 (demarcation line) to stage 5 (total retinal detachment) [3]. Aggressive posterior ROP is a severe variant characterized by rapid progression and high risk of blindness if not promptly treated [4]. The prevalence of retinopathy of prematurity varies depending on the gestational age and birth weight of the infants [2]. Several risk factors have been identified for the development of retinopathy of prematurity, including low gestational age, low birth weight, prolonged oxygen therapy, respiratory distress syndrome, multiple births, and the presence of other medical conditions such as sepsis or anemia [5]. ROP is indeed a complex condition that primarily affects premature infants, particularly those born with very low birth weights and underdeveloped retinas. The multifactorial nature of ROP results from a mix of genetic predisposition and environmental influences, making it difficult to identify precise causes or accurately forecast its advancement [7].
Oxygen is crucial in ROP, just as it is in other retinopathies such as proliferative diabetic retinopathy and sickle cell retinopathy. Birth weight and gestational age are inversely correlated with the incidence of ROP.8 Retinal vasoconstriction may result from elevated oxygen concentrations. It has been noted that oxygen saturation is a variable that, if maintained at a low level, can impede the progression of ROP. Additionally, studies have shown that certain genetic factors and maternal characteristics, such as smoking during pregnancy or preeclampsia, may also contribute to the risk of retinopathy of prematurity [8,9]. Premature newborn survival rates have improved as a result of recent advancements in neonatal care during the past ten years. As a result, ROP prevalence is increasing. Low birth weight, low gestational age, and increased oxygen supplementation postpartum are risk factors for ROP [9]. Infants born before 32 weeks gestation or weighing 1500 grams should be screened with proper follow-up based on risk factors [10,11]. ROP affects around 50,000 children worldwide, with increasing incidence in low-income nations. Research conducted in western countries reveals that the prevalence of ROP varies from 21 to 65.8% [12,13]. The frequency of ROP has grown in babies weighing less than 900 grams at birth, and it is now a major preventable cause of newborn blindness [13]. As much as 80–100% of neonates born at fewer than 25 weeks are affected [14].
Current prevalence rates of Retinopathy of Prematurity (ROP) vary from 9.3% in Switzerland to 64.1% in Portugal and 39.5% in Norway, with different screening guidelines used across Europe. The prevalence of Retinopathy of Prematurity (ROP) in India varies across different studies. In Karnataka, a study reported a prevalence of 17.41% among preterm babies [15]. Another study conducted in Western Maharashtra found an incidence of 13.50% for ROP [16]. Additionally, a study in Rajkot reported an incidence of 8% for ROP in low birth weight and preterm neonates [10]. Furthermore, a study in Aligarh, Uttar Pradesh, identified a prevalence of 17.68% for ROP among premature babies [12]. This research aims to investigate the occurrence, patterns, and potential risk factors linked to Retinopathy of Prematurity (ROP) within a tertiary multispecialty hospital situated in western Odisha. Additionally, our analysis seeks to understand their impact on both the development and progression of ROP.
Material and Method
Study Design
This was a hospital-based retrospective observational study on 300 neonates attending Vikash Multi Speciality Hospital,Bargarh, Odisha between 1-1-2021 to 1-1-2024. The study included 243 Inborn and 57 referral patients, referred by paediatricians from the same district. The informed consent form was collected from patients after ethical clearance of the project from the institutional ethical committee.
Study Population
Included neonates with gestational age between 26-40 weeks and birth weight more than 750 g. The infants were first examined at 2 to 6 weeks after birth.
Inclusion Criteria
Included in the study were neonates with birth weights greater than or equal to 750 grams and gestational ages exceeding 26 weeks, provided they exhibited additional risk factors such as respiratory distress, requirement for mechanical ventilation, septicemia, blood transfusion, or apnea. Recorded data encompassed the infant's name, gender, gestational age at birth, birth weight, age, and weight at the time of screening, along with risk factors such as respiratory distress syndrome (RDS), Patent Ductus Arteriosus (PDS) septicemia, hypoxia, blood transfusion, multiple gestations, Intraventricular hemorrhage and apnea [17-19].
Exclusion Criteria
Excluding neonates with ocular disorders and those not followed up till complete retinal vascularization could introduce selection bias.
Statistical Analysis
The statistical analysis focused on specific risk factors like gestational age and birth weight, potentially overlooking other relevant variables influencing ROP development. Entered all study data into a performa and MS Excel sheet for cleaning and verification. Analyzed categorical variables using Chi-square or Fischer exact test and continuous variables using t-tests in SPSS software.
Results
This study was conducted from January 2021 to January 2024. A total of 600 eyes of 300 neonates were registered during the study period. Out of them, 293 neonates underwent ROP screening after finding them suitable based on inclusion criteria. Of these infants, 24.25% received their initial screening in the NICU before discharge. A total of 293 cases were screened, with 40 (13.6%) cases diagnosed with ROP. Among total 40 ROP cases, 22 were inborn patients and 18 were referred cases. The mean birth weight of all screened infants was 1.45 kg, contrasting with 1.27 kg among infants with ROP. These results underscore the importance of early gestational age and lower birth weight as significant risk factors that increase the likelihood of ROP in premature infants associated with the development of ROP in preterm infants, emphasizing the need for targeted screening and intervention strategies to address this sight-threatening condition effectively (Table 1). On comparing ROP-positive patients and total screened patients, the maximum patients belonged to GA 28week-32weeks and birth weight range of 1kg- 1.5kg.
Gestational age
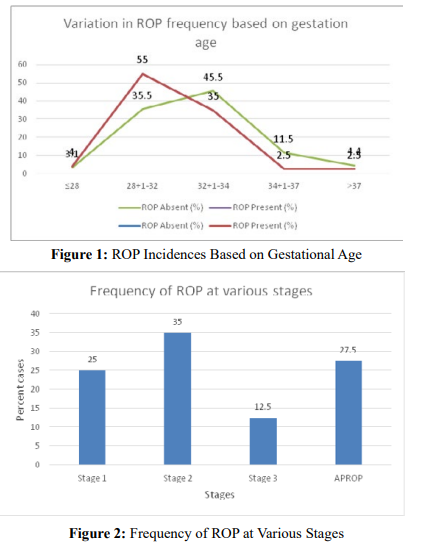
The average gestational age of patients included was 32 weeks and 1 day, ranging from 28 weeks to 40 weeks, however, it was 31 weeks and 3 days for ROP-positive patients (Table 1). The research findings indicate a notable correlation between gestational age and the prevalence of retinopathy of prematurity (ROP). Among infants born at or before 28 weeks of gestation, ROP was observed in 4% of cases, while in those born between 28 - 32 weeks, the prevalence significantly increased to 55%. Conversely, as gestational age advanced (32+1 weeks - 34 weeks), a significant decrease in ROP prevalence (35%) was observed among ROP cases. However, 45.5% of all ROP absent cases belonged to this category. Infants born after 34 weeks of gestation exhibited 5% of total ROP prevalence whereas 16% had no ROP (Figure 2).
Stages of ROP
The stages of ROP classify its severity based on the extent of abnormal blood vessel growth. In Zone I, which is the innermost region of the retina, Stage 1 and 3 ROP was noted in single cases however, stage 2, characterized by a line of abnormal vessels, was more common. Zone II, extending from the edge of Zone I to the ora serrata showed maximum frequency of ROP cases. Stage 3 marks the presence of abnormal vessels extending into the vitreous was noted in 12.99% of cases. Stages 1 and 2 of zone II were most commonly seen in patients with 25.97% and 31.17% frequency. Zone III, the least severe region, showed lowest frequencies of ROP cases, often with milder manifestations (Table 2). On comparing stage-wise cases stages 4 and 5 were not observed in the provided data cases either at the time of screening or during follow-up. The highest overall percentage of ROP cases belonged to stage 2 (35%) followed by AROP cases (27.5%). APROP was observed in 45 eyes (29.22%), characterized by indistinct ROP stages, shunting, vascular looping, and flat neovascular fronds in Zone I and posterior Zone II, along with vessel dilation and tortuosity in all quadrants. Stage 3 cases were noted lesser than stage 1 cases (Figure 2).
|
Variable |
Results in all the screened infants, n (%) |
Results in infants with ROP, n (%) |
|
Total number of cases (n) |
293 |
40 (13.65) |
|
Mean GA (weeks+days) |
32±1 |
31±3 |
|
Mean birth weight (kg) |
1.45±1 |
1.27±1 |
|
Infants in different GA categories (weeks+ days) |
||
|
≤28 |
10 (3.4) |
2 (4.0) |
|
28+1-32 |
114 (38.9) |
22 (55.0) |
|
32+1-34 |
131 (44.74) |
14 (35.0) |
|
34+1-37 |
28 (9.6) |
1 (2.5) |
|
>37 |
10 (3.4) |
1 (2.5) |
|
Infants in various birth weight categories (kg) |
||
|
<1 |
18 (6.14) |
3 (7.5) |
|
1-1.5 |
170 (58.02) |
24 (60.0) |
|
1.5-2 |
85 (29.0) |
11 (27.5) |
|
2-2.5 |
20 (6.83) |
2 (4) |
Table 1: Characteristics of Infants Screened for Retinopathy of Prematurity
Risk Factor Analysis
We analyzed to IDENTIFY risk factors associated with ROP development. Our findings revealed a positive correlation between ROP and several factors, including lower GA (<34 weeks), anemia, Intraventricular hemorrhage, packed red blood cell transfusion, apnea, respiratory distress, and the presence of two or more risk factors. However, septicemia, multiple gestation, hypoxia, and Patent Ductus Arteriosus did not show a statistically significant association with ROP development. Interestingly, birth weight did not demonstrate a significant association with ROP in our study. Among the screened babies, 93% had a birth weight of less than 2 kg. However, among ROP patients 87.5% of babies with a birth weight less than 2 kg (Table 3).
|
Stages of ROP |
Zone I |
Zone 2 |
Zone 3 |
|||
|
Frequency |
Percentage |
Frequency |
Percentage |
Frequency |
Percentage |
|
|
Stage 1 |
1 |
0.65 |
8 |
25.97 |
1 |
1.30 |
|
Stage 2 |
2 |
2.6 |
11 |
31.17 |
1 |
2.60 |
|
Stage 3 |
1 |
1.95 |
3 |
12.99 |
1 |
0.65 |
|
Stage 4 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Stage 5 |
0 |
0 |
0 |
0 |
0 |
0 |
Table 2: Distribution of Stages of ROP among Patients
We analyzed to identify risk factors associated with ROP development. Our findings revealed a positive correlation between ROP and several factors, including lower GA (<34 weeks), anemia, Intraventricular hemorrhage, packed red blood cell transfusion, apnea, respiratory distress, and the presence of two or more risk factors. However, septicemia, mechanical ventilation, multiple gestation, hypoxia, and Patent Ductus Arteriosus did not show a statistically significant association with ROP development. Among the screened babies, 87.5% of ROP present cases and 76.14% of ROP absent cases had a birth weight of less than 2 kg. However, among ROP patients 87.5% of babies had a birth weight less than 2 kg (Table 3).
|
Risk Factor |
ROP Present (%) n=40 |
ROP absent (%) n= 253 (%) |
χ2 |
df |
P |
|
Birth weight <2 kg |
35.0 (87.5%) |
223.0 (76.14%) |
4.8033 |
1 |
0.051 |
|
GA <34 weeks |
38.0 (95.0%) |
127.0 (50.20%) |
1.370 |
1 |
0.001 |
|
Multiple gestations |
2.0 (5.0%) |
15.0 (5.93%) |
0.0186 |
1 |
0.89 |
|
Intraventricular hemorrhage |
7.0 (17.5%) |
12.0 (4.74%) |
6.974 |
1 |
0.008 |
|
Sepsis |
16.0 (40.0%) |
47.0 (18.58%) |
0.0026 |
1 |
0.04 |
|
Transfusion |
17.0 (42.5%) |
31.0 (12.25%) |
6.803 |
1 |
0.0091 |
|
Mechanical ventilation |
4.0 (10.0%) |
12.0 (4.74%) |
0.71 |
1 |
0.4 |
|
Patent Ductus Arteriosus |
2.0 (5.0%) |
6.0 (2.37%) |
0.04 |
1 |
0.83 |
|
Anemia |
6.0 (15.0%) |
16.0 (6.32%) |
9.392 |
1 |
0.0021 |
|
Hypoxia |
2.0 (5.0%) |
4.0 (1.58%) |
0.048 |
1 |
0.83 |
|
Respiratory distress |
10.0 (25.0%) |
49.0 (19.37%) |
13.0804 |
1 |
0.0003 |
|
Multiple risk factors |
7.0 (17.5%) |
84.0 (33.23% |
10.8243 |
1 |
0.001 |
Table 3: The Incidence of Risk Factors among Infants with and without ROP
Discussion
Our research was conducted at a tertiary care hospital in West Odisha. It revealed the prevalence and patterns of ROP within our facility. Additionally, it investigated the associations between various risk factors and the development of ROP. This study indicates a 13.65% incidence rate of ROP occurrence. Previous studies indicated that the overall incidence of ROP ranges from 13.5% to 32.3%, with severe ROP affecting up to 17.7% of infants [20]. We also noted aggressive posterior ROP (APROP) as a major pattern of ROP. Notably, it has been observed in a significant percentage of cases in India, ranging from 16% to 28% over the years, which is higher than our results [21,16]. Risk factors associated with the development of ROP in Indian infants include low gestational age, low birth weight, presence of apnea, intraventricular hemorrhage (IVH), anemia, and respiratory distress syndrome (RDS), which is common among ROP cases [22]. The increasing prevalence of ROP in India is attributed to factors such as a high number of preterm births, suboptimal neonatal care, lack of awareness, and inadequate ophthalmic care in neonatal units [23]. Stage I ROP is considered an early stage of retinopathy of prematurity (ROP) [24]. In the context of ROP, Stage I ROP is characterized by demarcation lines without a ridge [25]. On the other hand, Stage II ROP represents a more advanced stage of the disease, involving the presence of a ridge and Stage V is the most advanced stage. In the present study, 25% exhibited Stage 1 at various zones and 35% displayed Stage II ROP across the zones.
Neonates who participated in the study did not show Stage IV and V ROP, also known as advanced ROP, which are difficult to manage without timely interventions [26]. Early diagnosis and intervention are crucial for preserving vision in partial detachments not involving the fovea, making stage IV ROP a critical therapeutic window [1,9]. Innovative technologies like automatic ROP construction methods are also being developed to enhance efficiency and generality in ROP management. Overall, a multidisciplinary approach combining surgical expertise, pharmacological interventions, and technological advancements is key to addressing the complexities of advanced ROP [3,6,7]. According to Prasad et al., (2023) and Abdul et al., (2022) hyperoxemia, hypoxia, extended respiratory assistance, clinical signs of maternal chorioamnionitis, neonatal sepsis, platelet transfusions, and insufficient postnatal weight gain are frequently encountered risk factors associated with severe cases of retinopathy of prematurity (ROP) [18,27]. Infants diagnosed with medical or surgical necrotizing enterocolitis face heightened susceptibility to ROP, including severe forms of the condition. Our study also noted these risk factors with the dominance of neonatal sepsis and platelet transfusions.
References
- Azad, R., Gilbert, C., Gangwe, A. B., Zhao, P., Wu, W. C., Sarbajna, P., & Vinekar, A. (2020). Retinopathy of prematurity: how to prevent the third epidemics in developing countries. Asia-Pacific Journal of Ophthalmology, 9(5), 440-448.
- Balamurali, M., Balakrishnan, N., Devimeenakshi, K., & Naaraayan, S. A. (2023). Incidence and risk factors of Retinopathy of Prematurity–a prospective observational study. Perinatal Journal, 31(2), 111-117.
- Makogon, S. I., Gorbacheva, N. V., & Khlopkova, Y. S. (2022). Antenatal risk factors for retinopathy of premature. Russian Pediatric Ophthalmology, 17(4), 49-59.
- Fu, Z., Nilsson, A. K., Hellstrom, A., & Smith, L. E. (2022). Retinopathy of prematurity: Metabolic risk factors. Elife, 11, e80550.
- Fu, Z., Nilsson, A. K., Hellstrom, A., & Smith, L. E. (2022). Retinopathy of prematurity: Metabolic risk factors. Elife, 11, e80550.
- de las Rivas Ramírez, N., Luque Aranda, G., Rius Díaz, F., Pérez Frías, F. J., & Sánchez Tamayo, T. (2022). Risk factors associated with Retinopathy of Prematurity development and progression. Scientific Reports, 12(1), 21977.
- Prasad, M., Ingolfsland, E. C., & Christiansen, S. P. (2023). Modifiable Risk Factors and Preventative Strategies for Severe Retinopathy of Prematurity. Life, 13(5), 1075.
- Nair, A., El Ballushi, R., Anklesaria, B. Z., Kamali, M., Talat, M., & Watts, T. (2022). A review on the incidence and related risk factors of retinopathy of prematurity across various countries. Cureus, 14(11).
- Anjaneyulu, k., Narendranatha, R., G., Ugandhar, R., B., Priya, R., K.(2023). Incidence and risk factors of retinopathy of prematurity: a clinical study conducted at teritiary care hospital. INDIAN JOURNAL OF APPLIED RESEARCH, 7(1).
- Yadav, R. Y. S., Rai, C., Srivastava, N., & Jhunjhunwala, A. To study the significance of various risk factors in development of retinopathy of prematurity at a tertiary care center in Eastern Uttar Pradesh.
- Yucel, O. E., Eraydin, B., Niyaz, L., & Terzi, O. (2022). Incidence and risk factors for retinopathy of prematurity in premature, extremely low birth weight and extremely low gestational age infants. BMC ophthalmology, 22(1), 367.
- Alka, G., Ashutosh, R., Astha, T. (2023). Associated risk factors of retinopathy of prematurity and its incidence in a tertiary care teaching hospital of eastern uttar pradesh.. INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH, 7(3), 5-7.
- Bhatnagar, A., Skrehot, H. C., Bhatt, A., Herce, H., & Weng,C. Y. (2023). Epidemiology of retinopathy of prematurity in the US from 2003 to 2019. JAMA ophthalmology, 141(5),479-485.
- Sabri, K., Ells, A. L., Lee, E. Y., Dutta, S., & Vinekar, A. (2022). Retinopathy of prematurity: a global perspective and recent developments. Pediatrics, 150(3).
- Shaik, R., & Chaitra, M. C. (2023). Prevalence, risk factors and severity of retinopathy of prematurity in preterm infants in a tertiary care hospital in rural Karnataka. Indian Journal of Clinical and Experimental Ophthalmology, 9(2), 232-240.
- Disha, N., Deepa, M., Tejaswini, K. (2023). Trends of retinopathy of prematurity in a tertiary care centre in urban India. INDIAN JOURNAL OF APPLIED RESEARCH, 8(5), 25-27.
- Sheth, N. R., Shah, M. P., Pandey, A., & Dubey, S. (2023). Retinopathy of prematurity-A clinical study of incidence and risk factors. Indian Journal of Clinical and Experimental Ophthalmology, 9(1), 103-111.
- Rizvi, S. A., Waris, A., Ali, S. M., Faizi, N., & Ahuja, P. (2022). Retinopathy of prematurity: Risk factors and associated co-morbidities. Panacea J Med Sci, 12(3), 503-9.
- Singh A. Guidelines for Universal Eye Screening in Newborns Including Retinopathy of Prematurity: Rashtriya Bal Swasthya Karyakram. Ministry of Health and Family Welfare. Government of India; 2017.
- Bhat, V., Patil, S. H., & Ashwini, S. (2022). Prevalence, patterns, and risk factors of retinopathy of prematurity in a tertiary care multispecialty hospital in North Karnataka. Journal of Clinical Ophthalmology and Research, 10(3), 114-117.
- Tekchandani, U., Katoch, D., & Dogra, M. R. (2021). Five-year demographic profile of retinopathy of prematurity at a tertiary care institute in North India. Indian Journal of Ophthalmology, 69(8), 2127-2131.
- Sahu, S. K., & Mishra, P. (2023). Challenge accepted: Retinopathy of prematurity (ROP) during COVID-19. Cureus, 15(2).
- Gour, R., Shende, S., Melwani, V., Singh, P., & Kumar, K. (2021). Pattern and risk factors of retinopathy of prematurity in tertiary care centre. Indian Journal of Clinical and Experimental Ophthalmology, 7(4), 695-698.
- Díaz-Coto, S., Corral-Blanco, N. O., & Martínez-Camblor,P. (2021). Two-stage receiver operating-characteristic curve estimator for cohort studies. The International Journal of Biostatistics, 17(1), 117-137.
- Huang, Y. P., Basanta, H., Kang, E. Y. C., Chen, K. J., Hwang,Y. S., Lai, C. C., ... & Wu, W. C. (2021). Automated detection of early-stage ROP using a deep convolutional neural network. British Journal of Ophthalmology, 105(8), 1099-1103.
- Kulida, E. L. (2018). A two-stage algorithm for generating aset of Pareto-optimal trajectories of an object. Advances in Systems Science and Applications, 18(1), 92-101.
- Prasad, Minali, Ellen C. Ingolfsland, and Stephen P. Christiansen. "Modifiable Risk Factors and Preventative Strategies for Severe Retinopathy of Prematurity." Life 13.5 (2023):1075.